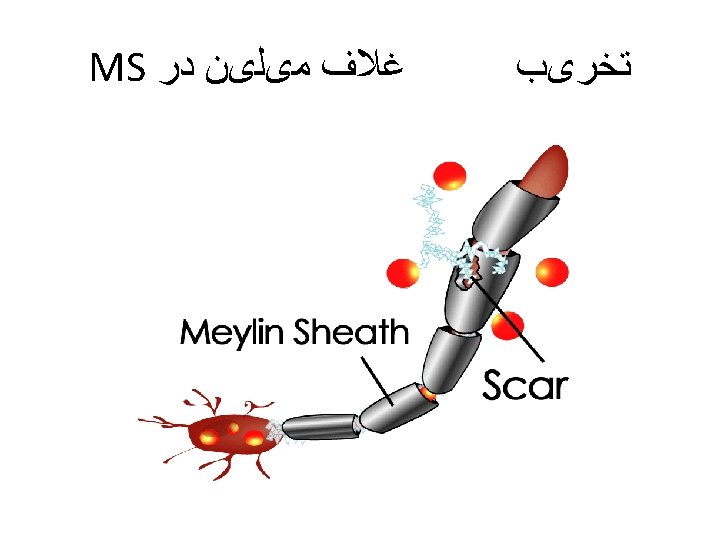
Client with Multiple Sclerosis Description Chronic demyelinating disease






, cyclophosphamide (Cytoxan) § Cychophosphamide §")





- Slides: 19
Client with Multiple Sclerosis Description -Chronic demyelinating disease of CNS associated with abnormal immune response to environmental factor Initial onset followed by total remission making diagnosis difficult - Most persons have disease with periods of exacerbations and remissions -Progression of disease with increasing loss of function - Incidence is highest in young adults (20 – 40); onset between 20 – 50 -Affects females more than males - More common in temperate climates -Occurs mainly in Caucasians
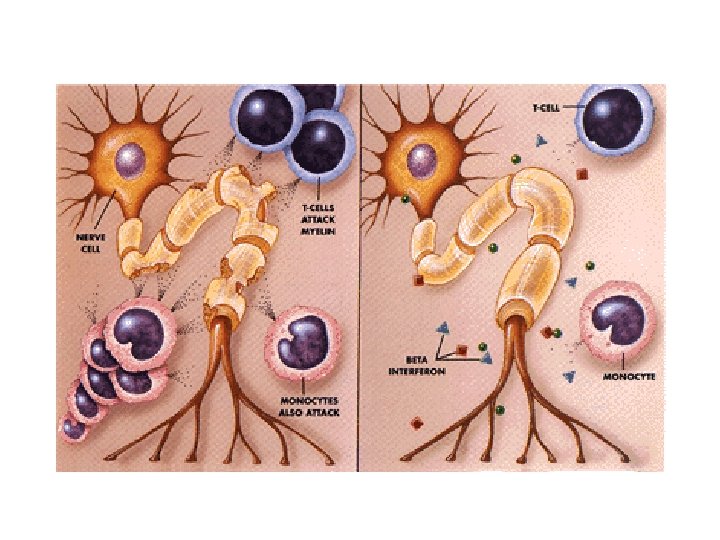
Pathophysiology Autoimmune response to prior viral infection Inflammation destroys myelin leading to axon dysfunction Myelin sheaths of white matter of spinal cord, brain, optic nerve destroyed in patches called plaques Demyelination slows and distorts nerve conduction resulting in absence of impulse transmission Neurons in spinal cord, brain stem, cerebrum, cerebellum, and optic nerve affected Recurrent demyelination and plaque formation result in scarring of glia and degeneration of axons Disease follows different courses, most common is the relapsing-remitting type Stressors trigger MS: febrile states, pregnancy, physical exertion and fatigue; and these also can trigger relapses
Manifestations 1. Fatigue 2. Optic nerve involvement: blurred vision, haziness 3. Brain stem involvement: nystagmus, dysarthria (scanning speech), cognitive dysfunctions, vertigo, deafness 4. Weakness, numbness in leg(s), spastic paresis, bladder and bowel dysfunction 5. Cerebellar: nystagmus, ataxia, hyptonia 6. Blindness
Collaborative Care Focus is on retaining optimum functioning, limiting disability
Diagnostic Tests • Neurological exam, careful history • Lumbar puncture with CSF analysis: increased number of T lymphocytes; elevated level of immunoglobulin G (Ig. G) • Cerebral, spinal optic nerve MRI: shows multifocal lesions • CT scan of brain: changes • PET: measures brain activity • Evoked response testing of visual, auditory, somatosensory impulses show delayed conduction
Medications § ACTH § Glucocorticosteroids § Immunosuppressants: azathioprine (Imuran), cyclophosphamide (Cytoxan) § Cychophosphamide § Antispasmodics to treat muscle spasms § Medications to deal with bladder problems: anticholinergics or cholinergics depending on problem experienced by client
Rehabilitation • Physical therapy to maintain abilities and deal with spasticity
Health Promotion • Client needs to develop strategies to deal with fatigue, exacerbations • Prevention of respiratory and urinary tract infections
Nursing Diagnoses • Fatigue • Self care deficits
Home Care • Education • Referral to support group and resources • Referral to home health agencies when condition requires