Clusterin Expression Distinguish Follicular Dentritic Cell Tumor From

 • Tumor of dendritic cell lineage, including follicular dendritic cell tumor(FDCTs), interdigitating dentritic")
 • CD 21, CD 23, CD 35, CD 1 a and S 100")
 • Expression in benign follicular dendritic cell • Clusterin glycoprotein expressed in parenchyma")
 • Expression in anaplastic large cell lymphoma, diffuse large B cell lymphoma, peripheral")
 • Mayo Clinic in-house and consutation file, 1995~2003 • Follicular dendritic")
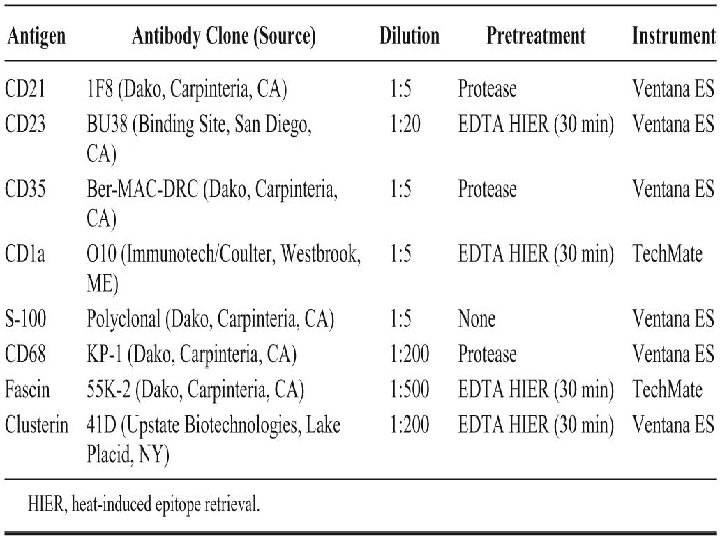
 • Paraffin embedded tissue: CD 21, CD 23, CD 35, CD")
 • EM was performed on selected case( 3 FDCT, 2 IDCT,")
 • FDCT: variable number of multinucleated tumor cells, intermixed inflammatory cell,")
 • IDCT: greater degree of nulclear pleomorphism, more polygonal cell with")
 • Clusterin diffuse strong cytoplasmic staining in all FDCT • Majority of FDCT")
 • 2 case of FDCTs were negative of CD 21, CD 23 and")
 • IDCT: negative or showed only focal weak positive for clusterin • All")
 • 6/14 LCH complete negative for clusterin and 8 cases showed variable positive")
 • 6 spindle cell tumor, NOS: all showed some degree of fascin, •")
 • Were performed in selected case( 3 FDCTs and 2 IDCTs) • FDCT:")
 • Unclassifiable spindle tumor: nonspecific features that lack membrane interdigitating process, intercellular junction,")
 • Follow-up clinical information was available in 9 FDCT(M: 58. 4 m)")
 • IDCT occurred in older adult • Four presented with solitary LN(+)")

 • The distinction of FDCT from other subtypes of dendritic cell tumor and")
 • Strong clusterin staining also distinguishes FDCTs from other dendritic cell neoplasm •")
 • CD 21 is thought to be the most reliable FDC marker with")
 • In addition to be a supplemental marker, clusterin staining can help classify")
 • IHC finding on 6 spindle cell tumor, NOS suggest that clusterin may")
 • Attempt to correlate clinicopathologic parameterw with clinical outcome have been limited by")
 • IDCTs display a variable behavior from benign to rapidly fatal dx •")

- Slides: 39
Clusterin Expression Distinguish Follicular Dentritic Cell Tumor From Other Dentritic Cell Neoplasm: Report of a Novel Follicular Dentritic Cell Marker and Clinicopathologic Data on 12 Additional Follicular Dentritic Cell Tumors and 6 Additional Interdigitating Dentritic Cell Tumors ~2004 AJSP August
Background(1) • Tumor of dendritic cell lineage, including follicular dendritic cell tumor(FDCTs), interdigitating dentritic cell tumor(IDCTs) and Langerhans cell histiocytoses(LCH), are rare • Share IHC positive for fascin, CD 68 and many morphologic features
Background(2) • CD 21, CD 23, CD 35, CD 1 a and S 100 distinguish them • D/D FDCTs and IDCTs is of clinical importance • CAN. 42, Ki-FDC 1 p, Ki-M 4 p, R 4/23 and desmoplakin
Clusterin(1) • Expression in benign follicular dendritic cell • Clusterin glycoprotein expressed in parenchyma cells of liver, stomah and brain • Complement fixation, membrane protection, cell aggregation, cell-matrix interaction, lipid transport, apoptosis, stress –induced secreted chaperone protein
Clusterin(2) • Expression in anaplastic large cell lymphoma, diffuse large B cell lymphoma, peripheral T-cell lymphoma, nodular sclerosis Hodgkin lymphoma, ca of breast, colon, pancreas, and prostate • Expression on dentritic cell tumor has not previously been reported • Substantial number
Material and method(1) • Mayo Clinic in-house and consutation file, 1995~2003 • Follicular dendritic cell sa/tumor, interdigitating dendritic cell sa/tumor, dendritic cell, NOS • FDCT: 20>>>> 12 • IDCT: 9>>>> 6 • DCT, NOS: 5>>>> 3>>>6 • LCH: 3+11
Material and method(2) • Paraffin embedded tissue: CD 21, CD 23, CD 35, CD 1 a, S 100, CD 68, fascin and clusterin were applied • Selected case: additional IHC marker were applied • Positive of clusterin was scored both quantitatively(0~4) and qualitatively
Material and method(3) • EM was performed on selected case( 3 FDCT, 2 IDCT, 6 spindle cell tumor, NOS) • Clinical data and f/u information were obtained in FDCT and IDCT cases from Mayo Clinic patient redords or discussion with the referring physcians
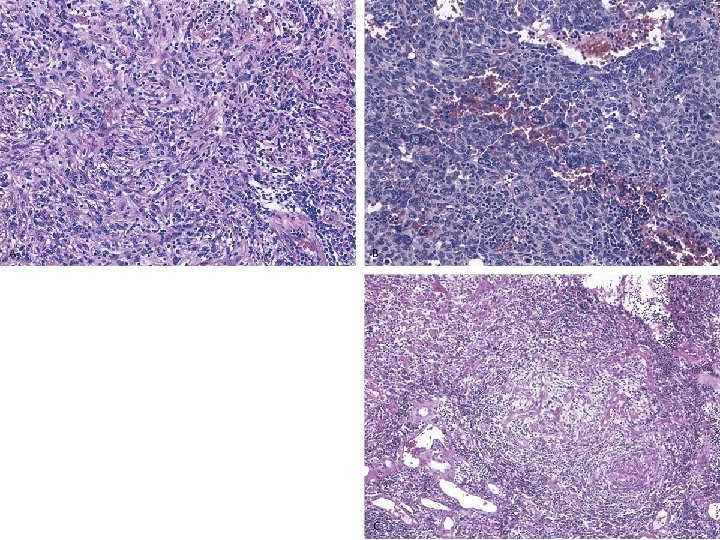
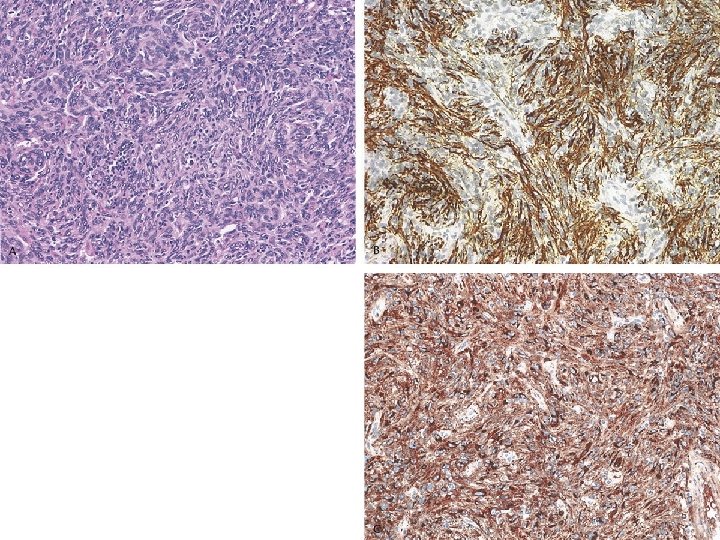
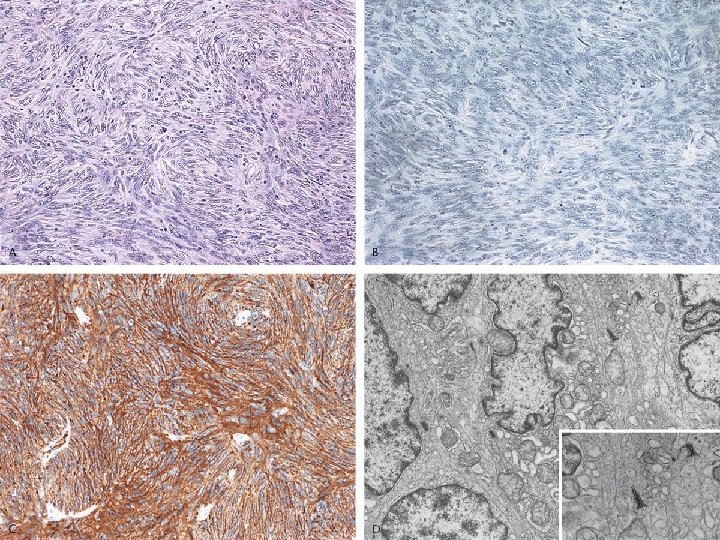
Result histological feature(1) • FDCT: variable number of multinucleated tumor cells, intermixed inflammatory cell, centered in the cortical region of LN, • Myxoid change, pseudovascular space, dense fibrosis, angiofollicular hyperplasia, necrosis • Mitoses: 0~34/10 hpf(M: 11. 4)
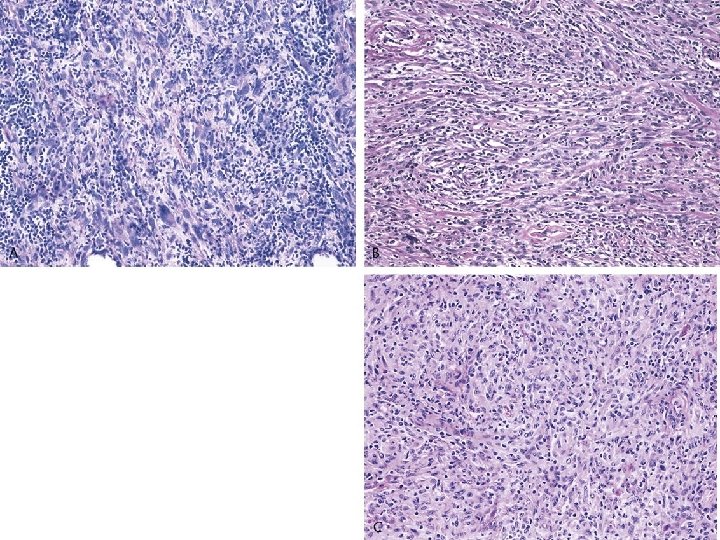
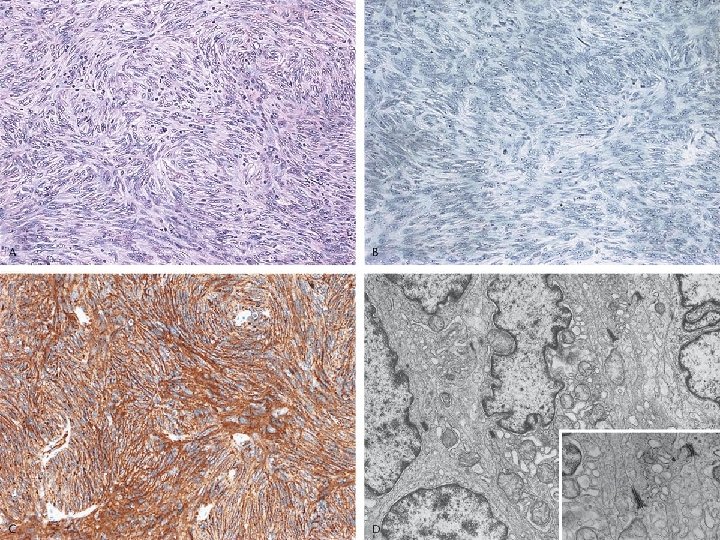
Result histological feature(2) • IDCT: greater degree of nulclear pleomorphism, more polygonal cell with more abundant eosinophilic cytoplasm • Paracortical distribution • 2 case: histiocyte like • Intermixed lymphoplasmacytic population and multinucleated tumor giant cell • Mitose: 0~19/10 hpf (M: 7. 5) • necrosis
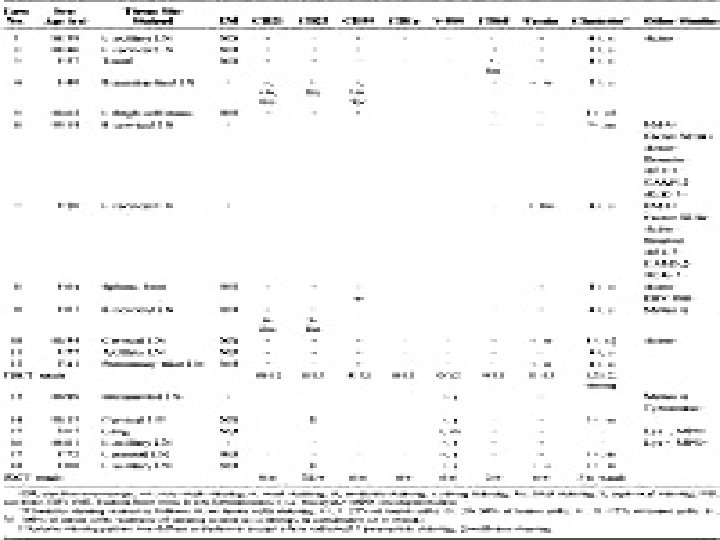
IHC(1) • Clusterin diffuse strong cytoplasmic staining in all FDCT • Majority of FDCT showed positive for one or more of the tranditional FDC marker • CD 1 a and S-100 were negative in all FDCT • CD 68 and fascin were positive in the majority
IHC(2) • 2 case of FDCTs were negative of CD 21, CD 23 and CD 35, were classified as FDCT by EM • Negative for actin, desmin, ALK-1, CK, CAM 5. 2 • Both show positive for EMA
IHC(3) • IDCT: negative or showed only focal weak positive for clusterin • All IDCT were strongly positive for S-100, fascin and negative for CD 1 a, CD 21, CD 35 • Subset case shows CD 23 and CD 68 positive
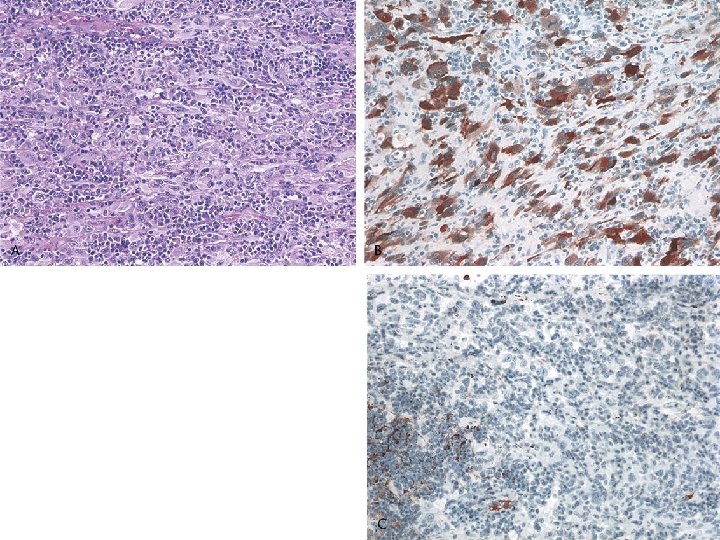
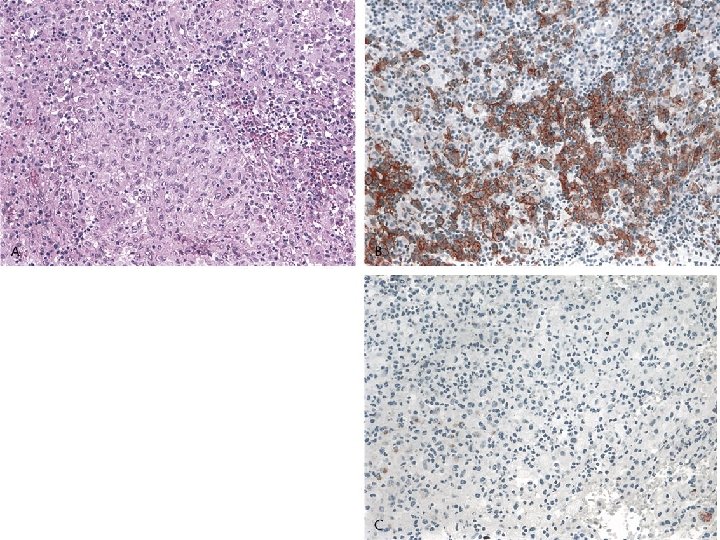
IHC(4) • 6/14 LCH complete negative for clusterin and 8 cases showed variable positive • All LCH were positive for CD 1 a, fascin and CD 68 • S-100 showed variable intensity in 13 cases • CD 21, CD 35 were negative in all cases • CD 23: equivocal in 9 cases
IHC(5) • 6 spindle cell tumor, NOS: all showed some degree of fascin, • 2 showed strong culsterin in the minor subset of cells • Others: negative
EM(1) • Were performed in selected case( 3 FDCTs and 2 IDCTs) • FDCT: long interwining process connected by well-formed desmosome • IDCT: complex interdigitating process without intercellular junction, variable number of lysosome and intermediate filament
EM(2) • Unclassifiable spindle tumor: nonspecific features that lack membrane interdigitating process, intercellular junction, dense bodies and basal lamina
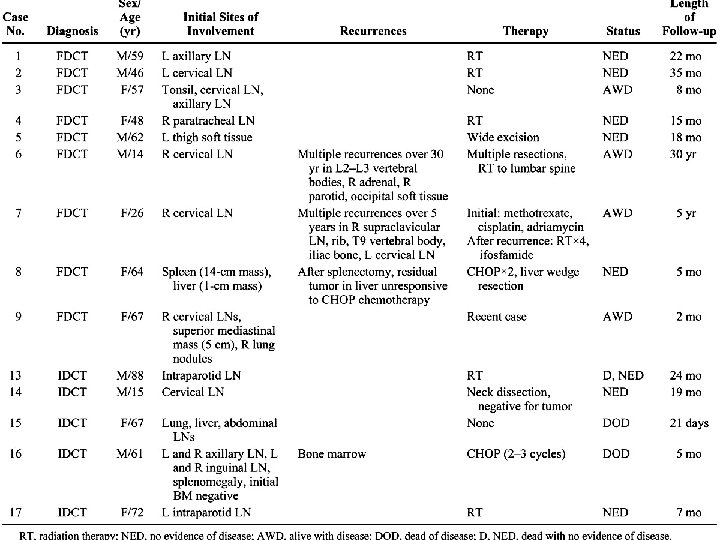
Clinical feature(1) • Follow-up clinical information was available in 9 FDCT(M: 58. 4 m) • 4 achieved apparent cure • meta was noted in 5 cases • None of the patient with FDCT is known to have died
Clinical feature(2) • IDCT occurred in older adult • Four presented with solitary LN(+) • Follow up clinical information was avaiable in 5 IDCT cass • Three achieved apparent cure • Two presented with disseminated dx and progressed rapidly to death from their dx
Clinicopathological Correlation • No apparent correlation of behavior of FDCT or IDCT with mitotic activity, necrosis, degree of atypia or tumor location • The two very aggressive IDCT had very similar histiocyte-like morphology and CD 68(+) that was distinct from the other three cases
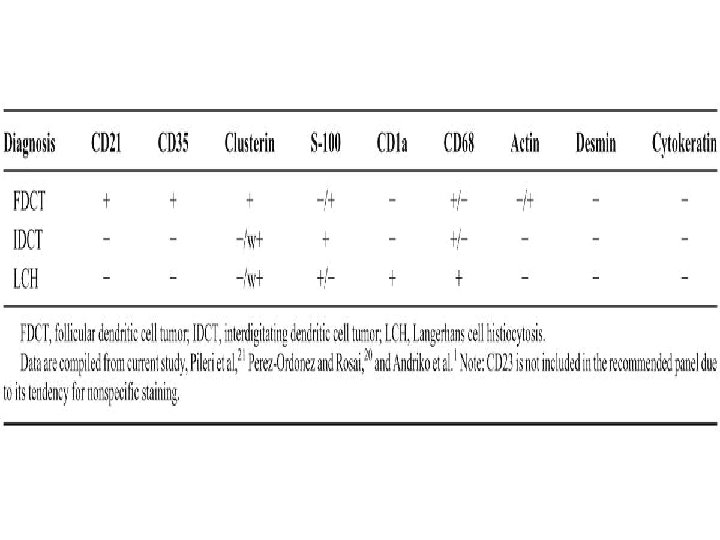
Discussion(1) • The distinction of FDCT from other subtypes of dendritic cell tumor and other spindle cell tumor requires a panel of IHC stain(CD 21, CD 23, CD 35, S-100, CD 1 a, CD 68, actin, desmin and CK) • we demonstrate the additional marker, clusterin, increases the diagnostic sensitivity
Discussion(2) • Strong clusterin staining also distinguishes FDCTs from other dendritic cell neoplasm • Robust clusterin staining is useful as supportive evidence for FDCT in cases with weak or focal expression of the extablished FDC markers
Discussion(3) • CD 21 is thought to be the most reliable FDC marker with a sensitivity of 96% • Weak and focal staining is a particular problem in hepatosplenic FDCT cases with an inflammatory pseudotumor-like morphology • Some have used CD 21 and CD 35 cocktail or additional marker(Ki-FDC 1 p, Ki-M 4 p, CAN. 42, R 4/23)
Discussion(4) • In addition to be a supplemental marker, clusterin staining can help classify FDCT that is completely devoid of staining for these traditional marker • Strong clustrin expression shows specificity for FDCTs among dendritic cell tumor
Discussion(5) • IHC finding on 6 spindle cell tumor, NOS suggest that clusterin may not be entirely specific for FDCTs among all spindle cell tumor • The clinical finding in our cases supplement previous report, behave as low gr sarcoma, with tendency for local recurrence and late metastases, some with castleman dx
Discussion(6) • Attempt to correlate clinicopathologic parameterw with clinical outcome have been limited by the rarity of the tumor • One previous study of 17 FDCTs found a statistically significant correlation between intraabdominal location, significant pleomorphism and a worse outcome
Discussion(7) • IDCTs display a variable behavior from benign to rapidly fatal dx • No apparent association between mitoses, necrosis, nuclear pleomorphism or extranodal location • It’s interesting to speculate that IDCTs displaying more histiocytic differentiation may be associated with more aggressive behavior
Conclusion • IHC for clussterin is of significant utility in diagnostic evaluation of dendritic cell tumor • Strong clusterin stain appears to be a highly sensitive marker of FDCT • Additional study is needed to delineate the specificity of clusterin expression among a broader spectrum of sarcoma and other spindle cell tumor