Clinical Utility of Thromboelastography TEG Lowell Chambers MD
 Lowell Chambers, MD")
Clinical Utility of Thromboelastography (TEG) Lowell Chambers, MD
 CLASSIC COAGULATION CASCADE INTRINSIC PATH (PTT) XII EXTRENSIC PATH (PT)")
Secondary Hemostasis (Coagulation Cascade) CLASSIC COAGULATION CASCADE INTRINSIC PATH (PTT) XII EXTRENSIC PATH (PT) XIIa XI XIa IX VIIa + TF IXa + VIIIa X Xa + Va Ca++ Prothrombin (II) Fibrinogen (I) Thrombin (IIa) Fibrin (Ia)
 PHYSIOLOGIC PATHWAY VIII VII + IX Platelet Thrombin TF IXa")
Secondary Hemostasis (Coagulation Cascade) PHYSIOLOGIC PATHWAY VIII VII + IX Platelet Thrombin TF IXa + VIIIa* V X XI XIa Xa II + Va XIII (transglutaminase) Thrombin Ca++ Fibrinogen Fibrin XIIIa Cross. Linked* Fibrin

Cell-Based Hemostasis

Challenges in Coagulation Evaluation • Evaluation of Platelet Function • Monitoring of New generation anticoagulants • Determination of Hyperfibrinolytic States

Coagulopathy of Trauma Hyperfibrinolysis Prot. C Activation ACIDOSIS Impaired Clotting Factor Function Impaired Platelet Function HYPOTHERMIA HIGH ISS HYPOTENSION CNS Injuries Increased TF Release Long Bone Fxs Fat Embolism Increased IVF & PRBCs Dilution of Clotting Factors & Platelets DIC C O A G U L O P A T H Y Hess J, … Hoyt D, … Bouillon B. J Trauma 2008; 65: 748 -54

Coagulopathy of Trauma • ¼ Significant Trauma patients • 4 x increased mortality • Multifactorial • Currently addressed with: - Whole Blood - 1: 1: 1 Massive Transfusion Protocols Hess J, … Hoyt D, … Bouillon B. J Trauma 2008; 65: 748 -54

Coagulopathy of Trauma • ¼ Significant Trauma patients • 4 x increased mortality • Multifactorial • Currently addressed with: - Whole Blood - 1: 1: 1 Protocols Improved Outcomes Hess J, … Hoyt D, … Bouillon B. J Trauma 2008; 65: 748 -54

Consequences of Overtransfusion • Waste • ALI / MSOF • Thrombosis

Hyperfibrinolysis in Trauma • See in 2 -34% of Trauma Pts • Increased risk with increased ISS, need for transfusion, etc… • Associated with increased mortality Napolitano L, … Moore EE. J Trauma Acute Care Surg 2013; 74: 1575 -86

Fibrinolyis in Trauma Kashuk J, Moore EE, et al. Ann Surg 2010; 252: 434 -44

Hyperfibrinolysis in Trauma Napolitano L, … Moore EE. J Trauma Acute Care Surg 2013; 74: 1575 -86
 • 20, 127 trauma pts in")
• Randomized, multicenter trial (Europe, Asia, Africa) • 20, 127 trauma pts in 274 hospitals • Inclusion criteria: -Hemorrhagic Shock (SBP < 90, HR > 110) -High risk of substantial bleeding -Within 8 hr of injury • TA (1 gm over 10 min. then another gm over 8 hr) versus Placebo

Tranexamic Acid in Trauma All cause mortality reduction of 1. 5%. Lancet 2010; 376: 23 -32

Tranexamic Acid in Trauma Lancet 2010; 376: 23 -32 All cause mortality reduction of 1. 5% with TXA. + No harm from TXA + Low Cost (~$6. 00/gm) Potential to save 70 -100, 000 lives annually world-wide (NNT 1 = 67)

TXA in Trauma • Cheap • Safe • Effective SO WHY NOT USE ROUTINELY IN BLEEDING TRAUMAS ? Added to WHO “Essential Medications List” in 2011 Napolitano L, … Moore EE. J Trauma Acute Care Surg 2013; 74: 1575 -86

CRASH-2 Problems Napolitano L, … Moore EE. J Trauma Acute Care Surg 2013; 74: 1575 -86

Deficiencies in Current Coag. Assessment of Severely Injured Trauma Pts • No rapid, reliable assessment of hyperfibrinolysis • Incomplete assessment of Coagulopathy of Trauma - Lack of Qualitative Platelet Evaluation - Lack of rapid Coag. Assessment - Inability to assess when switch from hypo to hypercoagulable occurs
 • A viscoelastic point of care hemostatic assay • Provides a graphic")
Thrombelastography (TEG) • A viscoelastic point of care hemostatic assay • Provides a graphic presentation of clot formation & lysis Johansson PI, et al. Scan J Trauma, Resus, & Emerg Med 2009; 17: 45.

Hemostasis Monitoring with the TEG® System Measures entire clotting process Measures: ∆Clot strength / time • Rate of clot formation • Strength of clot • Stability of clot S Hemostatic status
 Hartert H. Klin Wochenschr")
TEG - History • Initial description in 1948 (H Hartert) Hartert H. Klin Wochenschr 1948; 26: 577 -83 • Important role in development of open heart surgery and liver transplantation Dr. Kurt von Koulla & Hartert TEG 1950 s Dr. Henry Swan & Hypothermic Open Heart Procedures 1960 s Dr. Thomas Starzl & Liver Transplantation

TEG Method • 0. 36 ml whole blood incubated @ 37 o. C in a heated, kaolin-containing cup (after being collected in Citrate – if delay in running > 3 min) • Pin is suspended into cup and connected to a detector system (torsion wire) • Cup is oscillated at an angle to the pin • Fibrin forms between the cup and pin • Formation of fibrin results in transmitted rotation from the cup to the pin • Tracing is generated as a result of pin’s movement • Pattern & duration of different aspects of tracing provides information on the clotting and lysis process

TEG Tracing and Clotting Process ║ ║ Time § Continuous monitoring of clotting process § Generates parameters that relate to each phase Time (min) Copyright © 2009 Haemonetics Corp.

Analytical Software Graphical Representation Kinetics of clot development LY 30 Percent lysis 30 minutes after MA Reaction time, first significant clot formation Achievement of certain clot firmness Maximum amplitude – maximum strength of clot Copyright © 2009 Haemonetics Corp.
 FFP r. VIIa PCC FFP")
TEG Parameters: R Reaction time (4 – 8 min) FFP r. VIIa PCC FFP + Platelets LMWH + ASA Copyright © 2009 Haemonetics Corp.
 : Angle (47 - 74°) Rate of")
TEG Parameters: K and angle ( ) : Angle (47 - 74°) Rate of clot growth K: Clot kinetics (0 - 4 min) 4 -8 min FFP Cryoprecipitate Copyright © 2009 Haemonetics Corp.
 Platelets ASA")
TEG Parameters: MA Maximum clot strength Maximum amplitude (54 – 72 mm) Platelets ASA Copyright © 2009 Haemonetics Corp.
")
TEG Parameters: LY 30 Clot Breakdown Lysis at 30 minutes (0 – 7. 5%) TXA ACA Copyright © 2009 Haemonetics Corp.

TEG: Basic Patterns Copyright © 2009 Haemonetics Corp.

Hemostasis Monitoring with the TEG® System Measures entire clotting process Measures: ∆Clot strength / time • Rate of clot formation • Strength of clot • Stability of clot S Copyright © 2009 Haemonetics Corp. Hemostatic status
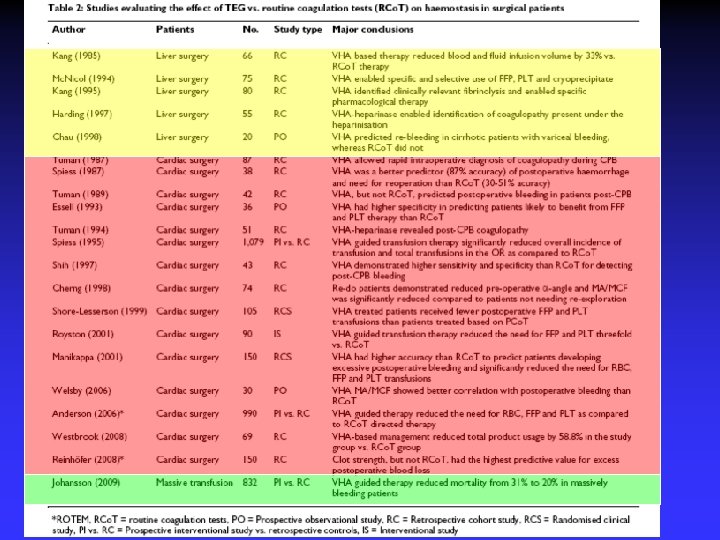

Clinical Experience with standard TEG • Majority of experience is with Cardiac & Liver Surgery • > 20 clinical studies with > 4500 pts in last 25 years • Varying quality (3 rand. clin. trials) • Uniform findings of superiority of TEG over routine coagulation tests. Johansson PI, et al. Scan J Trauma Resus Emerg Med. 2009; 17: 45

Standard TEG in Massive Tranfusion • European Prospective Trial • n=832 massively bleeding pts (21% trauma) • TEG-guided patients: - 20% VS 32% mortality - > FFP - > Plts Johansson PI, et al. Vax Sang 2009; 96: 111 -8

TEG in Trauma Johansson PI, et al. Scan J Trauma Resus Emerg Med. 2009; 17: 45

TEG in Trauma • Differentiates different etiologies of the Coagulopathy of Trauma • Quicker & more accurate than coags. • Permits ID of Hyperfibrinolysis • Differentiates hyper VS hypocoagulability • Gives info. on coag status with newer anticoag. agents Johansson PI, et al. Scan J Trauma Resus Emerg Med. 2009; 17: 45

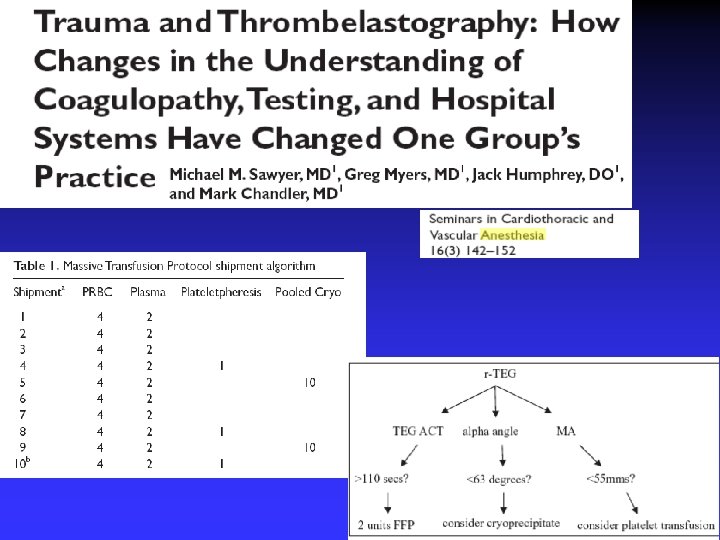
Rapid. TEG • Tissue Factor added to Kaolin in cup • Cuts processing time by ~ 50%: - r-TEG 19. 2 min to completion - TEG 29. 9 min “ - Coags 34. 1 min “ Software available facilitating viewing of TEG on monitor in ICU/OR real-time so initial information available within minutes. Jeger V, et al. J Trauma 2009; 66: 1253 -7 Holcomb JB, et al. Ann Surg 2012; 256: 476 -86

r-TEG Tracing Comparison Rapid. TEG Standard TEG Differences: R range: 0 -1 min & use ACT

U Colorado Experience More “Goal Directed” Therapy “LEAN” Goals met c blood products needed Kashuk JL, Moore EE, et al. Transfusion 2012; 52: 23 -33

U Colorado Case Study • 38 yo F auto VS ped. patient • HD unstable from intra-abd bleeding • Emergent Trauma Lap. Initial r-TEG in OR - PRBCs for hemorrhagic shock - FFP for prolonged ACT - Platelets for depressed MA - 5 gm EACA for elevated LY 30

U Colorado Case Study • Intra-abd. Bleeding controlled but still “oozey” 2 nd r-TEG in OR - Improved coagulopathy (improved ACT) - Improved platelet function (improved MA) - Persistent Fibrinolysis (Sign. Increased LY 30 still) Additional EACA administered

U Colorado Case Study • Pt continued to stabilize • “Oozing” resolved 3 rd r-TEG in OR

Ann Surg 2012; 256: 476

r-TEG U Texas Experience … Holcomb JB, et al. Ann Surg 2012; 256: 476

U Texas Approach • Unstable Pt: 1: 1: 1 Transfusion • Once surgical hemostasis achieved: Holcomb JB, et al. Ann Surg 2012; 256: 476

Baylor Approach • ~ 10 year experience with TEG-directed resusc. • Use conventional TEG rather than r-TEG Tapia NM, … Mattox KL, Suliburk J. J Trauma Acute Care Surg 2013; 74: 378 -86

Baylor Experience • In October 2009 instituted 1: 1: 1 MTP • Reviewed outcomes 21 months before & after • Compared outcomes with TEG-directed VS reflexive 1: 1: 1 MTP Tapia NM, … Mattox KL, Suliburk J. J Trauma Acute Care Surg 2013; 74: 378 -86

Baylor Experience Tapia NM, … Mattox KL, Suliburk J. J Trauma Acute Care Surg 2013; 74: 378 -86

Baylor Experience • No improved survival in MTP with increased FFP utilization • Some subsets of MTP with worse outcomes Tapia NM, … Mattox KL, Suliburk J. J Trauma Acute Care Surg 2013; 74: 378 -86

Baylor Approach Tapia NM, … Mattox KL, Suliburk J. J Trauma Acute Care Surg 2013; 74: 378 -86

? Mt Carmel Approach > 3. 0% TXA Tapia NM, … Mattox KL, Suliburk J. J Trauma Acute Care Surg 2013; 74: 378 -86

U Texas Approach Holcomb JB, et al. Ann Surg 2012; 256: 476

TEG & PE risk assessment • Prospective Study with 2, 070 consecutive Cat. 1 Trauma Alerts (2009 -11) at U Texas, Houston • All had r-TEG • 53 (2. 5%) PEs at median of 6 days (range 2 -31 days) • Sens. 82% Spec. 53% Cotton B, … Holcomb J. J Trauma Acute Care Surg 2012; 72: 1470 -7

TEG & PE risk assessment Sens. 49% Spec. 87% Cotton B, … Holcomb J. J Trauma Acute Care Surg 2012; 72: 1470 -7

• Prospective Blinded Cohort Study • 240 pts undergoing major non-cardiac surgery • Routinely drew ran TEG 2 hr postop & followed • 12 thrombotic complications in 10 pts (6 MI, 2 DVT, 2 PE, 2 CVA)

TEG & Postop Thrombosis

TEG & Postop Thrombosis

TEG & Postop Thrombosis

New Anticoagulant Monitoring Holcomb JB, et al. Ann Surg 2012; 256: 476

TEG & LMWH • LMWH not typically monitored • Anti-Xa levels used when needed: - Limited availability - Inconsistent data • TEG Delta R (with & without heparinase) appears to be a better index of LMWH dose adequacy White H, et al. Blood Coag & Fibrinolysis 2012; 23: 304 -10 Van PY, … Schreiber M. J Trauma 2009; 66: 1509 -17

TEG & LMWH R < 0. 4 associated with DVT & calls for LMWH dose Van PY, … Schreiber M. J Trauma 2009; 66: 1509 -17

Anti-platelet issues • Surgical issue: risk of bleeding VS risk of ischemic events • Medical / Cardiac Issue: variance of response • Current “Gold Standard” in platelet monitoring is Light Transmission Platelet Aggregometry (LTA) : - Requires specialized labs - Poorly standardized between labs - Not routinely used clinically Agarwal S, et al. Anesthesiology 2006; 105: 676 -83

Conventional TEG & Antiplatelets • Not helpful • Kaolin-induced thrombin generation overshadows any platelet effect • Lab & clinical experiences have demonstrated normal TEG MAs in specimens with definitive platelet inhibition on LTA Agarwal S, et al. Anesthesiology 2006; 105: 676 -83

Platelet Mapping • Modified TEG c Heparin added to prevent thrombin activity. • Then add ADP or Arachidonic Acid to determine the contribution of the ADP & Tx. A 2 receptors. • Correlates well with the unwieldy standard of Light Transmission Aggregometry. Mylotte D, et al. Cardiovasc Hematolog Agents Med Chem 2011; 9: 14 -24 Agarwal S, et al. Anesthesiology 2006; 105: 676 -83

Platelet Mapping

Platelet Mapping Minimal Platelet Inhibition: - minimal risk of bleeding - ischemia risk Severe Platelet Inhibition: - risk of bleeding - minimal ischemia risk Wohlauer MV, Moore EE, et al. J Am Coll Surg 2012; 214: 739 -46 Agarwal S, et al. Anesthesiology 2006; 105: 676 -83
 / (MAThrombin")
Platelet Mapping % Inhibition = 100 - [(MAADP or AA – MAFibrin) / (MAThrombin – MAFibrin) X 100] >50% Inhibition 30 -50% Inhibition < 30% Inhibition Response Partial Response Lack of Response Agarwal S, et al. Anesthesiology 2006; 105: 676 -83

TEG vs LTA vs PFA 65 60 91% Correlation between LTA & TEG Agarwal S, et al. Anesthesiology 2006; 105: 676 -83

TEG vs LTA vs PFA Agarwal S, et al. Anesthesiology 2006; 105: 676 -83

Preop Antiplatelet Assessment • Current Anesthesia Policy at U of Wales: -< 30% Platelet inhibition: proceed with surgery - > 30% Platelet Inhibition: wait or administer platelets • “Allows for informed rather than empirical platelet transfusions. ” Kauer J, et al. British J Anaesthesia; 2009; 103: 304 -5
 (n 154)")
Post PCI J Am Coll Cardiol 2005; 46: 1820 -6 (n 38) (n 154)

Post PCI Gurbel PA, et al. J Am Coll Cardiol 2005; 46: 1820 -6

Clinical Utility of TEG • Direct resuscitation of severely injured pts • Guide anticoagulation therapy • Guide anti-platelet therapy
- Slides: 73