Cluster Headache Anish Bahra The National Hospital for

Cluster Headache Anish Bahra The National Hospital for Neurology and Neurosurgery Whipps Cross University Hospital

Classification of Headache Disorders 1. Migraine 2. Tension-Type Headache 3. Trigeminal Autonomic Cephalalgias 4. Other Primary Headaches

Trigeminal Autonomic Cephalalgias • Cluster Headache • Paroxysmal Hemicrania • SUNCT Short-lasting Unilateral Neuralgiform attacks Conjunctival injection & Tearing Goadsby PJ, Lipton RB. Brain 1997; 120: 193 -209

1. Migraine 15 -18% 2. Tension-Type Headache 3. 1 Cluster Headache 0. 1% 3. 2 3. 3 4. 1 Paroxysmal Hemicrania SUNCT Stabbing Headache Less 4. 2 4. 3 Cough Headache Exertional Headache 4. 4 4. 5 Sexual Headache Hypnic Headache 4. 6 Thunderclap Headache 4. 7 Hemicrania Continua 4. 8 New persistent Daily Headache ~ 60 -80%

Diagnosis of Cluster Headache
 • Ipsilateral")
Trigeminal Autonomic Cephalalgias • Strictly unilateral head and facial pain (V 1) • Ipsilateral autonomic features • Short-lived attacks • Multiple daily attacks • Active bouts and remissions / no remissions

% Cluster Headache – Laterality

• • Retro-orbital Temporal Upper teeth Forehead 92 % 70 50 46 • • • Jaw 45 Cheek Lower teeth Neck Nose Ear 17 Shoulder Vertex Occiput Parietal 45 32 31 20 13 7 6 1 Bahra A et al. Neurology 2002; 58: 354 -361

Autonomic Features N 2301 1802 1053 • Lacrimation % 91 84 86 • Conjunctival injection 77 58 88 • Nasal congestion 75 48 71 • Rhinorrhoea 72 43 - • Ptosis / Eye-lid swelling 74 57 - 1. 2. 3. Bahra A et al. Neurology 2002; 58: 354 → Prospective Manzoni et al. Cephalagia 1983; 3: 21 Ekbom. Acta. Neurol. Scand. 1970; 46 (suppl. 41)

Ipsilateral autonomic features • • • Conjunctival injection Lacrimation Nasal congestion Rhinorrhea Eye-lid oedema Forehead & facial sweating • Ptosis and miosis Parasympathetic Sympathetic
 • Ipsilateral")
Trigeminal Autonomic Cephalalgias • Strictly unilateral head and facial pain (V 1) • Ipsilateral autonomic features • Short-lived attacks • Multiple daily attacks • Active bouts and remissions / no remissions

Attack Duration and Frequency N 1802 4233 Duration 30 -120 Freq/day <1 to >5 1054 30 -120 2/wk to >8/day < 30 -180 <1 to >3
 • Ipsilateral")
Trigeminal Autonomic Cephalalgias • Strictly unilateral head and facial pain (V 1) • Ipsilateral autonomic features • Short-lived attacks • Multiple daily attacks • Episodic / Chronic

Cluster Headache : Active Bouts & Remissions Episodic Cluster Headache 7 days - One year Pain-free interval ≥ one month Chronic Cluster Headache ≥ one year without remission ≥ one year with remissions one month * Interictal pain

Bouts per year ar ye 4/ ar ye 3/ ar ye 2/ ar ye 1/ 18 ery Ev Ev ery 2 y /12 rs N (230) Bahra et al. Neurology 2002

Other Distinctive Features • Restlessness • Periodicity – Diurnal and Seasonal • Alcohol Triggering

 Month Kudrow (1987) Headache")
Cluster period onsets (n) Month Kudrow (1987) Headache
 and")
Cluster Headache Attack Provocation • 1 mg s/l nitroglycerine provocation • During (n=28) and out (n=15) of active bout • Attack precipitated in ALL during active bout • No attack precipitated out of the bout Ekbom, K. Arch Neurol 1968; 19: 487

Cluster Headache Severe unilateral orbital, supraorbital and/or temporal pain Conjunctival injection Lacrimation Nasal congestion Rhinorrhea Eye-lid oedema Forehead & facial sweating Ptosis and miosis 15 min to 3 hours attack duration 1 / alternate days - 8 attacks / day ~ Daily 7 days - 1 yr with ≥ one month remission (~ 90%) A sense of restlessness / agitation

Differential Diagnosis of Cluster Headache

Differential Diagnosis Migraine CH PH SUNCT Trigeminal Neuralgia

Strictly unilateral Nausea Vomiting Motion Photophobia Phonophobia Aura Lacrimation Conjunctival injection Nasal Congestion Rhinorrhoea Migraine CH 30 82 50 99 45 20 ~ 90 83 86 ~ 90 60 30 80 44 24 25 22 18 95 62 45 65 Rasmussen 1991, Ekbom 1970

Strictly unilateral Nausea Vomiting Motion Photophobia Phonophobia Aura Lacrimation Conjunctival injection Nasal Congestion Rhinorrhoea Migraine CH 30 82 50 99 45 20 ~ 90 83 86 ~ 90 60 30 80 44 24 25 22 18 95 62 45 65 Rasmussen 1991, Ekbom 1970

Symptomatic Cluster Headache • Aneurysm of the ACA • Pituitary tumour • AVM of the occipital lobe • Aneurysm of the vertebral artery • Meningioma of the cervical canal (C 2)

Any one → Sensitivity 98. 6% & specificity 34. 4% Likelihood Ratio Age > 50 years* 2. 34 Sudden Onset* 1. 74 Predictors of Secondary Headache * Abnormal neurological examination* 3. 56 Additional Features 2. 27 Locker at al. Headache. 2006 ( n = 558) / Ramirez-Lassepas. Arch Neurol. 1997

N

Treatment of Cluster Headache

Abortive Therapy : Sumatriptan 6 mg sc • Modest > benefit from 12 mg • 2 & 3 mg are effective 74 • No prophylactic benefit 26 • Long term - Well tolerated. • No medication overuse The Sumatriptan Cluster Headache Study Group -1991

Abortive Therapy : Oxygen • Oxygen 100% 12 l/min • Mask holes covered 78 • For multiple daily attacks • Safe but impractical 20 • http: //www. impressresp. com/ ‘Rationalising oxygen use to improve patient safety and reduce waste’ Cohen 2007
 Zolmitriptan 5 and 10 mg IN (A/B)")
ABORTIVE THERAPY Sumatriptan 20 mg IN (A) Zolmitriptan 5 and 10 mg IN (A/B) Zolmitriptan 5 and 10 mg po (B) Lidocaine IN (B)
 Zolmitriptan 5 and 10 mg IN (A/B)")
ABORTIVE THERAPY Sumatriptan 20 mg IN (A) Zolmitriptan 5 and 10 mg IN (A/B) Response at 30 minutes Zolmitriptan 5 and 10 mg po (B) Lidocaine IN (B)

PREVENTATIVE THERAPY : VERAPAMIL • 240 – 960 mg daily – Lethargy • Start at 80 mg tds – Constipation • 40 -80 mg increments every 10 -14 days – Pedal oedema • ECG monitoring every two weeks – Bradycardia Leone et al. (2000) Neurology ; 54 : 1382
 Dose ±SD Patients on VPM")
Verapamil in Cluster Headache Arrhythmias No Patients Mean VPM(mg) Dose ±SD Patients on VPM 217 512 ± 279 ECGs 108 587 ± 264 1° Heart Block 13 578 ± 264 Other HB 9 604 ± 260 Total arrhythmias 21 567 ± 290 PR ≤ 0. 2 s 9 653 ± 275 Cohen, 2007

PREVENTATIVE THERAPY : METHYSERGIDE • 3 -6 mg : Increase in one week • Then 1 mg / week – Nausea and vomiting – Abdominal discomfort – Vasoconstrictive effects – Organ Fibrosis • Up to 12 mg daily • BNF – 6 months then drug holiday Weight gain Muscle cramps Mood changes

Preventative Therapy : Lithium • Tremor • GI side effects • ↓ thyroid, euthyroid goitre • Ataxia, nystagmus, dysarthria • Diabetes Insipidus • Caution re Drug Interactions

Preventative Therapy : Lithium • 600 -1500 mg • Level at 4/7 after dose change • Weekly until dose constant for 4 weeks • Then 3 monthly • 0. 7 -1. 2 mmol/l • Normal renal function and Na+ (Li toxicity)

Preventative Therapy : Corticosteroids Short-term use for multiple daily attacks Attacks recur once the dose is decreased • 40 -80 mg for 5 – 7 days • Taper thereafter over 2 weeks • Simultaneously introduce a suitable prophylactic Jammes (1975) Dis. Nerv. Syst. ; 36 : 375
 • Ergotamine tartrate (B) • Valproic acid (C) •")
Preventative Therapy • Topiramate (B) • Ergotamine tartrate (B) • Valproic acid (C) • Melatonin (C) • Gabapentin (C) • Pizotifen (C) EFNS Guidelines for the Management of Cluster Headache 2006

Preventative Therapy • Topiramate 800 mg • Ergotamine tartrate 10 mg • Valproic acid 2 g • Melatonin 15 mg • Gabapentin 3. 6 g • Pizotifen 4 mg

Surgical Therapy • Trigeminal ganglion and nerve • Sphenopalatine ganglion • Greater superficial petrosal nerve • Nervus intermedius • Greater Occipital Nerve • Hypothalamus

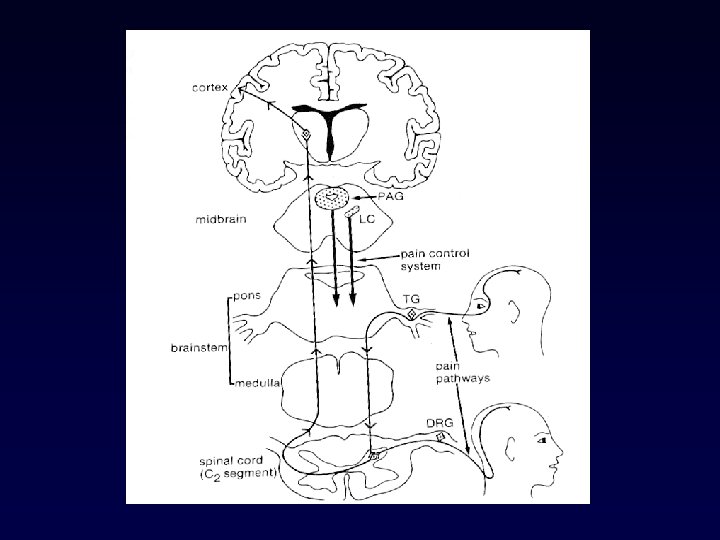
Cervicotrigeminal Modulation

Greater Occipital Nerve Block Patients N=23 Treatment Group Placebo Complete response at 1/52 11 None Complete response at 4/52 8 None Ambrosini et al. Pain (2005) Patients (N) No. Injections Complete response (N) Partial Response (N) 19 22 10 3 Mean 17 days Mean 52 days AUDIT. Afridi et al. Pain 2006

Occipital Nerve Stimulation Cluster Headache Improvement Burns et al. Lancet, 2007

Cluster Headache - Stereotactic Stimulation of the Posterior Hypothalamic Gray Matter May et al. (1998) Lancet ; 352 : 275 Leone et al. (2001) NEJM ; 345 : 1428

Cluster Headache: Summary Acute • Strictly unilateral head pain + autonomic features • Sc Sumatriptan (A) • 15 -180 mins & daily Prevention • Restless during attacks • Woken early hours a. m • Active bouts & remissions • High flow oxygen (A) • Verapamil (A) • Methysergide (B) • Lithium (B) • Steroids (A) • Topiramate (B) • Occipital nerve block
 • High flow oxygen (A) Prevention")
Cluster Headache: Summary Acute • Sc Sumatriptan (A) • High flow oxygen (A) Prevention • Verapamil (A) • Methysergide (B) • Lithium (B) • Steroids (A) • Topiramate (B) • Occipital nerve block
- Slides: 48