Clinical Chemistry of Parathyroid disorders BONE H 2

Clinical Chemistry of Parathyroid disorders
2 x(PO")
BONE H 2 O Inorganic Ca-hydroxyapatite Ca 2+ 10 -x (H 3 O+)2 x(PO 4 3 -)6(OH-)2 osteocalcin osteonectin osteopontin Organic (osteoid) Proteoglycans lipids 12% collagen (type I) 88%
 - potentiate and")
CELLS IN BONE 1. Osteoblast - production of organic matrix (osteoid) - potentiate and control mineralisation - potentiate production of alkaline phosphatase 2. Osteocyte - connection with extracellular fluid - regulation of Ca and Pi movement between bone and extracellular fluid 3. Osteoclast - polynuclear specific macrophages - bone resorption
 - - Ca 2+ - -")
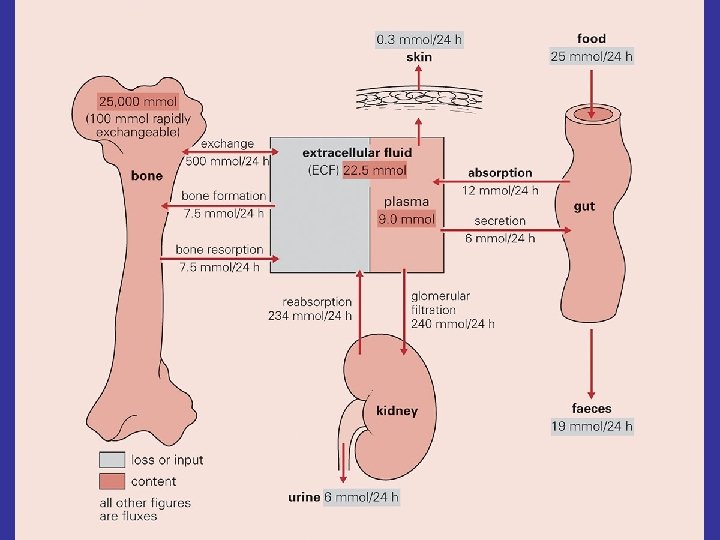
Ca 2+ - - - PROTEIN - (albumin) - - Ca 2+ - - Anion Ca 2+ Anions HCO 3 H 2 PO 4 HPO 4 -2 Citrate Lactate Ca 2+ Protein bound calcium 46% Free calcium 47% Complexed calcium 7% Total calcium (2. 1 -2. 6 mmol/l)
 parathyroid glands • Calcitriol -")
Hormones regulating plasma calcium concentration • Parathyroid hormone (PTH) parathyroid glands • Calcitriol - 1 -25 DHCC (active vitamin D) Formed after hydroxylation! (liver, renal) • Calcitonin (thyreoidea C cells) Its physiological function is not well characterized
 • Polypeptide (84 amino acids) • Product of chief cells")
A parathyroid hormone (PTH) • Polypeptide (84 amino acids) • Product of chief cells of parathyroid glands • N-terminal 34 AA fragment and intact PTH are biologically active • increase of serum Ca 2+ decrease of serum phosphate

Half life: 3 -4 min Half life: 2 -3 hours

Target organs for PTH • Bone: Ca and Pi resorption by osteoclasts • Kidney tubular Ca reabsorption tubular Mg reabsorption tubular P reabsorption tubular HCO 3 reabsorption • Intestine 1 -25 DHCC production in kidneys

PTH regulation and mechanism of action Stimulatory effects: Inhibition: Se Ca 2+ Mild hypomagnesaemia PTH release Se Ca 2+ Severe hypomagnesaemia Calcitriol PTH binding to the target cell receptors (Mg dependent) Adenylate cyclase c. AMP Ca 2+ cellular influx to the target cells
")
Abnormal functions of parathyroid glands • Hyperparathyroidism Primary Secondary (PTH increase is physiological response) Tertiary (autonome PTH secretion) • Hypoparathyroidism Congenital/acquired Pseudohypoparathyroidism

Secondary hyperparathyreoidism A/ With osteomalacia or rickets a. Decrease of Ca and vitamin D uptake or absorption Ca, vitamin D deficient diet, Steatorrhoea or malabsorption b. Defect in production of active vitamin D Chronic renal failure Chronic hepatopathia lack of alpha hydroxylation c. Increased inactivation of vitamin D anticonvulsive therapy d. Lack of 25 HCC transport protein e. D vitamin receptor defect B/ Without osteomalacia and rickets a. acute pancreatitis b. neonatal hypocalcaemia

Typical biochemical features of hyperparathyroidism Primary Se Ca 2+ Secondary Tertiary or N Phosphate or Alkaline phosphatase N or PTH N or or

Parathyroid hormone-related peptide • It is elevated in 50 -90% of patients with hypercalcemia associated with malignancy • Its gene on chr 12 (PTH gene on chr 11) • 3 isoforms • N terminal end shows homology to PTH • Can bind to PTH receptors and mimic its biological action

Serum calcium Normal or decreased Increased PTH Increased Normal Decreased Secondary HPT Primary HPT Tumor hypercalcemia Other causes of Hypercalcemia Creatinine Increased Normal Renal disease Other causes of secondary HPT
 - Pseudohypoparathyroidism Acquired")
Hypoparathyreoidism Congenital e. g. Di. George synd. (immunodeficiency + thymic aplasia) - Pseudohypoparathyroidism Acquired 1/ 2/ 3/ 4/ Operation a. total or partial thyroidectomy b. laryngectomy c. parathyroidectomy Autoimmune disorder Haemochromatosis infiltrative states

Pseudohypoparathyroidism Hereditary disorders, plasma PTH are elevated, but superficially resembles hypoparathyroidism Type 1 Activation of adenyl cyclase is defective and cyclic AMP is not formed Rounded face and skeletal abnormalities, learning difficulties Type 2 c. AMP is formed, but the responses to it are blocked Differentiation: Urinary c. AMP after PTH: elevated in type 2

Typical biochemical features of hypoparathyroidism True Pseudo Se Ca 2+ Phosphate Alkaline phosphatase PTH N N

Calcitriol • Derived from Vitamin D by successive hydroxylation UV 7 -dehydrocholesterol Cholecalciferol Liver 25 -(OH)-Cholecalciferol (Calcidiol) Kidney 1, 25 -(OH)2 Cholecalciferol (Calcitriol) 24, 25 -(OH)2 Cholecalciferol
")
Regulation of hydroxylation in the kidney Synthesis of a Ca 2+-binding protein (calbindin D) Longer term stimulatory effect: GH, prolactin, estrogen

Calcitriol Effects: • Ca and P absorption from intestine • Ca and P resorption from bones by osteoclasts • Receptors of calcitriol in other tissues • Cellular differentiation (normal and malignant cells) • Immunomodulatory effect : Stimulation of production of cytokines

Calcitonin • Polypeptide hormone • Thyreoid C cells • Its physiological function is unknown / under investigation after total thyreoidectomy no clinical symptoms! calcium homeostasis is normal • Its level is elevated pregnancy lactation • Has been detected gut CNS (neurotransmitter) • Experimentally inhibit osteoclast activity, thus bone resorption • Clinical significance medullary carcinoma, small cell cc
- Slides: 23