CMB REVIEW FOR STEP I Prepared by Pamela

CMB REVIEW FOR STEP I: Prepared by Pamela L. Derstine, Ph. D. • Chromosome Organization • DNA Replication • DNA Repair • DNA Recombination • Cell Division February 13, 2003

Chromosome Organization

CLINICAL SIGNIFICANCE: 1. Most unrepaired mutations no effect. 2. Retrotransposon integration into genes 3. Retrotransposon mispairing over deletion or duplication inactivation unequal crossing disease. 4. Unequal crossovers of simple sequence repeats bordering chromosome regions microdeletion syndromes.

NF 1 Caused by Alu insertion Autosomal dominant 17 q 11. 2 Frequency 1: 3000 Also, skeletal deformities Predisposition to tumors of nervous system 50% new mutations

Review Problem #4, August 8, 2001 for data analysis

7 q 11 Microdeletion: Williams syndrome Autosomal dominant aortic stenosis Unusual face Joint laxity Mental disability Sensitivity to loud noises Strikingly happy personality Remarkable musical & language skills above mental function

DNA Replication

DNA Replication

DNA Replication

CLINICAL SIGNIFICANCE: Bloom’s Syndrome Helicase deficiency

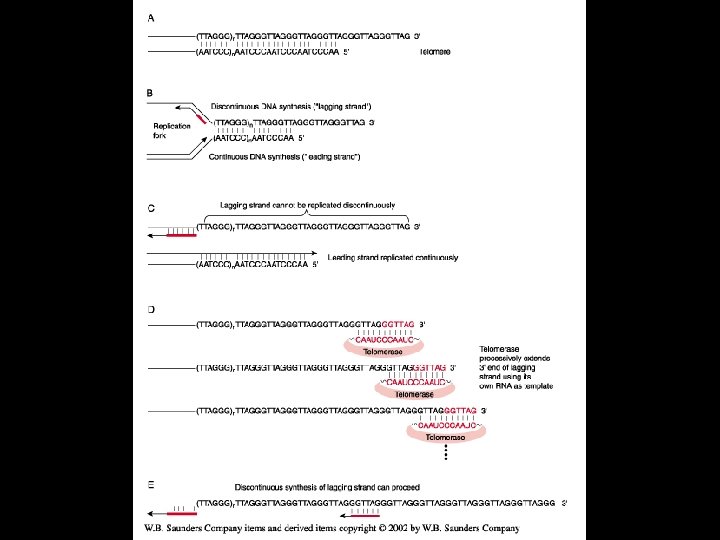
DNA Replication: telomeres

DNA Replication: telomerase

DNA Replication: telomerase

Clinical significance: Cancer or absent telomere due to progressive shortening with DNA replication

CLINICAL SIGNIFICANCE: CANCER SELF-RENWAL OF EPITHELIAL CELL POPULATION BY REPEATED CELL DIVISION Telomeres shorten and uncap Normal p 53 cell cycle checkpoint control Normal senescent cells stop dividing Loss of p 53 and cell cycle checkpoint control Mutant cell survives and proliferates Chromosome translocation Cell dies due to catastrophic genomic instability and DNA damage Chromosome fusion Chromosome breakage Chromosome bridge Massive chromosomal damage Telomerase reactivated CANCER CHROMOSOME BREAKGE-FUSIONBRIDGE CYCLE Chromosomes are partially stabilized and cell survives with many mutations

DNA damage, repair mechanisms and consequences

DNA REPAIR DURING REPLICATION: • DNA PROOFREADING • MISMATCH REPAIR

Proofreading
 recognizes")
MMR occurs close to the replication fork h. MSH 2/3 (Mut. S ) recognizes insertion or deletion loops h. MSH 2/6 (Mut. S ) recognizes mismatches, single-base loops h. MLH 1/h. PMS 2 (Mut. L ) binds to Mut. S and replication factors (determining strand specificity) Excision and resynthesis is carried out by exo and endonucelases, DNA pol / , RPA, PCNA
: no polyps Microsatellite instability")
CLINICAL SIGNIFICANCE: HNPCC Autosomal dominant inherited MMR mutation (multiple locations): no polyps Microsatellite instability LOH Additional mutations accumulate Colorectal Cancer: Tumor cells with almost normal karyotype

CLINICAL SIGNIFICANCE: HNPCC • Male heterozygotes: 90% lifetime colon cancer risk • Female heterozygotes: 70% lifetime colon cancer risk, 40% endometrial cancer risk • Other cancers • Accumulation of point mutations, microsatellite instability due to strand slippage during replication (replication error positive or RER+ phenotype)
")
RER Phenotype Testing (RFLP)

HNPCC vs FAP Familial adenomatous polyposis: autosomal dominant cancer; inherited mutation APC tumor suppressor gene (5 q 21 -q 22); early appearance of benign polyps Deletion or mutation of both copies of the tumor suppressor APC begins the process. Each polyp can develop into a carcinoma.

FAP

HNPCC vs FAP 5% population develops colorectal cancer Colorectal cancer: 11% total cancer deaths FAP: 0. 5% all colorectal cancers HNPCC: 3. 0% all colorectal cancers Sporadic: most colorectal cancers (DS DNA repair defects [translocations], cell division defects [nondisjunction])

DNA REPAIR POST-REPLICATION: • EXCISION REPAIR • DOUBLE-STRAND BREAK REPAIR

Excision Repair
 and XPF")
DNA damage recognition by XPC, XPA, RPA Coupled incisions by XPG (3’) and XPF (5’), generating a 2730 nucleotide fragment Helicase subunits of TFIIH (XPB, 3’-5’ and XPD, 5’-3’) unwind and release SS DNA fragment Repair synthesis by DNA polymerase / and the accessory proteins PCNA, RPA, ligase.

CLINICAL SIGNIFICANCE: XERODERMA PIGMENTOSUM Heterogeneous group of autosomal recessive skin disorders: sun-sensitivity, dryness and pigmentation of exposed skin, increased tendency to develop tumors Complementation

Double Strand Break Repair DNA damage checkpoint protein ATM activated Ku, DNA-PK proteins protect ends; mechanistic overlap with V(D)J recombination Phosphorylate p 53 to arrest cell cycle

CLINICAL SIGNIFICANCE: • NHEJ - increased radiosensitivity and immune deficiency when repair proteins inactive • HEJ – CANCER-PRONE CLINICAL SYNDROMES

Rec. BCD homologs generate DS DNA nicks and degrade both strands 5’-to-3’ Rec. A homologs (RAD 51) and accessory proteins (RPA, BRCA 1, BRCA 2) catalyze strand invasion and loop displacement Repair synthesis by DNA polymerases, PCNA, ligase, etc. Ruv. ABC homologs promote branch migration and resolution by strand cutting
")
Recombination; HEJ BIVALENT IN MEIOSIS OR SISTER CHROMATIDS (HEJ)
![CLINICAL SIGNIFICANCE OF DYSFUNCTIONAL HEJ: 1. Familial breast cancer (BRCA 1 [17 q 21],](http://slidetodoc.com/presentation_image/352fbe2ddfc8bb679bea2efc3bab3f6c/image-35.jpg "CLINICAL SIGNIFICANCE OF DYSFUNCTIONAL HEJ: 1. Familial breast cancer (BRCA 1 [17 q 21],")
CLINICAL SIGNIFICANCE OF DYSFUNCTIONAL HEJ: 1. Familial breast cancer (BRCA 1 [17 q 21], BRCA 2 [13 q 12. 3] mutation, autosomal dominant); one possible mechanism is shown. 2. Ataxia telangiectasia, an autosomal recessive, pleiotropic, variable disease due to mutations in ATM gene (11 q 23).

Cell Division

Clinical Significance: Cancer drug targets Taxol: binds, stabilizes microtubules Colchicine, colemid: binds subunits, prevents polymerization Vinblastine, vincristine: binds subunits, prevents polymerization Nocodozole: binds subunits, prevents polymerization

Clinical Significance: Cancer drug targets Motor protein inhibitors: example of Monastrol

Clinical Significance: Aneuploidy Trisomy 21: meiotic nondisjunction
")
Clinical Significance: Sporadic colorectal cancer (mitotic nondisjunction due to checkpoint malfunction)

Clinical significance: metaphase checkpoint malfunction Release from kinetochore Cdc 20 MAD 2
; Many")
Clinical Significance: LOH Rb 1 gene locus Retinoblastoma (autosomal dominant 13 q 14); Many common cancers. Review 9/17/01 problem set, #11.
- Slides: 42