Clinical Dilemma Which Adjuvant Chemotherapy is Just Right









 CEF (NCIC-CTG)")
 (2) (3) (4) (5) (6) (1) (2)")
 AC (1970’s) (1980’s)")






 %")


 NSABP B")
















- Slides: 58
Clinical Dilemma: Which Adjuvant Chemotherapy is Just Right? Dr. Maureen Trudeau Head, Division of Medical Oncology/Hematology Toronto Sunnybrook Regional Cancer Centre Associate Professor, University of Toronto June 15, 2007
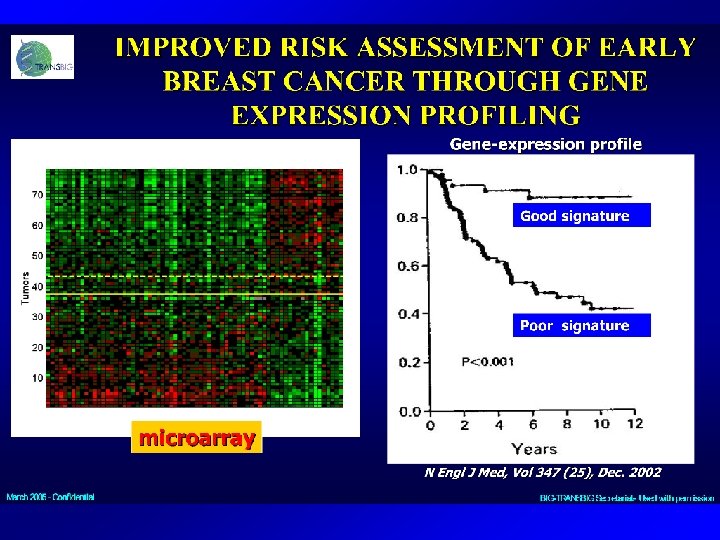
Systemic Therapy - Chemotherapy • Overall survival improvement in clinical trials both for standard and newer treatments • Choice – for patients, for physicians (anthracycline +/- taxanes) • Better decision making aids – www. adjuvantonline. com • Molecular profiles – Oncotype Dx, Mammo. Print • Improved supportive care
Decision Making in Adjuvant Therapy Tumour characteristics T, N, Grade, ER, Pg. R, Patient Characteristics Age, Comorbidities HER 2, LVI Prior Therapy Performance Status Patient Preference Work/Family/Self Molecular Profile Clinical Trials, Guidelines Recent Reports
Select Breast Cancer Treatments Based on Tumor Phenotype • Tumor phenotype defines treatment options Hormone receptor Positive Hormonal therapy Negative Chemotherapy HER 2 Positive HER 2 -targeted therapy Negative
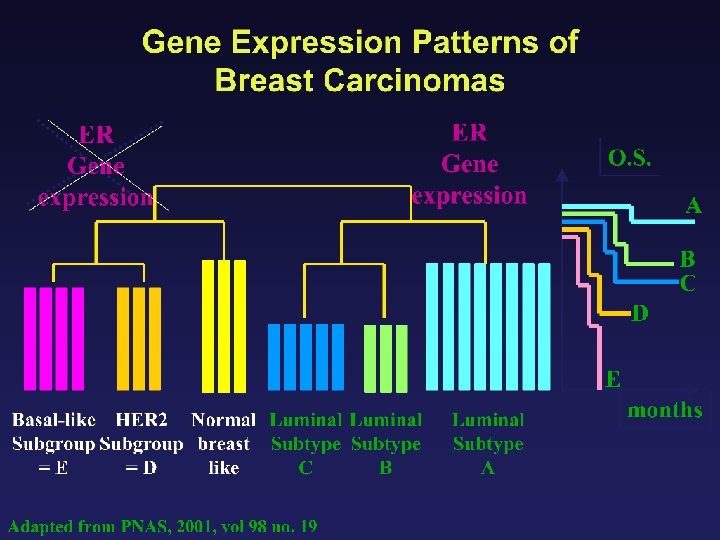
Breast Cancer is not ONE Disease Basal-like HER-2 “Normal” Luminal B Luminal A Sorlie T et al, PNAS 2001
ER+ 65 -75% All Breast Cancer HER 2+ 15 -20% Basaloid 15%
Molecular Classifications of Breast Tumors Luminal A ER + high Prolif - P 53 mutations 16% Luminal B + 71% Basal -like ER + low ER - + ERBB 2 + Normal-like ER-/+ ER - -/+ - 75%, also BRCA 1 86% Sorlie 2007
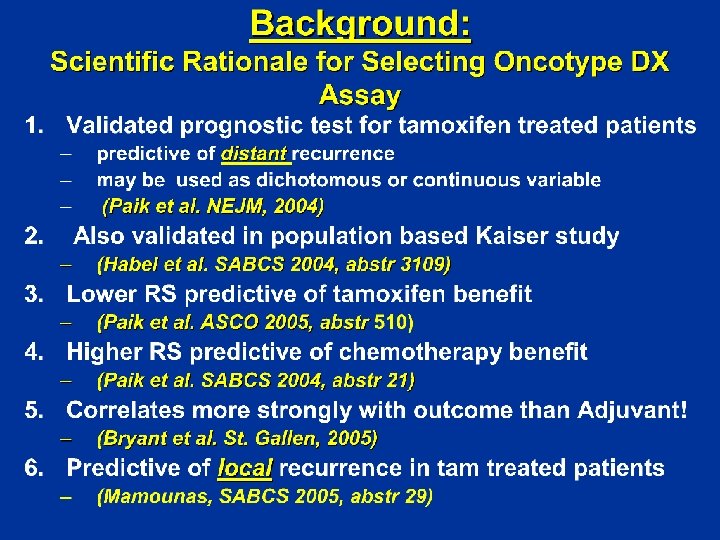
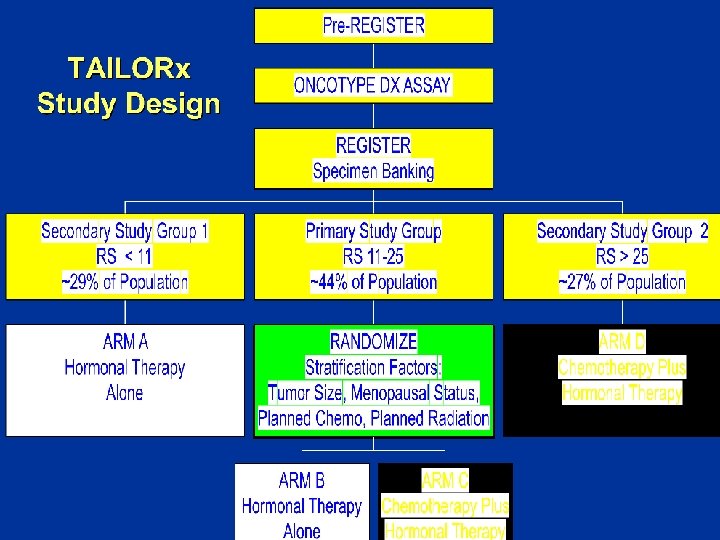
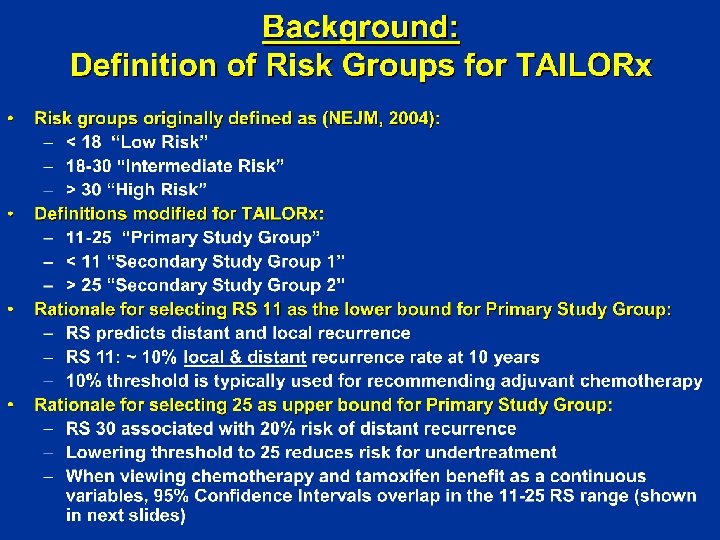
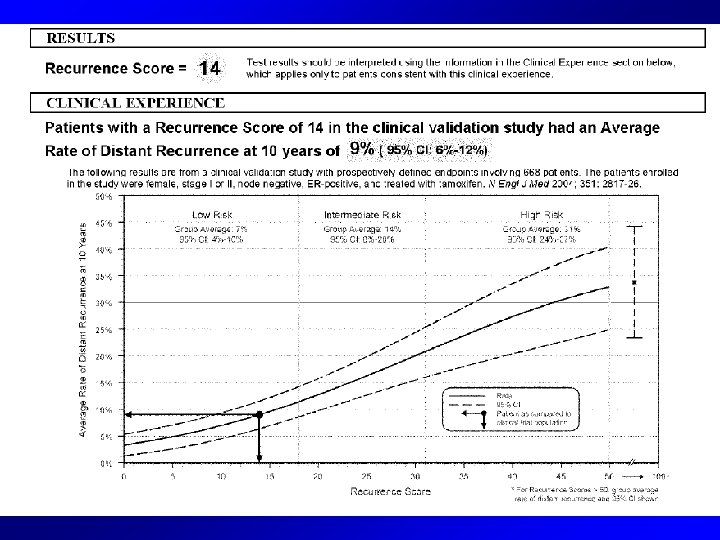
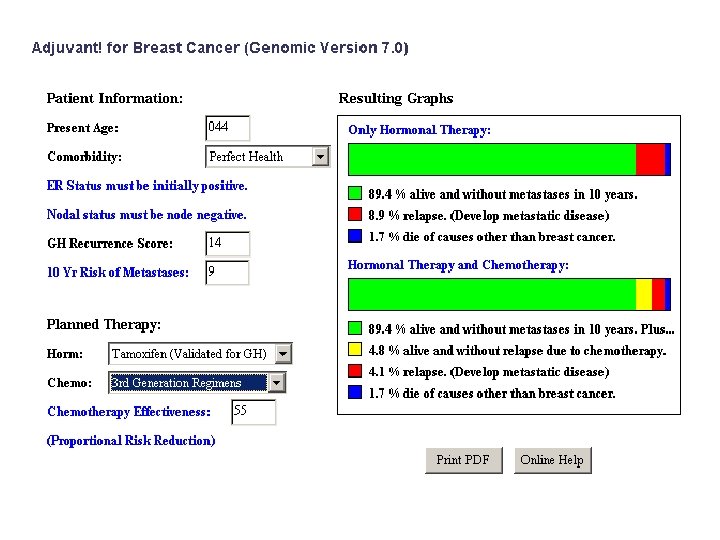
Oncotype DX • A multigene assay to predict recurrence of Tamoxifen-treated, node-negative breast cancer (Paik NEJM 204) • 21 genes - proliferation (5), invasion (2), HER 2 (2), Estrogen (4) , 3 others and 5 reference genes with a Recurrence Score (RS) algorithm • For node negative, tam treated (JCO 2007): –Luminal A = low risk oncotype DX –Luminal B = mod/high risk
Adapted by Dr. Maureen E. Trudeau, MD
Anthracycline-based Regimens Superior To CMF/AC Regimen Trials Group. DFS / OS (1) CEF (NCIC-CTG) (2) dd (EC) CEF (3) FEC 100 > FEC 50 (FASG) FEC 50 CMF (ICCG) -- -- (4) CAF (SWOG) (5) E CMF (NEAT/SCTBG) (6) AV CF (7) TC (NCIC/EORTC/SAKK) (MISSET) (Jones) -- -- --
Taxane Regimens Superior To AC-type Regimens (1) (2) (3) (4) (5) (6) (1) (2) Regimen Trials Group DFS / OS AC P (CALGB) AC P (NSABP) -P FAC (MDACC) -- -DAC (BCIRG) FEC D (PACS 01) A(C) D CMF (BIG 2 -98) Regimens superior to AC P dd AC P (CALGB) or dd A P C CEF or dd (EC) P --
Adjuvant Chemotherapy Options – A Growing List 1998 CMF Options (F) AC (1970’s) (1980’s) 2007 Options CEF (CMF) FEC 100 (FEC 50) AC Taxol (AC) TAC (FAC) FEC 100 Docetaxel (FEC 100) Dose-dense AC Taxol (AC Taxol) Dose-dense (AC Taxol) (EC) Taxol CEF (AC Taxol)
TAXANES AS ADJUVANT THERAPY SECOND GENERATION OF CLINICAL TRIALS Best taxane ECOG 1199 (intergroup trial) N 5000 AC x 4 Px 4 AC x 4 P weekly x 12 2800 pts AC x 4 Dx 4 AC x 4 D weekly x 12
Are There Factors that May Predict Response or Suggest which Therapy to Use?
TAXANES AS ADJUVANT THERAPY SECOND GENERATION OF CLINICAL TRIALS Taxane ± Herceptin® • HERA: any chemo Herceptin: 0 vs 1 vs 2 yr • AC D vs AC D + H 1 yr vs DCH x 6 H 1 yr • AC P vs AC P + H 1 yr N 8700 • AC P weekly x 12 vs AC P weekly x 12 H 1 yr vs AC P weekly x 12 + H 1 yr
Trastuzumab DFS Median follow-up HERA 1 year Combined analysis 2 years DH 2 years BCIRG 006 DCarbo. H 2 years BCIRG 006 AC Fin. HER VH / DH 3 years CEF 0 Favors Trastuzumab 1 Favors no 2 Trastuzumab HR Piccart-Gebhart et al 2005; Romond et al 2005; Slamon et al 2005; Joensuu et al 2005
Adjusted for pos nodes, T size, menopausal status Courtesy: Berry et al SABCS 2004
PACS 01 DFS by Age, ITT Age 50 yrs Age < 50 yrs 1. 00 3 FEC 100 -3 D 0. 75 Kaplan-Meier Estimate 3 FEC 100 -3 D 6 FEC 100 0. 50 Log-rank P-Value = 0. 690 HR (Cox model) = 0. 98 [0. 77 -1. 25] 0. 25 6 FEC 100 0. 50 Log-rank P-Value = 0. 001 HR (Cox model) = 0. 67 [0. 51 -0. 88] 0. 25 Multivariate Interaction Test HR: 0. 66 [0. 46 -0. 95] P-value = 0. 026 0. 00 0 1 2 3 4 5 6 Survival Time (years) 7 8 0 1 2 3 4 5 Survival Time (years) 6 7 8
TAC vs FAC DFS by HER 2 Status (Centrally reviewed, FISH centrally reviewed) % Alive and Disease-Free 100 Negative 90 100 Positive 90 80 TAC FAC 70 60 HR = 0. 76 P = 0. 046 50 70 60 HR = 0. 60 P = 0. 0088 FAC 50 0 6 12 18 24 30 36 42 48 54 60 66 Time to First Event Ratio of HRs 0. 85 p= 0. 4122 NEJM 2005
Topoisomerase II • Topoisomerase II is essential for DNA replication and recombination • Anthracyclines target topoisomerase II • Increased sensitivity to HER 2 due to coamplification of TOP 2 A?
A pooled analysis on the interaction between HER-2 expression and responsiveness of breast cancer to adjuvant chemotherapy Alessandra Gennari, Maria Pia Sormani, Matteo Puntoni and Paolo Bruzzi National Cancer Research Institute - Genoa and University of Genoa - Italy SABCS 2006
Characteristics of studies - I Study Comparison HER 2 status determined (%) NSABP B 11 PF vs PAF 638/682 (94%) NSABP B 15 CMF vs AC 2. 034/2. 295 (89%) GUN 3 CMF vs CMF/EV 123/220 (56%) Brussels CMF vs HEC/EC 354/777 (46%) Milan CMF vs CMF→ A 506/552 (92%) DBCCG - 89 - D CMF vs FEC 805/980 (82%) NCIC MA 5 CMF vs CEF 628/710 (88%) 5. 088/6. 216 (82%) Total (available/randomised) SABCS 2006
Disease Free Survival HER 2 positive HER 2 negative Study HR 95% CI NSABP B 11 0. 60 0. 96 0. 84 1. 02 0. 65 1. 35 0. 83 1. 22 0. 75 0. 79 0. 52 0. 91 0. 44 - 0. 82 0. 75 - 1. 23 0. 65 - 1. 08 0. 86 - 1. 20 0. 34 - 1. 27 0. 93 - 1. 97 0. 46 - 1. 49 0. 91 - 1. 64 0. 53 - 1. 06 0. 60 - 1. 05 0. 34 - 0. 80 0. 71 - 1. 17 Total 0. 90 0. 82 - 0. 98 p = 0. 01 Overall 0. 71 1. 00 0. 61 - 0. 83 0. 90 - 1. 11 p < 0. 0001 p = 1. 0 NSABP B 15 Brussels Milan DBCCG-89 -D NCIC MA-5 heterogeneity 25 = 5. 3, p = 0. 38 heterogeneity 25 = 7. 6, p = 0. 18 anthra better 0. 4 0. 6 0. 9 non anthra better 2 1 5 Test for interaction 2 = 13. 7 p < 0. 001 SABCS 2006
Efficacy summary HER 2 positive • Risk of relapse HER 2 negative • Risk of relapse 29% anthra ≈ non anthra HR 0. 71 (0. 61 -0. 83) HR 1. 00 (0. 90 -1. 11) (p < 0, 0001) (p = 1, 0) • Risk of death 27% anthra ≈ non anthra HR 0. 73 (0. 62 -0. 85) HR 1. 03 (0. 92 -1. 16) (p < 0, 0001) (p < 0, 86) SABCS 2006
Hierarchy of Chemotherapy Regimens Appropriate high risk population Older, no GCSF Younger, +/- GCSF Younger, + GCSF # of cycles 6 cycles 10 cycles 6 cycles (12 visits) 8 cycles 6 cycles High risk FEC D dd(EC) P CEF dd(AC) P TAC FEC 100 CEF (MA 5) FEC 50 CMF is better than Moderate risk CAF AC AC P AC AC DC AD is better than Low Risk P = paclitaxel D = docetaxel No Therapy FAC
The choice of chemotherapy Depends on the following: • Tumour characteristics and risk of relapse • Patient comorbidities • Patient age • Social determinants • Drug availability / costs • Physician or patient preference
Cost of common regimens Regimen N+ Study Total Treatment Costs USD (drug acquisition + incidental + administration) DAC AC ->P AC->P CE 120 F FE 100 C->D BCIRG 001 CALGB 9344 CALGB 9741 MA-5 FASG-5 PACS-01 $8, 226 $4, 340 $11, 741 $4, 852 $3, 557 ~ $6, 200
Convenience of common regimens Regimen N+ Study TAC BCIRG 001 AC ->T CALGB 9344 AC->T CALGB 9741 CE 120 F MA-5 FE 100 C FASG-5 FE 100 C->D PACS-01 Visits 6 8 8 12 6 6 Chair time (h) 14 21. 6 5. 4 9 8
Where are we going? Adapted by Dr. Maureen E. Trudeau, MD
Cases
A 68 -year old woman presents with an infiltrating duct carcinoma • 1. 2 cm in size • ER 80% PR 60% • HER 2 • Sentinel node negative
A 68 -year old woman presents with an invasive ductal carcinoma
A 59 -year old postmenopausal woman with invasive ductal carcinoma • 1. 9 cm in size • ER 30% PR 0% • HER 2+ (3+ by IHC) • Grade 3 • Sentinel node negative
A 59 -year old postmenopausal women with invasive ductal carcinoma
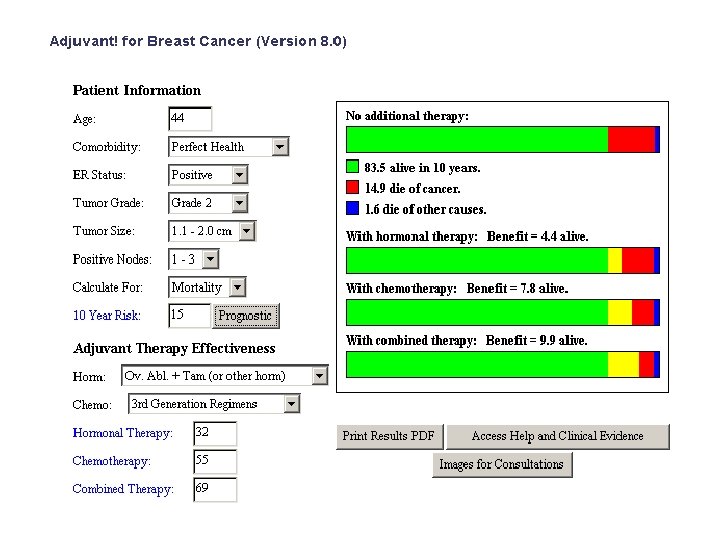
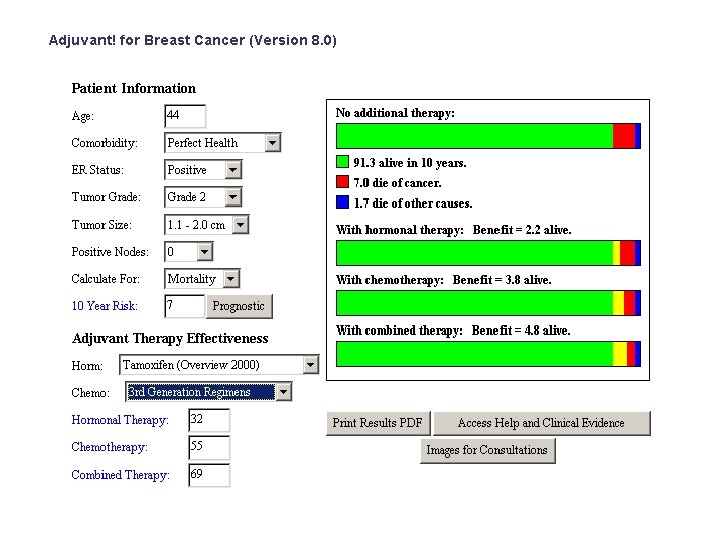
A 49 -year old premenopausal woman with invasive lobular carcinoma • 2. 5 cm in size • ER 70% PR 30% • HER 2 • Grade 2 • 2/10 positive lymph nodes
A 49 -year old premenopausal woman with invasive lobular carcinoma
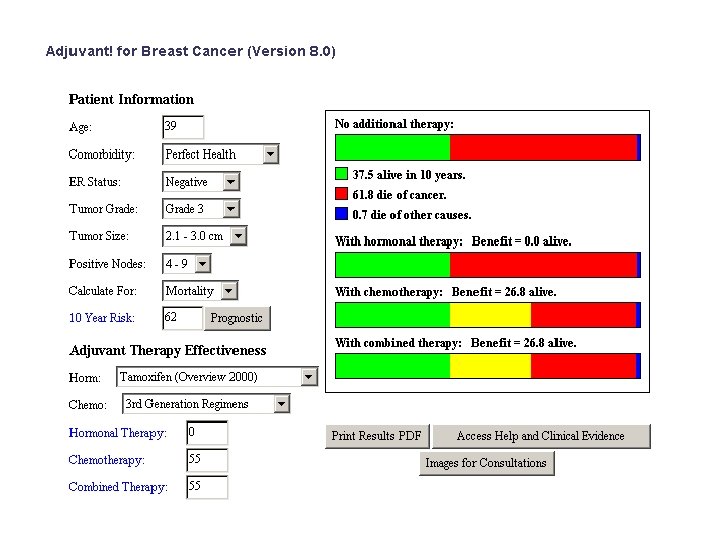
A 39 -year old premenopausal woman with invasive ductal carcinoma • 2. 8 cm in size • ER 0% PR 0% • HER 2 • Grade 3 • 5 nodes positive
A 44 -year old premenopausal woman with invasive ductal carcinoma • 2. 0 cm in size • ER 100% PR 100% • HER 2 • Grade 2 • 1/17 nodes positive • 2 other smaller lesions, grade 1