Clinical Manifestations Overview of Management of Pulmonary Tuberculosis
")
Clinical Manifestations & Overview of Management of Pulmonary Tuberculosis Dr Ruchi Dua (Associate Prof) Dept of Pulmonary Medicine

Learning Objectives • When to suspect Pulmonary Tuberculosis? • How to diagnose? • How to manage a case of drug susceptible Tuberculosis?
 • TB suspect Presumptive Tb • > 2 weeks cough")
When to suspect? (Pulmonary) • TB suspect Presumptive Tb • > 2 weeks cough • fever>2 wks, Dyspnea • significant wt loss Chest pain • Haemoptysis • abnormal CXR

Signs • General • Emaciated • Pallor • Cyanosis • Clubbing • Edema • LNpathy

• Respiratory • Any • Consolidation • Fibrosis • Cavity • Pleural inv • Miliary



Signs • Bronchial • Dec/Absent BS • Normal • Added sounds

Diagnostic tools

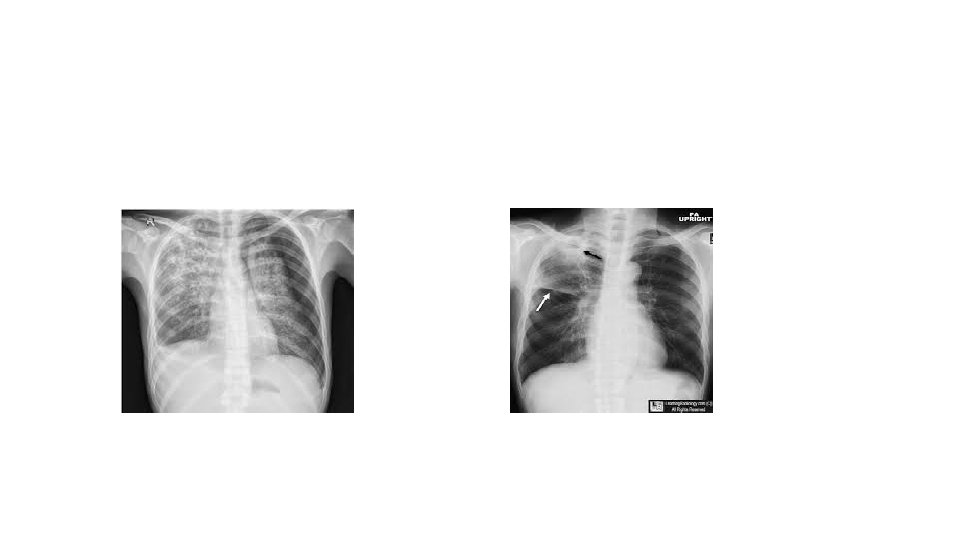
Diagnostics • CXR: • Sensitivity & poor specificity • Complementary tool

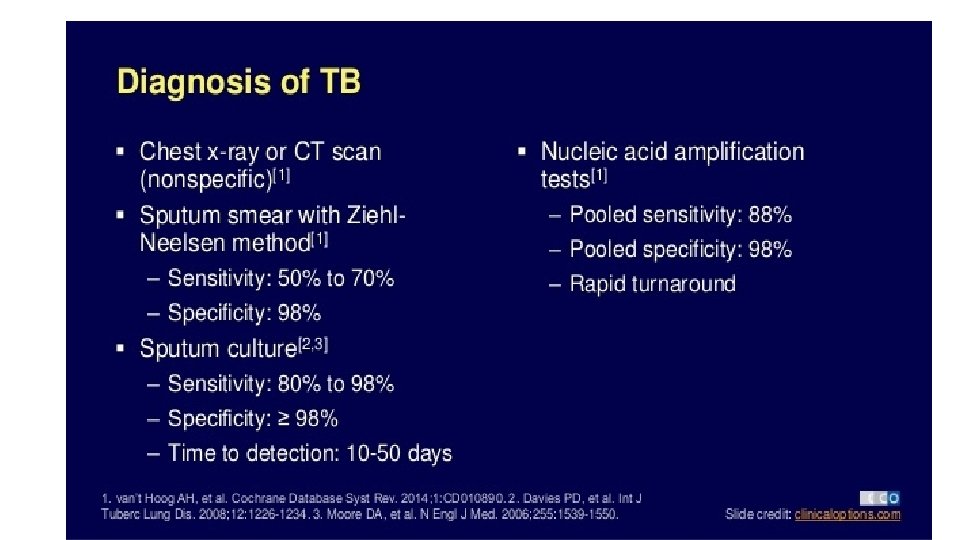
• Microscopy: • Serology: Banned • Gold standard: culture • • LJ media Rapid : Bactec MGIT Bac T

Diagnosis • Microscopy • ZN stain • Flourescent • Culture • solid (6 -8 wks) • liquid (42 days) • Rapid • CBNAAT • LPA Phenotypic methods Genotypic methods

OLD
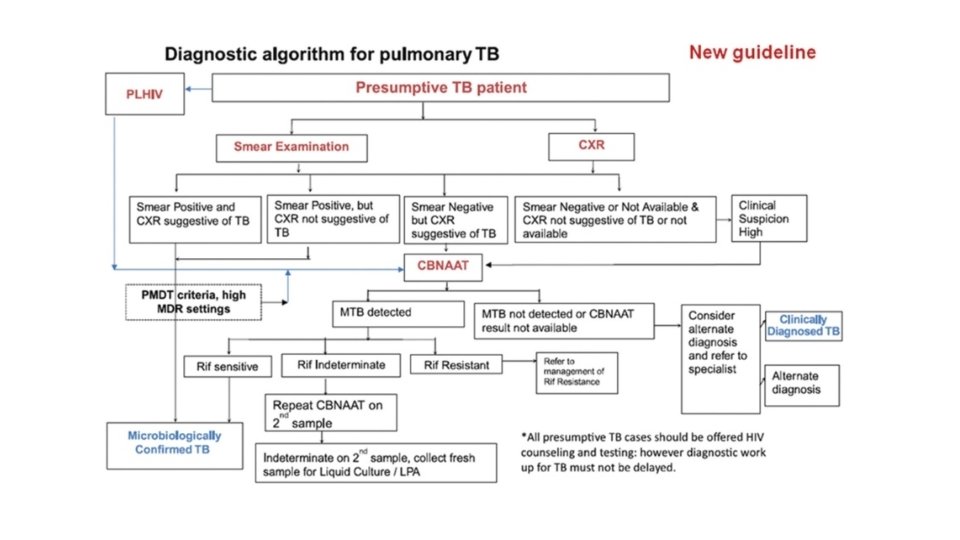

RNTCP 2017

Management • Medical: • long duration • IP & CP • Surgery: complications • Haemoptysis • Aspergilloma • Pleural diseases

TREATMENT REGIMENS Type of TB case Intensive Phase Continuation Phase New 2 RHEZ 4 RHE Retreatment 2 SHREZ/1 RHEZ Intermittent regimens 5 RHE are being changed to daily regimens under RNTCP in India R; rifampicin, H: isoniazid, E: ethambutal, Z: pyrazinamide, S: streptomyci n

• CAT 1 & 2 • CAT 4 : MDR • CAT 5: XDR • Definitions • • MDR: R and H XDR: R and H, any FQ, any injectables(kanamycin, amikacin, capreomycin) Primary & acquired resistance Mono/poly drug resistance: DRTB

DR TB: Principles of Treatment • MDR: 4 second line drugs /not used • XDR: 7 drugs • Duration: 24(MDR), 36(XDR) DOTS plus previously

Second line drugs • Treatment longer • Toxic • Expensive more • Stress: emergence rather than treatment of DRTb

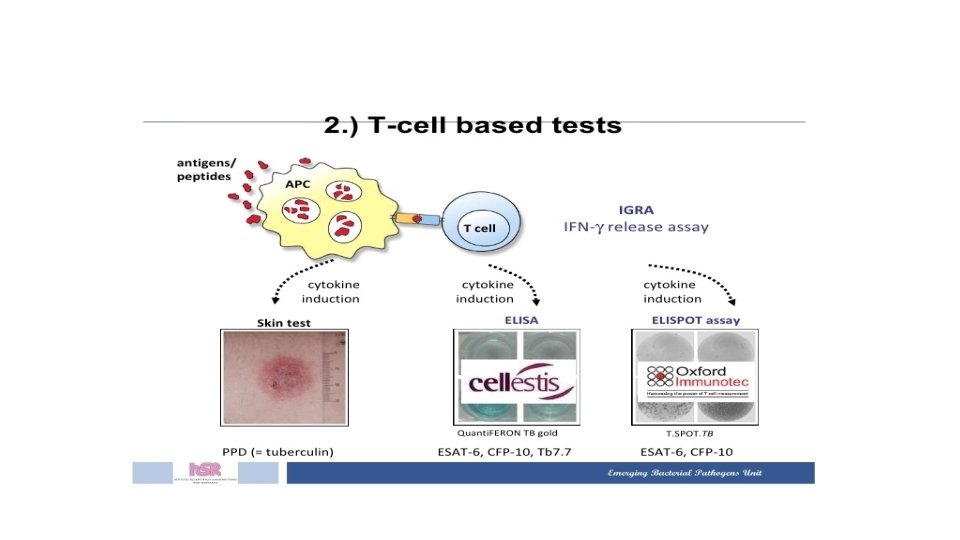
Infection Vs Disease • What ‘s the difference • For Infection • Mantoux/PPD • Interferon gamma release Assay • TB Gold/Elispot
 Pleural -Empyema/pneumo")
COMPLICATIONS • Local • • ARDS/respiratory failure Bronchiectasis/PTOAD aspergilloma haemoptysis (symp ) Pleural -Empyema/pneumo Extensive lung destruction Rt middle lobe syndrome Scar ca
 • Cor-pulmonale")
• Systemic • shock • amyloidosis • disseminated tb-(laryngeal tb) • Cor-pulmonale

THANK YOU
- Slides: 27