Clotting Hemostasis Anticoagulation Do Dr Jale oban Topics

Clotting, Hemostasis, Anticoagulation Doç. Dr. Jale Çoban

Topics 1 - Hemostasis overview 2 - Coagulation 3 - Bleeding / thrombosis 4 - Laboratory tests 5 - Patient samples

Hemostasis Clot Formation Clot Dissolution The balance between clotting and bleeding Components of Hemostasis: – Vasculature – Coagulation proteins – Platelets
 is the stoppage of bleeding, which is vitally important when blood")
Hemostasis („hemo”=blood; sta=„remain”) is the stoppage of bleeding, which is vitally important when blood vessels are damaged. Following an injury to blood vessels several actions may help prevent blood loss, including: Formation of a clot

PHASES OF THE HEMOSTATIC PROCESS • Initiation and formation of the platelet plug • Propagation of the clotting process by the coagulation cascade • Termination of clotting by antithrombotic control mechanisms • Removal of the clot by fibrinolysis
")
Local vasoconstriction • is due to local spasm of the smooth muscle (symp. reflex) • PLT comming in contact with exposed collagen release: serotonin, ADP, TXA 2, which accelerate vasoconstriction and causes PLT to swell and become more sticky

Formation of a platelet plug. When blood platelets adhere to collagen in the wall of a defective blood vessel, they release ADP and synthesize thromboxane A 2. These substances increase the adhesiveness of the platelets, causing more platelets to aggregate at the site of injury .

The functional response of activated platelets involves four different processes: 1. Adhesion — the deposition of platelets on the subendothelial matrix 2. Aggregation — platelet-platelet cohesion 3. Secretion — the release of platelet granule proteins 4. Procoagulant activity — the enhancement of thrombin generation

• This process is facilitated by a plasma glycoprotein, von Willebrand factor (v. WF). Produced in both endothelial cells and platelets, v. WF forms bridges between receptors on the surface of platelets and collagen fibers in the connective tissue.
")
Formation of platelet aggregate • Injured blood vessel releases ADP, which attracts platelets (PLT) • PLT comming in contact with exposed collagen release: serotonin, ADP, TXA 2, which accelerate vasoconstriction and causes PLT to swell and become more sticky

Formation of blood clot • In the formation of the clot, an enzyme called thrombin converts fibrinogen into insoluble protein, fibrin • Fibrin aggregates to form a meshlike network at the site of vascular damage
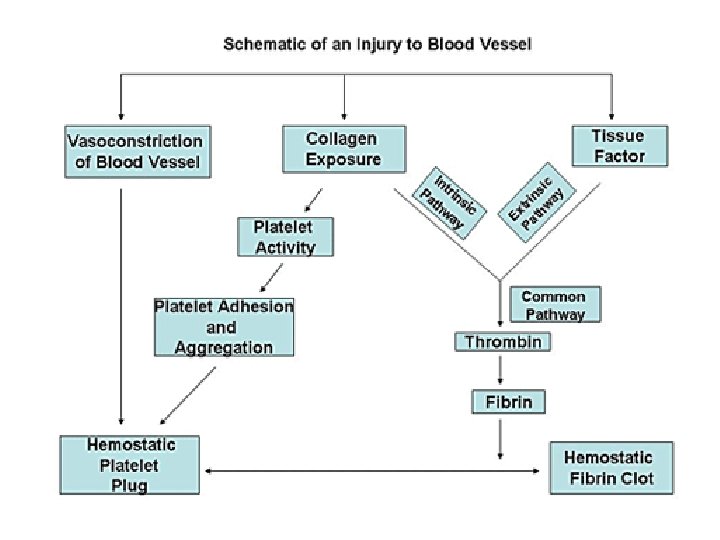

CLOTTING CASCADE AND PROPAGATION OF THE CLOT The clotting cascade is depicted as consisting of an intrinsic and extrinsic pathway.
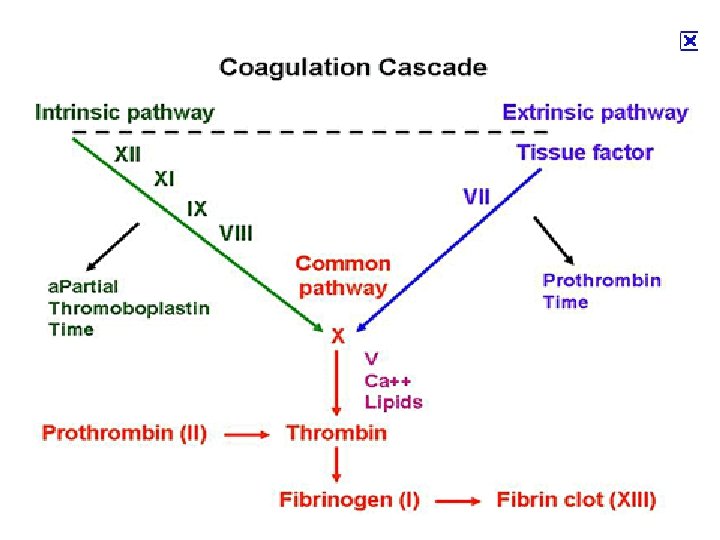

Extrinsic pathway: Ca 2+ Christmas factor Antihemophilic factor Stuart factor Stage I: Formation of prothrombin activator 1. When blood comes in contact with injured tissue – tissue thromboplastin (F III) interacts with (F VII), and Ca 2+ activating (F X).
. Activated F XII Ca Christmas activates")
Intrinsic pathway: 2. Exposed collagen activates (F XII). Activated F XII Ca Christmas activates plasma enzyme factor – plasma thromboplastin antecedent (PTA; F XI, Antiwhich in the presence of hemophilic Ca 2+ activates (F IX). F factor IX interacts with (F VIII), Ca 2+ to form a complex that activates (F Stuart factor X). 2+ Stage I: Formation of prothrombin activator

Ca 2+ Christmas factor Antihemophilic factor 3. Common pathway: Stage I: Formation of prothrombin activator Activated F X in the presence of Ca 2+ forms complexes with accelerin (F V) to form prothrombin activator

Stage II: conversion of prothrombin to thrombin Ca 2+ • Prothrombin – inactive precursor of enzyme thrombin • In the presence of prothrombin activator and Ca 2+ prothrombin is converted to thrombin • Thrombin itself increases its own rate of formation (positive feedback mechanism)

Stage III: conversion of fibrinogen to fibrin-stabilizing factor • Fibrinogen – plasma protein produced by the liver • Thrombin converts fibrinogen to fibrin • Thrombin also activates fibrin-stabilizing factor (F XIII), which in the presence of Ca 2+, stabilizes the fibrin polymer through covalent bonding of fibrin monomers

2+ Ca Calcium ions • Are required for promotion and acceleration of almost all blood clotting reactions • Except: activation of XII and XI (intrinsic mechanism)

Fibrinolysis

Clot Dissolution 1. Plasmin is formed from plasminogen - enzyme called activator (e. g. enzymes from urine, tears, saliva or bacterial enzyme streptokinase) 2. Plasmin as an enzyme is involved in breaking down fibrin into soluble fragments (fibrinolysis) Plasminogen t-PA Fibrin Plasmin soluble fragments

Anticoagulants Hirudo medicinalis produce Hirudin that inhibits Thrombin

Anticoagulants • Although tissue breakdown and platelets destruction are normal events in the absence of trauma, intravascular clotting does not usually occur because: - the amounts of procoagulants released are very small - natural anticoagulants are present (Antithrombin III, Heparin, Antithromboplastin, Protein C and S, fibrin fibers)

Natural anticoagulants • Antithrombin III – inhibits factor X and thrombin • Heparin from basophils and mast cells potentiates effects of antithrombin III (together they inhibit IX, X, XII and thrombin) • Antithromboplastin (inhibits „tissue factors” – tissue thromboplastins) • Protein C and S – activated by thrombin; degrade factor Va and VIIIa

n n - - Severe reduction in the number of PLTs thrombocytopenia this causes spontaneous bleeding as a reaction to minor trauma in the skin - reddishpurple blotchy rash it may result from: decreased production (toxins, radiation, infection, leukemias) increased destruction (autoimmune processes) increased PLTs consumption (DIC) Thrombocytopenia Hemorrhagic spots (petechiae)

Hepatic failure • Most of the clotting factors are formed in the liver Subconjunctival hemorrhage
 • Widespread coagulation thrombosis in small blood vessels increased fibrinolysis,")
Disseminated intravascular coagulation (DIC) • Widespread coagulation thrombosis in small blood vessels increased fibrinolysis, and depletion of coagulating factors generalized bleeding • It may result from: - bacterial infections damage) - disseminated cancers (release of procoagulants) - complications of pregnancy - severe catabolic states (endothelial Disseminated cervical cancer metastases (PET imaging)
 and B (lack of F IX) are transmitted")
Hemophilia A (lack of F VIII) and B (lack of F IX) are transmitted genetically and affect only males. Females carry the gen but do not show symptoms. Von Willebrand’s disease – loss of large component of f. VIII
 • Spontaneous or traumatic subcutaneous bleeding •")
Hemophilia A (lack of F VIII; 85%) • Spontaneous or traumatic subcutaneous bleeding • Blood in the urine • Bleeding in the mouth, lips, tongue • Bleeding to the joints, CNS, gastrointestinal tract Mild hemophilia after injection in buttock

Tests of coagulation
 � PROTHROMBIN TIME (PTT) �")
LABORATORY EVALUATION � PLATELET COUNT � BLEEDING TIME (BT) � PROTHROMBIN TIME (PTT) � PARTIAL THROMBOPLASTIN TIME (a. PTT) � THROMBIN TIME (TT)

PLATELET COUNT � NORMAL 150, 000 - 400, 000 CELLS/MM 3 < 100, 000 Thrombocytopenia 50, 000 - 100, 000 < 50, 000 Mild thrombocytopenia Sev Thrombocytopenia

Bleeding time • The blleding time is intennded to measure platele function, but it is neither a sensitive nor a spesific test. • Platelet counts < 100. 000/u. L, aspirin, other platelet inhibitory drugs can prolong the bleeding time • Tne bleeding time can be prolonged in von Willebrand disease and other hereditary plateled function disorders.

Bleeding time – procedure: • A trained healtcare professionall makes a small incision on the patient’s arm, and every 30 sec. Gently blots the blood with filtter paper to see if the bleeding has stopped. The filter paper must not touch the wound. Prior to making the cut, a blood pressure cuff is placed on the patient’s arm at 40 mm. Hg. • Referance İnterval : 1 - 9 min. This may vary from lab to lab, depending on how the test is measured

n n n The time taken for blood to clot mainly reflects the time required for the generation of thrombin The surface of the glass tube initiates the clotting process. This test is sensitive to the factors involved in the intrinsic pathway The expected range for clotting time is 4 -10 mins. Whole blood clotting time

Whole blood clotting time – procedure: • Clean the tip of the finger with an alcohol • Prick the finger tip with an automatic lancet • Note the time when blood first appears on the skin • Touch the tube to the drop of blood • Break gently 1 cm of the tube at the end of 2 min, and every 30 sec these after • When fibrin is formed between the two broken pieces of tube the coagulation or clotting time is noted

"Intrinsic" and "extrinsic" coagulation pathways Activated Partial Thromboplastin Time N: 25 -35 sec Prothrombin Time: 12 – 14 sec
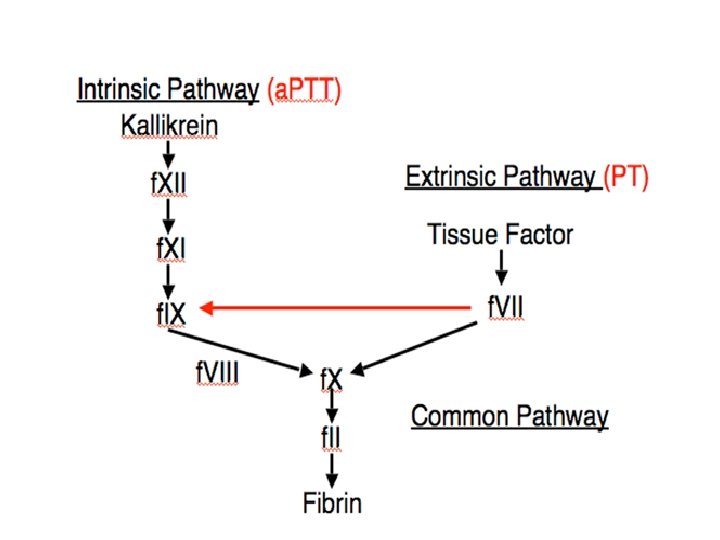

• The intrinsic pathway is initiated by the exposure of blood to a negatively charged surface (such as celite, kaolin, or silica in the in vitro activated partial thromboplastin clotting time [a. PTT]). • The extrinsic pathway is activated by tissue factor exposed at the site of injury or tissue factor-like material (thromboplastin, TPL in the in vitro prothrombin clotting time [PT]).
 • The PT measures the clotting time from factor VII through")
Protrombin Time (PTT) • The PT measures the clotting time from factor VII through fibrin formation(extrinsic and common pathways). • PT prolangations caused by: 1. factor deficiencies involoving -fibrinogen -factor II (protrombin) -factor VII -factor X 2. therapeutic anticoagulans Warfarin (Coumadine) 3. Lupus anticoagulants or by spesific factor inhibitors against Fibrinogen or factor II, V, VII or X
 • PT reagents is called thromboplastin (phospholipid with tissue factor and")
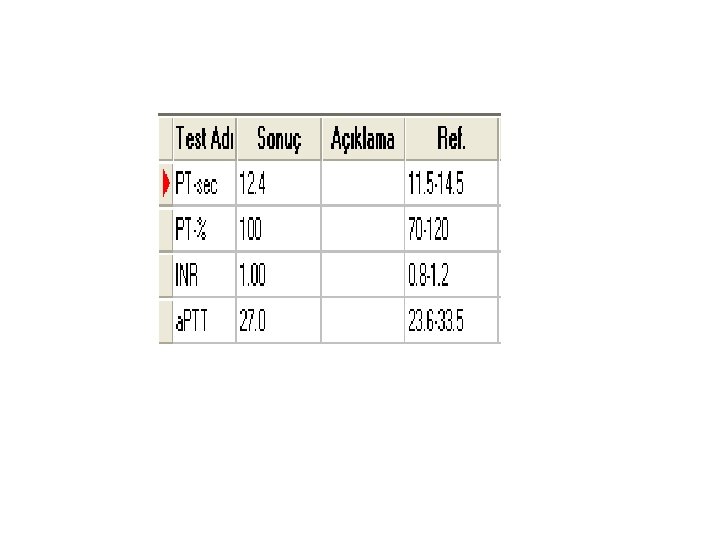
Protrombin Time (PTT) • PT reagents is called thromboplastin (phospholipid with tissue factor and Ca++). It is added to patient plasma, and the time until clot formation is measured in seconds (Referans interval: 12 -14 sec). • Tissue factor activates the extrinsic pathway. Phospholipid and Ca++ are required cofactors in the coagulation cascade. • Citrate in the blue top tube prevents clotting by chelating Ca++ • Prolonged PT: - a vitamin K deficiency (vitamin K is a co-factor in the synthesis of functional factors II prothrombin), VII, IX and X) - liver disease - Warfarin therapy (Coumadin)
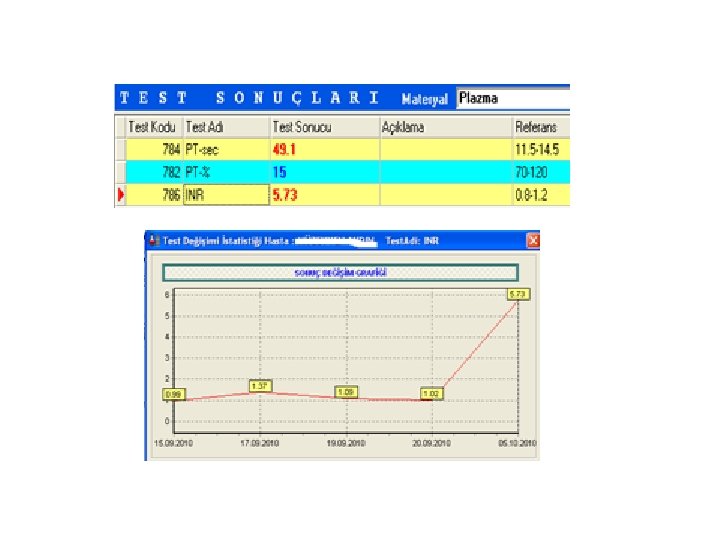
 • Warfarin is monitored by the international normalized ratio (INR) •")
Monitoring Warfarin (coumadin) • Warfarin is monitored by the international normalized ratio (INR) • The usual therapeutical goal is an INR of 2 -3.
 • INR is calculated from the PT and is intended")
International Normalised Ratio (INR) • INR is calculated from the PT and is intended to allow valid comparisons of results regardless of the type of PT reagent used among different laboratories: INR=(patient PT / mean normal PT)ısı • International sensitivity index(ısı) is a measure of the sensitivity of a particular PT reagent. Different PT reagents have different sensitivities to factor deficiencies.
 test result expressed as a ratio to")
• A patient’s prothrombin time (PT) test result expressed as a ratio to a normal population control which has been standardized (or normalized) for the potency to the thromboplastin used in the assay. • It is standardized using a World Health Organization (WHO) international reference thromboplastin preparation, and determined using the equation: INR = R^ISI, where R is the PT ratio obtained with the working thromboplastin.
 • The result for the PT is expressed as a")
International Normalised Ratio (INR) • The result for the PT is expressed as a ratio (prothrombin clotting time for patient plasma divided by time for control plasma); • Correction factor (International Sensitivity Index) is applied to the prothrombin ratio and the result issued as INR. • Therapeutic interval: Therapeutic interval for oral anticoagulant therapy: 2. 0 -4. 5. • Application: Monitoring oral anticoagulant therapy (eg. Warfarin); • note that heparin will not prolong INR (heparinase is included within the INR reagent)!!!!!!! For heparin therapy we monitor a. PTT and/or a. PTT ratio
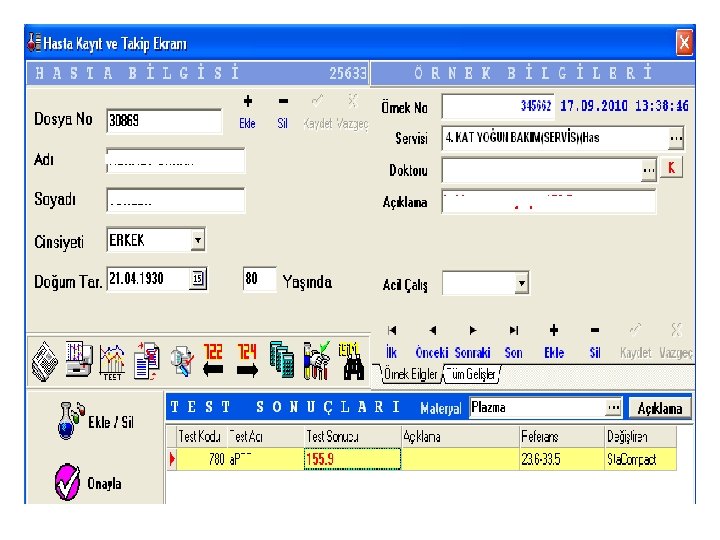
 a. PTT measures the cloting time from the")
Activated Partial Thromboplastin Time (a. PTT) a. PTT measures the cloting time from the activation of factor XII, through the formation of fibrin clot (intrinsic and common pathways) • a. PTT prolangations are caused by: 1. Either factor deficiencies (especially of factors VIII, IX, XI and/or XII) 2. Monitor therapeutic anticoagulan HEPARİN •
 PTT reagent(phospholipid with an intrensic pathway activator such")
Activated Partial Thromboplastin Time (a. PTT) PTT reagent(phospholipid with an intrensic pathway activator such as silica, kaolin. . . ) and Ca++ are added to patient plasma, and the time until clot formation is measured in second.

• prolongation of both the APTT and PT suggests factor X, V, II or I (fibrinogen) deficiency, all of which are rare • a. PTT is normal in factor VII deficiency (PT prolonged) and factor XIII deficiency Most common case of prolonged a. PTT – heparin!!!

Role of PT, PTT: Warfarin, Heparin Monitoring Anticoagulant PT a. PTT Heparin Normal Prolonged Warfarin (Coumadin) Prolonged Normal

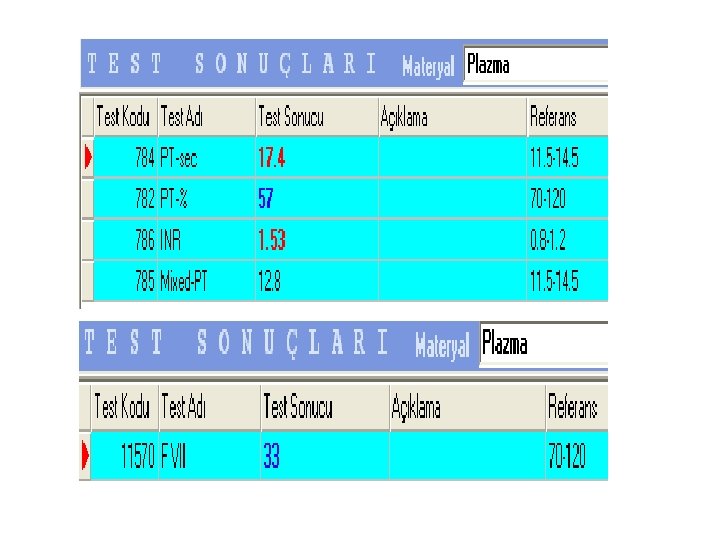
Mixing TEST + Hp F %0 + Np F %100 Mix F %50 Hp a. PTT 70 sn + Hp a. PTT 32 sn Mix 32 sn
 – norm: 14 -15 sec Prolonged TT: • Heparin (much more")
Thrombin time (TT) – norm: 14 -15 sec Prolonged TT: • Heparin (much more sensitive to heparin than a. PTT) • Hypofibrinogenemia
 Prothrombin Time (PT)")
Selected causes of abnormal coagulation tests Partial Thromboplastin Time (a. PTT) Prothrombin Time (PT) Thrombin Time (TT) Bleeding Time (BT) Factor deficiency (except VII) VII, X, V, II, fibrinogen deficiency Low or absent fibrinogen Thrombocytopenia Antibodies to clotting factors Antibodies Dysfibrinogenemia, Von Willebrand’s disease Heparin Warfarin; Vit K defficiency (mild to severe) Heparin Drugs (Aspirin, NSAIDs, high dose penicillins, etc. ) Excessive Warfarin Excessive Heparin hypofibrinogenemia Cirrhosis, Uremia, PLTs dysfunction
 Direct thrombin inhibitors Antiplatelet agents")
Anticoagulants • • Heparin Warfarin (Coumadin) Direct thrombin inhibitors Antiplatelet agents
- Slides: 60