CLINICAL EXAMINATION MANDIBLE FRACTURE Classification of Mandible fracture

CLINICAL EXAMINATION MANDIBLE FRACTURE

Classification of Mandible fracture

Definition • A fracture is a disruption in the continuity of a bone stressed beyond its elastic modulus, with the formation of two or more fragments.

I. III. IV. V. Location of problem to be treated. Diagnosis & treatment plan Documentation Assessment of treatment Epidemiological studies

Approaches • Direct or indirect • Complete or incomplete • Mechn- bending, torsion, shear, contrecoup. avulsion and burst type • Site • Displacement • Number-single , multiple or comminuted • Integument- closed or open • Shape- transverse , oblique butterfly, • oblique surface fracture

A –Dentoalveolar B-Condyle C-Coronoid D-Ramus E-Angle F-Body G-Para symphysis H-Symphysis

• • • Simple Compound Comminuted Pathological Green stick

Cause of fracture a. Direct violence b. Indirect violence c. Excessive muscular contraction

Direct violence a. b. c. d. Unilateral fracture Bilateral fracture Multiple fracture Comminuted fracture
 1. 2. 3. 4. 5. Number of fracture /fragments location")
AO CLASSIFICATION( FLOSA CLASSIFN) 1. 2. 3. 4. 5. Number of fracture /fragments location of fracture Status of occlusion Soft tissue involvement Associated injuries ( F) ( L) (O) (S) (A)
 • • • F 0 -")
No of Fragments ( F 1 -F 4) • • • F 0 - Incomplete fracture F 1 - Single fracture F 2 -Multiple fracture F 3 -Comminuted fracture F 4 -Fracture with a bony defect

F 2 -Multiple fracture • Category F 1/F 1 -Bilateral fracture

F 2/F 0 • Unilateral segmental fracture( multiple fracture in one segment

Multiple fracture with F 2/F 1 F 2/F 2

F 3 -comminuted F 4 - bony defect
")
Fracture by site (L 1 -L 8 )
 • O 0 -No malocclusion • O 1")
Displacement ( O 0 -O 2) • O 0 -No malocclusion • O 1 -Malocclusion • O 2 - Non existent malocclusion
 • • • S 0 -closed S 1")
Soft tissue involvement(S 0 -S 4) • • • S 0 -closed S 1 -open intraorally S 2 -open extraorally S 3 -open intra and extraorally S 4 -soft tissue defect
 • • A 0 -None A 1 -Fracture")
Associated fractures( A 0 -A 6) • • A 0 -None A 1 -Fracture or loss of tooth A 2 -Nasal bone A 3 -Zygoma A 4 -Le Fort I A 5 -Le Fort II A 6 -Le Fort III

Clinical Examination • Three stagesq Immediate assessment and treatment of q q constituting a threat to life General clinical examination Local examination any condt

PRIMARY SURVEY • Mf injuries may associated with body injuries may constitute threat to life than facial trauma • Rapid survey & Assessment v A-Airway v B-Breathing & Ventilation v C-Circulation & Hemorrhage control v D-Disability-Neurological assessment v E-exposure to external environment

AIRWAYS Management in Head injury

Oral airwys Nasopharyngeal

Breathing & ventilation

Circulation & Hemorrhage Control

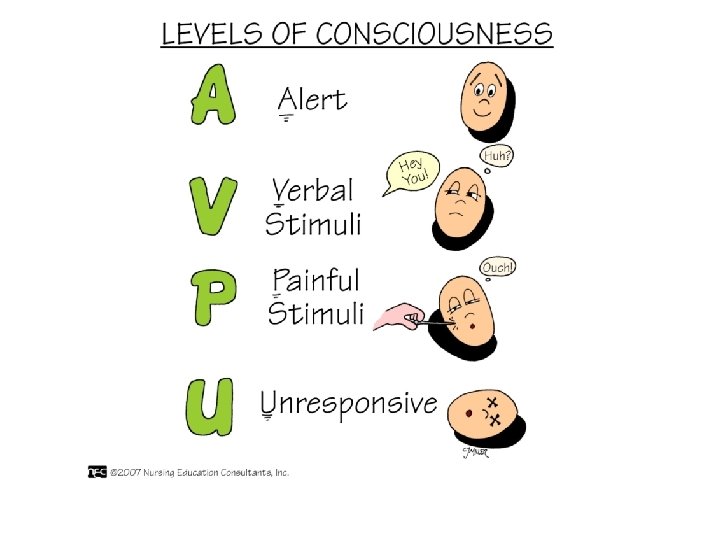
Shock-hypovolumic • Recognition v Central pulse –Femoral /carotid v Skin colour-pink-ashen grey-white v Level of consciousness-confusion-aggression-drowsinesscoma v Pulse- 120/min ( very thready) v Respiratory rate-20/min- Tachypnea v Weakness-due to hypoxia , acidosis v Urinary out put- >30 ml/hr- 0 -10 ml/hr
 v Pressure pack")
• Fluid replacement- Crystalloids. Colloids, Blood • Local-( Maxillofacial aspect) v Pressure pack v Ligation of Vessel v Direct dental wiring at fracture region

Disability –Neurological Assessment

• Careful clinical examination and no operative intervention without rule out additional more serious injuries • If cerebral hemorrhage , loss of consciousness • Additional injuries required urgent treatment than MF injuries • In polytrauma pt treated concurrently • Major injuries- careful inspection/palpation reveal their presence –treated accordingly

• If fracture mandible pt in shocked, very unusual, • Some more serious condition other than fracture mandible should be suspected and treated • first

St 21 AUG Clinical Examination

• • Preparation for examination Face-gently cleaned with warm water Remove road dirt etc-evaluation of soft tissue injury Mouth-loose , broken teeth, or dentures, any congealed blood removed with swab in nontooth forcep • If denture-full/ pieces reassemble piece so portion should be missing -possibly displaced down into throat • Complete extra & intra oral cleaning-assess full extent of injury

• During cleaning cranium and cervical spine should be carefully inspected and palpated for sign of injury

Extravsation of blood from injured bone resulted swelling of face-more swelling increase capillary permeability and edema Swelling+ecchymosis-fracture Facial deformity-fracture & displaced fragment Open hang mouth-B/L condylar #

Swelling

GENERAL EXAMN • Conscious pt- support his jaw with own hand • Compound fracture- blood stained saliva may dribbled out from corner of mouth • Palpation-begin from bilateral condylar regiondownwards posterior along lower border of mandible. • Any bone tenderness- pathognomic of fracture • Deformity /bony cerpitus present • Anesthesia/ paresthesia- injury to IAN- reduced or absent sensation On one or both side of the lower lip

TM JOINT EXAMINATION

Neck /Sub condylar region

LOWER BORDER PALPATION

Intra Oral Examination Clean oral cavity-lukewarm mouth wash/ cleaned with moistened swab Congealed blood, fragments of tooth, alveolus, denture removed with forcep/ suction tip Buccal & Libgual sulciecchymossis, submucosal extravastion of blood-#

• Any lingual mucosa hematoma-# • Bec lingual mucosa directly overlied periosteum of mandible • Linear hematoma in third molar reg-indi fracture

OCCLUSION

OCCLUSAL SURFACE Edentoulus/ alv ridge Step in occlusion, laceration in overlying mucosa Toothluxation/subluxation, crown fracture/dentine/pulp exposed ? Any loose filling, fine crack/split tooth Missing-tooth, f illing, crown, denture, portion of tooth. CHEST X-RAYS

BI MANUAL PALPATION • Fracture site- mobility placing finger and thumb on each side and using pressure to elicit mobility • Any pain in jaw movement recorded. • Flat of both hands placed over two angles of mandible and gentle pressure exerted-if pain • If crack fracture is present

INTRA ORAL EXAMN Bi manual Symphyseal region

Displacement of fracture • • • Direction and intensity of the traumatic force. Site of fracture Direction of fracture line Muscle pull exerted on the fractured fragments Presence or absence of tooth. Extent of soft tissue wounds

SIGN AND SYMPTOMS • SIGN , SYMPTOMS OFMANDIBULAR FRACTURE

Common Sign & symptoms q Injury q Pain- pain upon movement r remote from the site of injury q Abnormal mobility-abn mobility in dental arches r during jaw movement. q Bleeding- active bleeding / hematoma or ecchymosis may follow a fracture process. q Crepitus- Cracking, grating sound can be detected during palpation of injury site.

q Deformity-facial deformity depending upon degree and direction of impact, also direction of fracture line and muscle pull also. q Ecchymosis- and edma- seen extra orally and intraorally depending upon impact and site of fracture. q Loss of function or interference with function-Mastication problem, speech and difficulty in swallowing.

• Paresthesia/ hypoesthesia of lower lip- fracture between mental foramen and ramus region • Radiographic evidence-all suspected cases must be radiographed. help as diagnostic aid and addition confirmation also for medico legal documentation and as evidence.

FACIAL ASYMMETRY Facial deformity

Fracture Sites Anatomical • • Dento alveolar Condylar Coronoid Process Ramus Angle Body Symphysis & para symphysis Comminuted fracture

Dent alveolar Fracture • Avulsion/subluxation or fracture of tooth in association with fracture of alveolus. • DA fracture alone • DA plus mandibular fracture

Soft tissue Injuries • Laceration, full thickness wound of lower lip-imp low teeth • complete loss of soft tissue • Bruising with embeded tooth portion/ foreign body • Alv margin-laceration of gingiva, deformity of alveolus • Degloving injury

Laceration of Lip & cheek

Degloving injury Mandible • Impaction of point of chin on some resilient surface-soft earth • Jaw does not fracture but soft tissue rotated violently over point of chin. horizontal tear at junction of attached & free gingiva

Damage to tooth • Tooth- lost, recent extn wound-knocked out • Split/ Fracture- premolar & Molars- horizontal / vertical split below the gingival margin-indirect trauma from opposing dentition • Crown- fracture, embedded into soft tissue, swallowed or inhaled.

Tooth injuries • • • If pulp/near pulp exp-immediate treatment Root- fracture, excessive mobile tooth, subluxated ? IOP Xrays Thermal sensitivity-unreliable to test injury to pulp Trauma/ force –disturb the function of nerve endings

Alveolar Fracture • • • Isolated fracture With injury to tooth Gross comminution of Alveolus Alv fracture consists one or two fragments containing teeth Complete Alv Fr+ Teeth segment displaced into soft tissue of the floor of mouth covered by mucosa.

AVL Fracture • +-Difficult to differentiate alveolar fracture from symphysis fracture • Unless palpate at lower border of mandible. • During examn easy to reposition the alveolar fracture fragment in position-better prognosis.
 • Easily missed")
Condylar Fracture • Most common overall fracture ( 20 % ) • Easily missed fracture during examination
.")
Condylar # • Unilateral / Bilateral • Intra capsular / Extra capsular( condylar Neck). • Extra capsular type-with or without dislocation

Unilateral Condylar Fracture • Inspection • Swelling over joint - + • bleeding from ear( laceration of antr wall of EAM • D/D-bleeding from middle ear +CSF otorrhoea- Petrus temporal bone # • Ecchymosis of skin below mastoid process-when hematoma surrounding fractured condyle tracked down to EAM. • D/D Battle Sign ( Base of Skull # ) • If mandible locked- when condyle impacted through glenoid fossa

Inspection • If condyle medially dislocated-when edema subsided hollow characteristic sign will be present • Immediate post trauma-sign obscured by edema.

Contd • Tenderness over condylar area • EAM palpation –when condyle is dislocated from glenoid fossa. (standing in front of pt both little can be hooked into each EAM ). • Rarely hemorrhage from condylar region track across the base of skullexert pressure on mand. Divin. Of Vth N at F. Ovale-paresthesia of lower lip • D/D-Fracture of Body / Angle region of mandible rule out

INTRAORALLYCondyle dislocated resulted ramus height shortening. Molar gagging of the occlusion. Deviation of mandible towards fracture side. Painful movements- Lateral excursion to opposite side -Protrusive movement.

Bilateral • Extra orally- same sign & symptoms bilaterally • Mandibular movement restricted. • Intra orally • In intra capsular fracture bilaterally- if any ramal shortening but normal occlusion. • Extracapsular #- b/L condylar dislocation- B/L ramus shortening /overriding of fracture fragments- Antr open bite. • Painful & limited opening movements. • Painful & restricted protusion n lateral excursions

Bilateral condylar fracture

Guard man fracture- B/L condylar fracture with Symphy or Parasymphysis fracture

Coronoid process Fracture • Rare fracture • Result from reflux contracture of powerful antr fibres of temporalis muscle. • Direct trauma to ramus- # coronoid process • Tip #-pulled upwards into infratemporal space ( Temp M ) • Sometime- surgery of cyst r large tumor of the ramus. • Palp-tenderness over antr part of ramus, tell-tele hematoma • Painful, limited protrusive movement.

Fracture of the Ramus • Not common- two types • Single fracture- Low condylar fracture-both condyle & coronoid process on upper fragment. • Comminuted Fracture- direct violence from gun shot/missile injury- fragments splinted between masseter muscle and medial pterygoid muscles with little or no displacement.

CLINICAL FEATURES v Swelling & ecchymosis extra & intraorally. v Tenderness over the ramus. v Severe trismus present ?

Fracture of Angle • Inspection. Swelling Facial deformity I/O step deformity behind last molar Presence of hematoma Buccal r lingual side or both adjacent to fracture. v Anesthesia or paresthesia of the lower lip. v Occlusion-deranged. v v

Swelling

Angle Fracture

Contd • Palpationq Tenderness present at angle region q Movement /crepitus at fracture site ( if ramus steadied between finger and thumb and body of mandible moved gently with the other hand). q Step may palpated. q Painful restricted jaw movements.

Fracture of the Body( Molar & Premolar region • Swelling • Tenderness • Displaced fractured fragment, causes derangement of occlusion • Premature contacts in distal fragment (displacing action of muscles attached to Ramus) • Occlusion Derangement. • Gingival tear due to its firm attachment -displaced fragments

• If gross displacement can cause Intra oral hemorrhage -IAA torned ? • Molar & Premolar toothsplit longitudinally / vertically- considerable discomfort

Body Fracture Muscle influence causing displacement Displaced fract fragment

Symphysis & Parasymphysis • Commonly associated with one /both condyle. • Presence of bony tenderness & lingual hematoma important sign • Bec antr mandible thickness between often ensure fine cracks with little displacement. • May be missed if occlusion is undisturbed locally. •

contd § Bony tenderness and small lingual hematoma may be only physical sign present § Severe impact( direct violence-oblique fracture-displaced fragments. Which allows over riding of the fragments with lingual inversion of the occlusion on each side. § Always associated soft tissue injury of chin and lower lip

contd • Detachment of genioglossus M – may contribute loss of tongue control. • Airway obstruction. • If Pt Conscious- voluntarily control of tongue prevent obstruction. • If unconscious- stay suture of tongue/airway to prevent tongue fall. • No paresthesia of skin of mental region unless mental nerve is involved.

Parasymphysis plus angle fracture transverse width , condyle dislocated cross bite,

21 th AUG 2015
- Slides: 86