Clinical Tests for Hearing and Tests of Eustachian

 Parts: 1. Prongs or tines 2. Shoulder 3. Stem or")





: Vibrating tuning fork kept on pt's mastoid Pt")



: l Normal hearing or B/L equal")






































- Slides: 51
Clinical Tests for Hearing and Tests of Eustachian Tube Function Dr. Vijayalakshmi S
Tuning Fork (Gardiner Brown) Parts: 1. Prongs or tines 2. Shoulder 3. Stem or handle 4. Base or footplate
Tuning Forks Frequencies used in E. N. T. : 256, 512, 1024 Hz l 128 Hz → produces more of vibration sense l more than 1024 → short sound decay time
Striking Surfaces Hard: Olecranon, radial styloid process, patella Soft: Thenar & hypothenar eminences, thick rubber strip Tuning fork is allowed to fall by its own weight Impact area is b/w proximal two-thirds & distal one-thirds of its prongs
Rinne Test
Rinne Test Duration comparison technique: Vibrating tuning fork kept on pt's mastoid Pt signals when sound ceases → Move vibrating tuning fork over opening of ear canal (2 cm away & axis parallel to it) → Patient indicates if sound is still heard
Rinne Test Loudness comparison technique (better): Vibrating tuning fork kept on pt's mastoid Pt signals if sound is heard → Move vibrating tuning fork immediately over opening of ear canal → If sound is heard → patient asked which sound is louder
Results of Rinne Test Better response: l sound heard longer or louder A. C. > B. C. (positive test): l Normal hearing or Sensorineural deafness B. C. > A. C. (negative test): l Conductive deafness
Rinne Negative l 256 Hz = 15 - 30 d. B HL = mild conductive deafness l 512 Hz = 31 - 45 d. B HL = moderate conductive deafness l 1024 Hz = 46 - 60 d. B HL = severe conductive deafness
Weber Test Procedure: Vibrating 512 Hz tuning fork placed in midline of pt’s skull at forehead / vertex / central incisor
Results of Weber test Sound heard equally (central): l Normal hearing or B/L equal deafness Sound lateralizes to deafer ear: l Conductive deafness Sound lateralizes to better hearing ear: l Sensorineural deafness
Why Weber lateralizes to deafer ear in Conductive HL ? 1. Lack of masking effect of surrounding noise on tuning fork sound, as air conduction is reduced in conductive deafness 2. Lack of dispersion of sound energy due to ossicular break
Absolute Bone Conduction Test
Absolute Bone Conduction Test l Pt's B. C. compared vs. examiner's normal B. C. l Vibrating tuning fork kept on pt's mastoid with pt’s E. A. C. occluded (to prevent A. C. ) → pt signals when sound ceases → vibrating tuning fork kept on examiner's mastoid with examiner's E. A. C. occluded
Results of Absolute Bone Conduction Test Pt stops hearing before examiner: l sensorineural deafness Both hear for same duration: l normal hearing / conductive deafness
Schwabach Test
Schwabach Test Same as A. B. C. but E. A. C. is not occluded Pt stops hearing before examiner: l sensorineural deafness Both hear for same duration: l normal hearing Pt hears longer than examiner: l conductive deafness
False Negative Rinne l Etiology: U/L severe Sensorineural deafness l Detection: Rinne negative, Weber lateralized to better hearing ear l Confirmation: A. B. C. reduced in deaf ear l Correction: Repeat Rinne test with masking of better ear with Barany's noise box
False Negative Rinne Mechanism: In deaf ear, air conduction & bone conduction are absent. Trans-cranial transmission of sound to opposite cochlea is perceived as I/L bone conduction. Reported as bone conduction > air conduction in deaf ear (Rinne Negative)
Gelle Test l Vibrating tuning fork placed on pt's mastoid & examiner increases pt's E. A. C. pressure with Siegel's speculum Softer sound: l normal hearing or sensorineural deafness No change in sound: l conductive deafness
Bing Test l Vibrating tuning fork placed on pt's mastoid & examiner blocks pt's E. A. C. Louder sound: l normal hearing or sensorineural deafness No change in sound: l conductive deafness
Tests for E. T. function
1. Valsalva Maneuver Forced expiration with mouth & nose closed. Otoscopy shows lateral bulging of Tympanic membrane
2. Frenzel Maneuver l Hands free Valsalva for pilots l Compression of nasopharyngeal air by muscles of tongue l Otoscopy shows lateral bulging of tympanic membrane
2. Frenzel Maneuver
3. Toynbee Maneuver l More physiological l Swallowing with mouth & nose closed l Otoscopy shows retraction of tympanic membrane
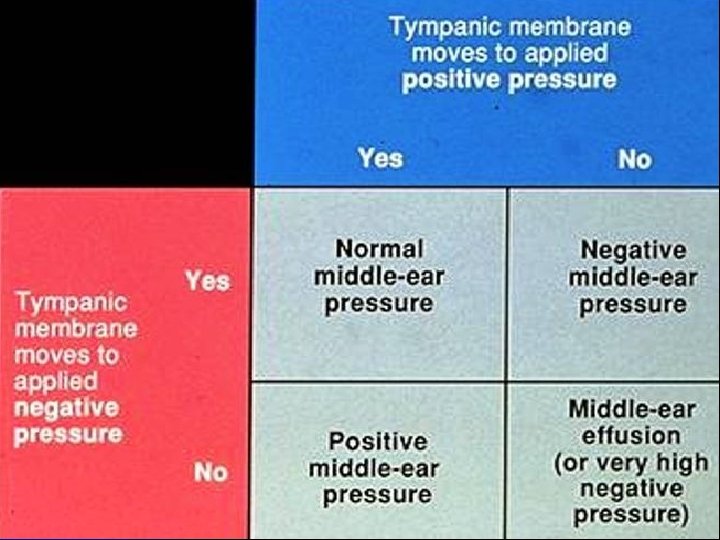
4. Pneumatic otoscopy & Siegelization l Air pressure is alternately increased & decreased within external auditory canal l Mobility of tympanic membrane is observed l Normal mobility indicates good patency of Eustachian tube
Siegelization
Pneumatic Otoscope
Normal Tympanic Membrane
Eustachian Tube dysfunction
Early otitis media with effusion
Late otitis media with effusion
Acute suppurative otitis media
Ear drum perforation
5. Politzerization
Politzer Bag
5. Politzerization l Rubber tube attached to a Politzer bag put into one nostril & both nostrils pinched l Patient asked to swallow or repeat “k” l Politzer bag is squeezed simultaneously l Otoscopy shows lateral bulging of ear drum in patent Eustachian tube
6. E. T. catheterization
Eustachian tube catheter
6. E. T. catheterization l E. T. catheter passed along nasal floor till it touches posterior wall of naso-pharynx. l Catheter rotated 90° medially & pulled forward till it impinges on posterior nasal septum. l Catheter rotated 180° laterally, & its tip inserted into opening of E. T. l Politzer bag attached to outer end of catheter
6. E. T. catheterization Air pushed into E. T. catheter by squeezing Politzer bag. Examiner hears by Toynbee auscultation tube put in pt's ear. Blowing sound = normal E. T. patency Bubbling sound = middle ear fluid Whistling sound = partial E. T. obstruction No sound = complete obstruction of E. T.
7. Tymapanometry
7. Tymapanometry l Type C = E. T. dysfunction l Type B = fluid in middle ear
8. William’s pressure equalization test l 200 mm H 2 O pressure is created in patient’s external auditory canal l Patient asked to swallow 10 times l Residual pressure in patient’s external auditory canal after 10 th swallow is noted l Test repeated with -ve 200 mm H 2 O pressure created in patient’s external auditory canal
William’s Test Residual Pressure Result Up to + 50 mm H 2 O normal E. T. function + 51 to + 100 mm H 2 O mild dysfunction + 101 to + 199 mm H 2 O moderate dysfunction + 200 mm H 2 O severe dysfunction
9. Sono-tubometry l Sound made in pt’s nasal cavity & detected with stethoscope in patient’s external auditory canal l Loud sound = patent Eustachian tube 10. Eustachian tube Salpingogram l Dye instilled through E. T. catheter & X-ray taken 11. C. T. scan & M. R. I. of skull
12. Trans-nasal E. T. video-endoscopy 13. Test for E. T. patency in T. M. perforation l Saccharine crystal / antibiotic ear drop / methylene blue placed in middle ear via ear drum perforation. l Sweet taste / bitter taste / blue staining of secretions indicates patent Eustachian tube
Thank You