CLOSING THE GAP BETWEEN PRACTICE AND RESEARCH Collecting

CLOSING THE GAP BETWEEN PRACTICE AND RESEARCH: Collecting and using quality adherence data in the real world Clare Mc. Bee, MA, DOT Program Manager at the PACT Project

Conflict of Interest Disclosure Heidi Behforouz, MD and Clare Mc. Bee Have no real or apparent conflicts of interest to report.
 Project Premise that the vulnerable can")
Prevention and Access to Care and Treatment (PACT) Project Premise that the vulnerable can be empowered to effect change at the level of the individual, community, health care system, and society at large Participant-driven Based on health promotion and harm reduction philosophies (defined broadly)
 Graduation")
DOT Integrated into PACT’s Comprehensive Intervention Monitored Self Administration INTAKE Health Promotion (HP) Graduation (MSA) E v al u at io n Health Promotion (HP) DOT* 7/5 day 0 3 day 1 day * While in DOT, Patients receive weekly health promotion T

Who receives DOT? Demographics • • 58% Female 57% Black/AA 25% Latino ~10 Median years since Dx • 54% Clinically Depressed • Age Distribution: o o o 20 – 30: 39. 2% 30 – 40: 18. 6% 50+ : 42. 2% Enrollment • Complex criteria: Clinical status Social status (inclusive of MH/BH) o History of nonadherence o Readiness is crucial to success o o

PACT’s DOT Program • Home visits at dose time provide: Skills-based training in real time and client’s context (“meeting client where they are”) o Emotional support o Empowerment and education o Progress to self-administration o • Total caseload N=25 • 3 DOT Specialists out in the field on any given day • Patients may be seen by different DOT specialists throughout the week • No MEMS Caps • Care team approach: DOT Specialists regularly communicate on client progress with PACT Health Promoters and medical providers via weekly PACT client list reviews, case management meetings and monthly adherence reports

Beyond adherence monitoring Profile of reasons for non-adherence • Stigma and disclosure issues • Housing instability • Substance use • Anxiety/depression • Cognitive impairment • Trauma/DV • Language/cultural barriers • History of incarceration • Co-morbidities (diabetes, Hep C, seizure disorder) A DOT Specialist spends between 10 and 45 minutes with each DOT client per visit, providing education on their HAART regimen and empowerment to overcome adherence barriers

Data collection for adherence monitoring • Sources of adherence data o o o Direct Observation Pillbox Check Patient Self Report • Encounter forms also detail o o Patient symptoms Facilitators/barriers to adherence (i. e. side effects, family member support)

Before… • One person responsible for collecting paper DOT logs and manually entering them into Access database, remaining mindful of DOT schedule, regimens and pillbox checks • PACT team waited one week to see compiled adherence data for a DOT client • DOT Specialists often forgot to turn in paper logs, or would have conflicting interpretations of a shared client’s pillbox check

Before…DOT paper log

Before…DOT paper log

Solution: Smartphone-driven care management application What does it do? • 2 -way data sharing across smartphone- and web-based data base re: CHW encounters ART/non-ART regimens DOT adherence data HIV bloodwork Periodic reminders of missing logs, blood work, appointments o Patient contact data o o o How was it developed? • Contract with Dimagi (Health IT firm) • Development team exposed to CHW practice, work processes, and constraints • Collaboratively developed project plan • Functionality priorities driven by care team and program management

Now… • DOT Specialists enter DOT logs directly into Android smartphones. No more paper logs of client encounters • Adherence data shared across PACT HIV team smartphones, so that information on a shared client’s DOT visits can be immediately accessed by all • DOT staff get a text message reminder at the end of each day with any missing logs. This has greatly reduced the amount of missing data • Any conflicts in pillbox check interpretations are coded and, depending on their complexity, are resolved by the Dimagi system, or by DOT manager

The new DOT log

The new DOT log

Real-time adherence data

How data informs QI • Client engagement patterns (day of week, with particular staff, etc. ) • Staff performance (frequency of direct observations, pillbox checks, self reports) • Client impact (changes in adherence and clinical status, graduation, transition, drop -out rate)

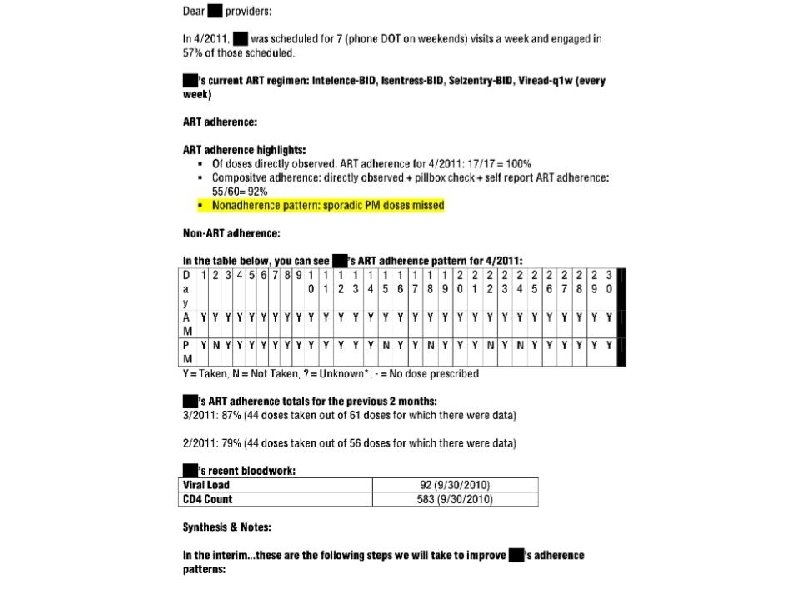
New DOT Monthly Report • Informed by latest research on resistance and virologic failure* • Provides actual data and interpretation • Distributed to providers via email within a week after the end of the month • Opens space for dialogue with providers • Availability of adherence data enhances teambased patient-centered care model *Gardner et al. (2009), Parienti et al. (2008), Parienti et al. (2010), Rong et al. (2007), Rosenblum et al. (2009).

Provider decision-making • HAART regimen changes • Stopping HAART due to reported nonadherence • Changing direction of treatment for comorbidities (seizure disorders, diabetes, Hep C) • Clinical monitoring during DOT transition

Quality real-time adherence data informs Clinician decisionmaking and course of treatment PATIENT QI initiatives by program management Timely CHW interventions
 • Programs")
Conclusions • Technology change is best led and informed by end-users (CHWs) • Programs will grow more robust by feeding their QI initiatives with quality data from the field • Availability of data enhances team-based patient -centered care • Real-time adherence data informs clinician’s decision-making and patient care

Questions? Heidi Behforouz, MD, Director: hbehforouz@partners. org Clare Mc. Bee, MA, DOT Program Manager: cmcbee@partners. org
- Slides: 23