Clavicle fracture Frequency Clavicle fractures involve approximately 5









- Slides: 12
Clavicle fracture
Frequency • Clavicle fractures involve approximately 5% of all fractures seen in hospital emergency admissions. Clavicles are the most common broken bone in the human body. It is most often fractured in the middle third of its length. Children and infants are particularly prone to it. Newborns often present clavicle fractures following a difficult delivery.
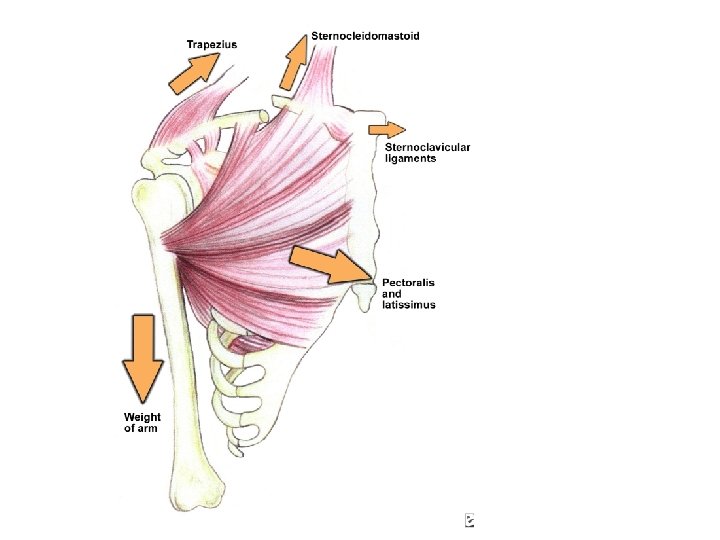
displacing forces • After fracture of the clavicle, the sternocleidomastoid muscle elevates the proximal fragment of the bone. The trapezius muscle is unable to hold up the distal fragment owing to the weight of the upper limb, and thus the shoulder droops. The adductor muscles of the arm, such as the pectoralis major, may pull the distal fragment medially causing the bone fragments to override.
Presentation • Because of the clavicle's subcutaneous position, injury is often obvious and is confirmed at the time of initial observation. Despite the relatively simple diagnosis, some aspects of clavicle fractures must be addressed. In particular, note any skin abrasions or other wounds in proximity to the fracture site to determine if the fracture is an open injury. Note any tenting of the skin, as this will likely cause pressure necrosis of the skin and an increased chance that the fracture will become an open injury.
• In addition to observing the status of the skin, perform a complete neurovascular examination of the involved extremity, including comparative blood pressure measurements if injury to the subclavian artery is suspected. Keep in mind that the excellent collateral circulation to the upper extremity mask injury to the subclavian artery. The subclavian vessels and brachial plexus run in close proximity to the clavicle and are at risk for injury with displaced clavicle fractures
Treatment • Treatment usually involves resting the affected extremity and supporting the arm with the use of a sling. In older practice, a figure-8 brace was used, designed to immobilize and retract the shoulder, maintaining symmetric positioning to facilitate healing. monitoring progress with X-rays every week or few weeks. Surgery is employed in 510% of cases
Surgery • More than 90% of clavicle fractures are successfully healed by non-operative treatment. The surgery is indicated when one or more of the following conditions presents. • Comminution with separation (multiple piece) • Significant Foreshortening of the clavicle (indicated by shoulder forward). • Skin penetration (Open Fracture). • Clearly associated nervous and vascular trauma (Brachial Plexus or Supra Clavicular Nerves). • Non Union after several months (3– 6 months, typically) • Distal Third Fractures which interfere with normal function of the ACJ (Acriomio Clavicular Joint).
• Typical surgical complications are infection, neurological symptoms distal the incision (sometimes to the extremity), and non-union requiring re-plating.
• Healing time varies based on age, health, complexity and location of the break as well as the bone displacement. For adults, a minimum of 3– 4 weeks of sling immobilization is normally employed to allow initial bone and soft tissue healing, teenagers require slightly less, children can often achieve the same level in two weeks. During this period, patients may remove the sling to practice passive pendulum ROM exercises to reduce atrophy in the elbow and shoulder, but they are minimized to 15 -20 degrees off vertical.