CLINICAL PHARMACY in GASTROENTEROLOGY Digestive diseases All diseases




 Hypertrophic Gastritis n At times, the folds in the stomach will become")
 Symptoms n The symptoms of gastritis depend on how acute it is")
 is a very common ailment, affecting one out of eight")
 n This funny-sounding name identifies the basic")


")
 Forms of production: 0, 15 g and 0, 3 g tablets and")








 and saline (liquid or")





- Slides: 28
CLINICAL PHARMACY in GASTROENTEROLOGY
Digestive diseases All diseases that pertain to the gastrointestinal tract are labelled as digestive diseases. This includes diseases of the esophagus, stomach, first, second and third part of the duodenum, jejunum, ileum, the ileo-cecal complex, large intestine (ascending, transverse and descending colon) sigmoid colon and rectum.
Gastritis means inflamation of the stomach. It means that white blood cells move into the wall of the stomach as a response to some type of injury. Gastritis does not mean that there is an ulcer or cancer. It is simply inflammation–either acute or chronic. What are the causes of gastritis? Helicobacter Pylori n This is the name of a bacteria that has learned to live in the thick mucous lining of the stomach. Although it doesn't actually infect the underlying tissue, it does result in acute and chronic inflammation. It probably occurs early in childhood and remains throughout life unless antibiotics cure it. The infection can lead to ulcers and, in later life, even to stomach cancer in some people. Fortunately, there are now ways to make the diagnosis and treat this disorder. Autoimmune Gastritis - Pernicious Anemia n The stomach lining also may be attacked by the immune system leading to loss of the stomach cells. This causes acute and chronic inflammation which can result in a condition called pernicious anemia. The anemia occurs because the body no longer can absorb vitamin B 12 due to a lack of a key stomach factor, destroyed by the chronic inflammation. Stomach cancer can even occur later in life.
Gastritis Aspirin & NSAID Gastritis n NSAID stands for non-steroidal anti-inflammatory drug. These arthritis and pain relievers and include the overthe-counter drugs Advil, Naprosyn, Motrin and ibuprofen as well as many prescription arthritis medicines such as Voltaren, Feldene, Lodine and Relafen. Along with aspirin, they reduce a protective substance in the stomach called prostaglandin. These drugs usually cause no problems when taken for the short-term. However, regular use can lead to a gastritis as well as a more serious ulcer condition. Alcohol n Alcohol and certain other chemicals can cause inflammation and injury to the stomach. This is strictly dose related in that a lot of alcohol is usually needed to cause gastritis. Social or occasional alcohol use is not damaging to the stomach although alcohol does stimulate the stomach to make acid.
Gastritis (cont’d) Hypertrophic Gastritis n At times, the folds in the stomach will become enlarged and swollen along with the inflammation. There is not a great deal known about why this occurs. A variation of this type of gastritis is called Ménétrier's disease where the gastric folds become gigantic. With this condition, there is often protein loss into the stomach from these weeping folds.
Gastritis (cont’d) Symptoms n The symptoms of gastritis depend on how acute it is and how long it has been present. In the acute phase, there may be pain or gnawing in the upper abdomen, nausea and vomiting. In the chronic phase, the pain may be dull and there may be loss of appetite with a feeling of fullness after several bites of food. Very often, there are no symptoms at all. If the pain is severe, there may be an ulcer as well as gastritis. Treatment n The treatment of gastritis will depend on its cause. For most types of gastritis, reduction of stomach acid by medication is often helpful. Beyond that, a specific diagnosis needs to be made. Antibiotics are used for infection. Elimination of aspirin, NSAIDs or alcohol is indicated when one of these is the problem. For the more unusual types of gastritis, other treatments may be needed.
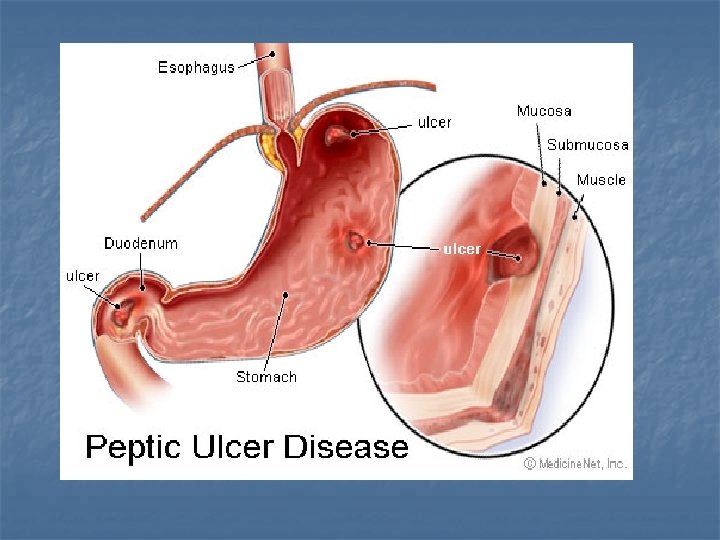
Peptic ulcer disease (PUD) is a very common ailment, affecting one out of eight persons in the United States. The causes of PUD have gradually become clear. With this understanding have come new and better ways to treat ulcers and even cure them
PEPTIC ULCER DISEASE Helicobacter pylori (H. pylori) n This funny-sounding name identifies the basic cause of most peptic ulcers, excluding those caused by aspirin or arthritis drugs. This bacteria has a twisted spiral shape and infects the mucous layer lining of the stomach. This infection produces an inflammation in the stomach wall called gastritis. The body even develops a protein antibody in the blood against it. The bacteria is probably acquired from contaminated food or from a drinking glass. It ims only after H. pylori bacteria injure the protective mucous layer of the stomach, allowing damage by stomach acid, that an ulcer develops. Arthritis medications include ibuprofen (Advil), Feldene, Naprosyn, Voltaren, Indocin, Aleve, Lodine, and many others. As with aspirin, they can damage the mucous layer of the stomach, after which the stomach acid causes the final injury. So, H. pylori and certain drugs are the two major factors that cause ulcers. In rare cases, a patient will produce very large amounts of acid and develop ulcers. This condition is called Zollinger -Ellison syndrome. Finally, some people get ulcers for unknown reasons.
PEPTIC ULCER DISEASE Symptoms Ulcers cause gnawing, burning pain in the upper abdomen. These symptoms frequently occur several hours following a meal, after the food leaves the stomach but while acid production is still high. The burning sensation can occur during the night and be so extreme as to wake the patient. Instead of pain, some patients experience intense hunger or bloating. Antacids and milk usually give temporary relief. Other patients have no pain but have black stools, indicating that the ulcer is bleeding. Bleeding is a very serious complication of ulcers.
PEPTIC ULCER DISEASE Therapy of PUD has undergone profound changes. There are now available very effective medications to supress and almost eliminate the outpouring of stomach acid. These acid-suppresssing drugs have been dramatically effective in relieving symptoms and allowing ulcers to heal. If an ulcer has been caused by aspirin or an arthritis drug, then no subsequent treatment is usually needed. Avoiding these latter drugs, should prevent ulcer recurrence. The second major change in PUD treatment has been the discovery of the H. pylori infection. When this infection is treated with antibiotics, the infection, and the ulcer, do not come back. Increasingly, physicians are not just suppressing the ulcer with acidreducing drugs, but they are also curing the underlying ulcer problem by getting rid of the bacterial infection. If this infection is not treated, the ulcers invariably recur. There a number of antibiotic programs available to treat H. pylori and cure ulcers. Working with the patient, the physician will select the best treatment program available
Treatment of peptic ulcer n n n Antimicrobial agents (tetracycline, bismuth subsalicylate, and metronidazole) to eradicate H. pylori infection Misoprostol (a prostaglandin analog) to inhibit gastric acid secretion and increase carbonate and mucus production, to protect the stomach lining Antacids to neutralize acid gastric contents by elevating the gastric p. H, thus protecting the mucosa and relieving pain Avoidance of caffeine and alcohol to avoid stimulation of gastric acid secretion Anticholinergic drugs to inhibit the effect of the vagal nerve on acid-secreting cells H 2 blockers to reduce acid secretion Sucralfate, mucosal protectant to form an acid-impermeable membrane that adheres to the mucous membrane and also accelerates mucus production Dietary therapy with small infrequent meals and avoidance of eating before bedtime to neutralize gastric contents Insertion of a nasogastric tube (in instances of gastrointestinal bleeding) for gastric decompression and rest, and also to permit iced saline lavage that may also contain norepinephrine Gastroscopy to allow visualization of the bleeding site and coagulation by laser or cautery to control bleeding Surgery to repair perforation or treat unresponsiveness to conservative treatment, and suspected malignancy.
Ranitidine (Ranitidin) Forms of production: 0, 15 g and 0, 3 g tablets and ampoules with 2 ml of 2, 5 % solution.
RECOMMENDATIONS OF HELICOBACTER PYLORI ERADICATION • • omeprazole 20 mg amoxicillin 1000 mg clarithromycin 500 mg, all twice daily for 7 days. An alternative regimen with a similar eradication rate of around 90% is: • omeprazole 20 mg • clarithromycin 250 mg • metronidazole 400 mg, again all twice daily for 7 days.
A typical quadruple therapy § § a PPI twice a day bismuth 120 mg four times a day metronidazole 400 mg three times a day oxytetracycline 500 mg four times a day, all for 7 days.
Ulcers associated with NSAIDs § omeprazole 20 mg daily is preferable to ranitidine 150 mg twice daily as the respective rates of healing are 80% and 63%. § H 2 RAs are slow to heal the ulcers if the offending drug is not stopped and so, under these conditions, a PPI is preferred. § H pylori eradication is no more effective than omeprazole alone to heal ulcers, but if the infection is present, then eradication will reduce the rate of relapse. § H pylori is not associated with an increased risk of ulcer with NSAIDs in the elderly but there is an increased risk of bleeding.
Motilium Form of production: 0, 01 g tablets
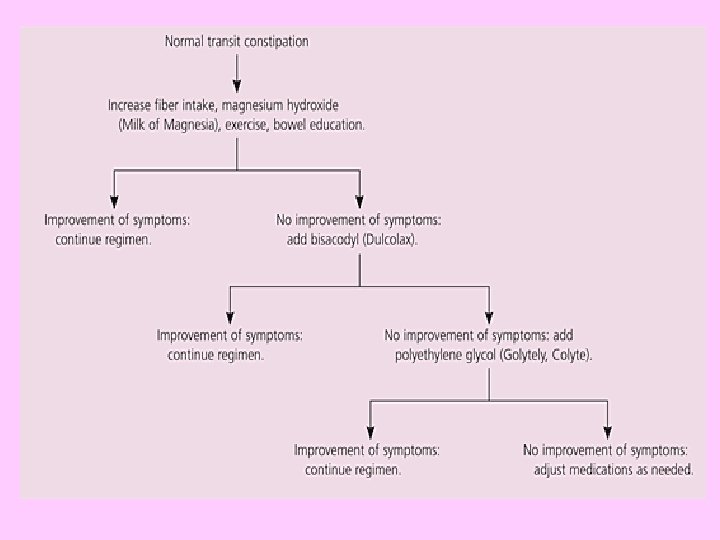
LAXATIVES AND CATHARTICS Constipation can be defined as infrequent or hard pellet stools, or difficulty in evacuating stool. Passing one or more soft, bulky stools every day is a desirable goal. While troublesome, constipation is not usually a serious disorder. However, there may be other underlying problems causing constipation and, therefore, testing is often recommended.
Constipation § Constipation is often caused by a lazy colon that does not contract properly and fails to move the stool to the rectum. The colon also can become spastic and remain contracted for a prolonged time. In this case, stool cannot move along. Too much water is absorbed and hard pellet-like stool develops. Constipation also can result from a mechanical obstruction, such as tumors or advanced diverticulosis, a disorder which can distort and narrow the lower-left colon. Other conditions that can produce a sluggish, poorly contracting bowel include: pregnancy, certain drugs, thyroid hormone deficiency, the chronic abuse of laxatives, travel, and stress.
Indications for Use § 1. To relieve constipation in pregnant women, elderly clients whose abdominal and perineal muscles have become weak and atrophied, children with megacolon, and clients receiving drugs that decrease intestinal motility (eg, opioid analgesics, drugs with anticholinergic effects) § 2. To prevent straining at stool in clients with coronary artery disease (eg, postmyocardial infarction), hypertension, cerebrovascular disease, and hemorrhoids and other rectal conditions § 3. To empty the bowel in preparation for bowel surgery or diagnostic procedures (eg, colonoscopy, barium enema) § 4. To accelerate elimination of potentially toxic substances from the GI tract (eg, orally ingested drugs or toxic compounds) § 5. To prevent absorption of intestinal ammonia in clients with hepatic encephalopathy § 6. To obtain a stool specimen for parasitologic examination § 7. To accelerate excretion of parasites after anthelmintic drugs have been administered § 8. To reduce serum cholesterol levels (psyllium products)
Laxatives There are two main types of laxatives: stimulants (chemical) and saline (liquid or salt). They occasionally help temporary constipation problems. However, chronic use of laxatives, especially stimulant laxatives is discouraged because the bowel becomes dependent upon them. Bowel regularity should occur without laxatives. An occasional enema is preferrable over the chronic use of laxatives.
Contraindications to Use Laxatives and cathartics should not be used in the presence of undiagnosed abdominal pain. The danger is that the drugs may cause an inflamed organ (eg, the appendix) to rupture and spill GI contents into the abdominal cavity with subsequent peritonitis, a life-threatening condition. Oral drugs also are contraindicated with intestinal obstruction and fecal impaction.
Diet The following foods should be eaten daily in adequate amounts Whole grain breads (whole wheat) Bran cereals § Vegetables -- Root (potatoes, carrots, turnips), leafy green (lettuce, celery, spinach), or cooked high residue (cabbage) § Fruit -- Cooked or stewed (prunes, applesauce) or fresh fruit (skin and pulp) § Bulking Agents -- Fiber is the undigested part of plant food that passes into the colon. Certain types of fiber can absorb and hold large amounts of water. This, in turn, results in a larger, bulkier stool which is soft and easier to pass. Adequate fiber in food or from supplements is recommended daily. This type of water-retaining fiber generally is easily obtained each day by one of the following: § Food bran -- This is available as wheat, oat or rice bran. Processing of wheat and other grains removes this valuable fiberous part of the food so these processed products should be avoided. § Psyllium bran -- The psyllium plant is remarkable because its ground seeds can retain so much water. This product is available as Metamucil, Konsyl, Effersyllium, Per Diem Fiber, or the less expensive generic preparation in drug and health food stores. Although labeled a laxative, it really is not a laxative. § Methylcellulose -- This is another fiber derived from wood which also retains water. It is available as Citrucel.
Antidiarrheals
• • • Antidiarrheal drugs are indicated in the following circumstances: 1. Severe or prolonged diarrhea (>2 to 3 days), to prevent severe fluid and electrolyte loss 2. Relatively severe diarrhea in young children and older adults. These groups are less able to adapt to fluid and electrolyte losses. 3. In chronic inflammatory diseases of the bowel (ulcerative colitis and Crohn’s disease), to allow a more nearly normal lifestyle 4. In ileostomies or surgical excision of portions of the ileum, to decrease fluidity and volume of stool 5. HIV/AIDS-associated diarrhea 6. When specific causes of diarrhea have been determined
Contraindications to Use Contraindications to the use of antidiarrheal drugs include diarrhea caused by toxic materials, microorganisms that penetrate intestinal mucosa (eg, pathogenic E. coli, Salmonella, Shigella), or antibioticassociated colitis. In these circumstances, antidiarrheal agents that slow peristalsis may aggravate and prolong diarrhea. Opiates (morphine, codeine) usually are contraindicated in chronic diarrhea because of possible opiate dependence. Difenoxin, diphenoxylate, and loperamide are contraindicated in children younger than 2 years of age.