Clinical Webinar Integrated Pharmacy Benjamin Gross Pharm D

Clinical Webinar: Integrated Pharmacy Benjamin Gross, Pharm D, MBA, BCPS, BCACP, CDE, BC-ADM, ASH-CHC Associate Professor Director of Residency Programs Lipscomb University College of Pharmacy

Objectives • Understand services provided by a pharmacist in a primary care office • Recognize quality metrics related to pharmacy services • Develop a plan on how to incorporate pharmacy services into a primary care office with emphasis on Federally Qualified Health Centers (FHQC)

CLINICAL PHARMACY SERVICES • COLLABORATIVE PRACTICE • MANAGE • • DIABETES HYPERLIPIDEMIA HYPERTENSION CONGESTIVE HEART FAILURE ASTHMA AND COPD NICOTINE DEPENDENCE MEDICATION THERAPY REVIEW IMMUNIZATIONS • EDUCATE • • MEDICATIONS DIABETES CHRONIC DISEASE STATES NICOTINE DEPENDENCE • MEDICATION RECONCILATION • QUALITY ASSURANCE • MEDICAL HOME

Comprehensive Medication Management: What is It? • Ensures each patient’s medications (Rx, OTC, alternative, traditional, vitamins, or nutritional supplements) are individually assessed to: • • determine that each medication is appropriate for the patient effective for the medical condition safe given the comorbidities & other meds taken able to be taken by the patient as intended

Comprehensive Medication Management: What is It? • Is Comprehensive Medication Management equal to Medication Therapy Management? • MTM Centers for Medicare & Medicaid Services (CMS) adopted it in January 2003 legislation to refer to the new, additional service required for certain patients receiving Medicare Part D benefits • Comprehensive Medication Management Includes: • • An individualized care plan that achieves intended goals Appropriate follow-up Patient agreement Focus on achieving an optimal regimen optimizing the patients medication experience

Comprehensive Medication Management: Specific Procedures 1. An assessment of the patient’s medication related needs -Uncovering the patient’s medication experience -Medication History -Patient’s current medication record 2. Identification of patient’s medication related problems -Appropriateness of the medication -Effectiveness of the medication -Safety of the medication -Adherence of the medication

Comprehensive Medication Management: Specific Procedures 3. Development of a care plan with individualized goals of personalized interventions -Intervene to solve problems -Establish individualized goals for EACH condition -Design personalized regimens and education -Establish measurable outcomes -Determine appropriate follow-up 4. Follow-up evaluation to determine actual patient outcomes

Comprehensive Medication Management: Which Patients Benefit • Those who have not reached goals for care of chronic disease states • Those experiencing adverse effects from medications • Those in need for preventative therapy • Those who are frequently readmitted for care to the hospital or emergency room

Pharmacy Services in FHQC • Clinical pharmacists focus on managing complex chronic conditions under collaborative drug therapy management agreements (CDTMs) as well as targeting quality and outcomes metrics for the organization. • Current CDTMs include: • • • Diabetes Hypertension Cardiovascular risk reduction Asthma COPD Smoking cessation Depression Anxiety Psychiatric medication monitoring

Pharmacy Services in FHQC • • • Transitions of care from a local hospital Post-discharge medication reconciliation Comprehensive medication reviews for high utilizers of the health care system Addressing gaps in care for elderly patients Pharmacists also support primary care teams through drug information presentations and individualized patient consults.

What does a typical day look like? • One-on-one appointments 30 -60 minutes • Scheduled ahead of time with help from staff • Assure space in clinic to see patients • Available for curbside consults • Balance time seeing patients with time available for curbside consults

WHAT IS A PATIENT-CENTERED MEDICAL HOME? • PUTS THE PATIENT AT THE CENTER OF THE HEALTH CARE SYSTEM • PROVIDES A SYSTEMATIC APPROACH TO PROVIDING COORDINATED CARE TO PATIENTS
 • Care Coordination and Care")
PCMH Standards • Performance Measurement and Quality Improvement (QI) • Care Coordination and Care Transitions (CC) • Care Management and Support (CM) • Patient-Centered Access and Continuity (AC) • Knowing and Managing Your Patients (KM) • Team-Based Care and Practice Organizations (TC)
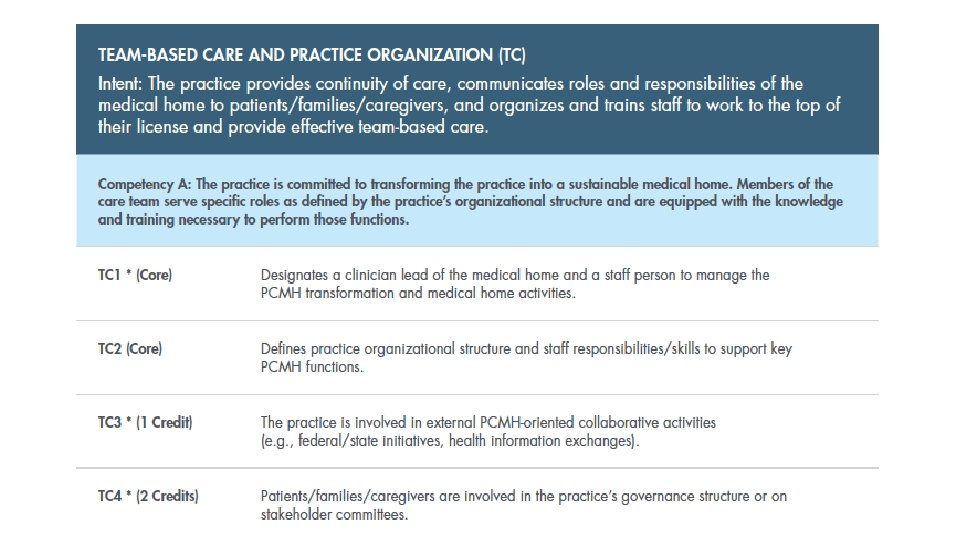

How do you achieve NCQA PCMH recognition? • Must meet all core criteria and earn at least 25 elective credits across five different concept areas
 • Integration of pharmacy services within PCMH model in")
Patient Center Medical Home (PCMH) • Integration of pharmacy services within PCMH model in FHQC • Co-Visits • Collaborative Practice Agreements

Co-Visits vs. Pharmacist-Only Visit

Annual Medicare Wellness Visits • Review of medical and family history • Review of list of current medical providers • Measurement of height, weight, BMI, and BP, along with other appropriate routine measurements • Detection of cognitive impairment • Review of risk factors and establishment of list of risk factors • Review of functional ability • Establishment of a written screening schedule for next 5 to 10 years • Provision of advice and referrals to health education and preventive counseling services

Annual Medicare Wellness Visits • Medicare mandates that AWVs must be furnished by a health professional, meaning a physician; physician assistant, nurse practitioner, or clinical nurse specialist; or a medical professional (including pharmacists) or a team of medical professionals working under the direct supervision of a physician

Annual Medicare Wellness Visits • From a coverage perspective, Medicare provides annual coverage of an AWV for beneficiaries who are no longer within 12 months after the effective date of their first Medicare Part B coverage period and who have not received an AWV within the past 12 months. However, patients may receive subsequent AWVs annually. Currently, initial AWVs are paid at $165 per visit, and subsequent visits at $110 per patient per year. -

Annual Medicare Wellness Visits • Based on the fee schedule for AMVs, about 1000 visits per year are needed to sustain a pharmacist full-time equivalent (FTE) position and associated ancillary personnel resources
 • “Define the Services Provided” • • Pt enrollment or referral Pt")
DEVELOPING (Services) • “Define the Services Provided” • • Pt enrollment or referral Pt encounter Documentation Collaborative agreements: • • • Compliance with practice standards Scope of practice agreement Collaborative drug therapy management agreement Legal & liability issues, risk management Other regulations (OSHA, CLIA, etc) Certification & Credentialing

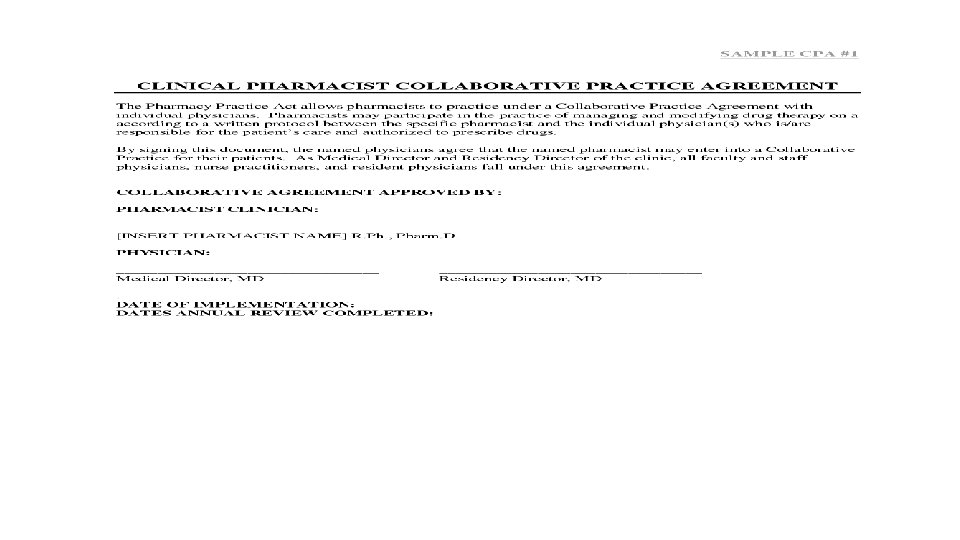
COLLABORATIVE PRACTICE AGREEMENT • AGREEMENT BETWEEN ONE OR MORE PROVIDERS AND PHARMACISTS • QUALIFIED PHARMACTIS WORKING WITHIN THE CONTEXT OF A DEFINED PROTOCOL • PERMITED TO ASSUME PROFESSIONAL RESPONSIBILITY FOR • • PERFORMING PATIENT ASSESSMENTS ORDERING DRUG THERAPY-RELATED LABORATORY TESTS ADMINISTERING DRUGS SELECTING, INITIATING, MONITORING, CONTINUING, AND ADJUSTING DRUG REGIMENS

PROTOCOL • A DRUG THERAPY MANAGEMENT PROTOCOL IS A WRITTEN PLAN • DELEGATES LEGAL PRESCRIPTIVE AUTHORITY TO PHARMACISTS UNDER DESIGNATED CIRCUMSTANCES • SERVES TO GUIDE THEIR CONDUCT • DIRECT THE COURSE OF ACTION • DELINEATE THE FUNCTIONS, PROCEDURES, AND DECISION CRITERIA TO BE FOLLOWED
 Clinical Competencies")
American College of Clinical Pharmacy (ACCP) Clinical Competencies
 • “Evaluate Service Outcomes” • Clinical Outcomes • Humanistic Outcomes • Economic")
SUSTAINING (outcomes) • “Evaluate Service Outcomes” • Clinical Outcomes • Humanistic Outcomes • Economic Outcomes • Should be agreed upon before service begins • Should know “where the bar is” before you jump • DOCUMENTATION VERY IMPORTANT!!!

Value of Clinical Pharmacy Services • Improved Patient Outcomes • Paynesville Area Health Care System • 92% of diabetic patients seen by pharmacist test blood glucose compared to 10% who are not seen by a pharmacist • 89% of anticoagulation patients are within therapy goal • El Rio Community Health Center • Controlled A 1 c increased from 6 % to 41%

Value of Clinical Pharmacy Services • Cost Savings • Harris Count Hospital • 1. 5 million in cost savings • Asheville Project • Decrease in total mean direct medical cost by $1200 per patient year • Increased productivity estimated at $18, 000 annually
 * TOC ICT CCM * - Incident-to - Employer-based - Facility Fee")
SUSTAINING (revenue) * TOC ICT CCM * - Incident-to - Employer-based - Facility Fee - G codes - CLIA waved tests - Procedures (CGMS, ABPM, insulin pump)
 G")
Billing Options CPT Billing Codes Practice Setting Medicare Reimbursement Diabetes Self-Management Training (DSMT) G 0108 (individual All visit) G 0109 (group visit) • • Incident to physician: office visit 99211 Physician- and hospital-based outpatient clinic 99211: $20. 02 Incident to physician: Transitional Care 99496 Management (TCM) 99495 Physician- and hospital-based outpatient clinic G 0108: $53. 70 G 0109: $14. 30 99496: $161. 25 -232. 41 99495: $111. 91 -165. 54 Medication Therapy Management 99605 (first 15 Pharmacy and self-insured employers, Variable minutes for a new contract health plan patient) 99606 (first 15 minutes for an established patient) 99607 (additional 15 minute increments) CMS Annual Wellness Visit G 0438 (first visit) Physician-and hospital-based G 0439 (subsequent outpatient clinic annual visits) Chronic Care Management 99490 Physician- and hospital-based outpatient clinic • • G 0438: $173. 41 G 0439: $117. 28

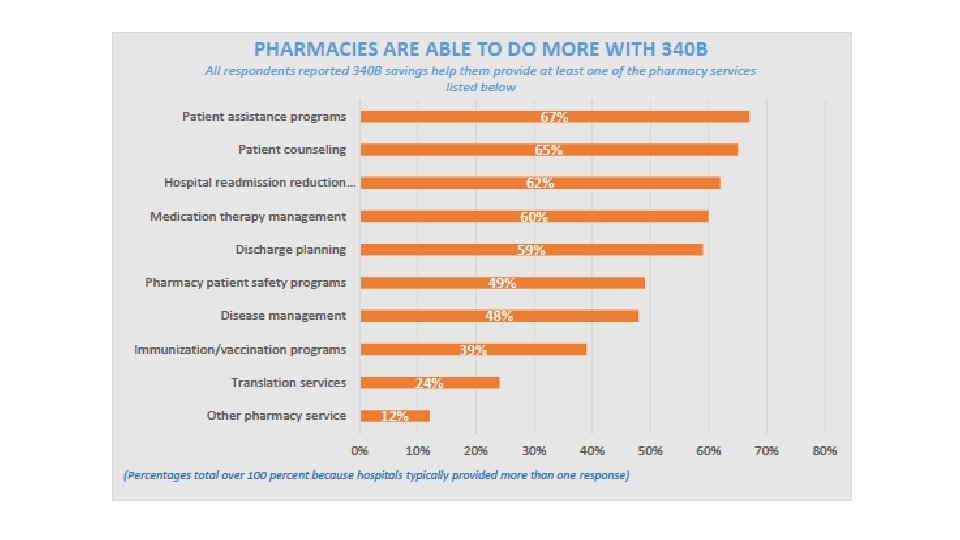
340 B Discount Drug Pricing Program • Average savings of 19 -22% of clinic purchases • Increase the number of patients served • Offset losses from providing pharmacy services for less than full compensation • Reduce prescription prices for patients • Increase services offered at clinics

QUESTIONS? ? ?
- Slides: 35