Classification of Periodontal Diseases Dr Enas Razzoqi B

Classification of Periodontal Diseases Dr. Enas Razzoqi B. D. S. , M. Sc. , Ph. D in Periodontics

The classification presented in this lecture is at the 1999 International Workshop for the Classification of the Periodontal Diseases organized by the American Academy of Periodontology (AAP).

GINGIVAL DISEASES

1. Dental Plaque-Induced Gingival Diseases plaque induced gingivitis periodontium with no attachment loss on a periodontium with previous attachment loss that is stable and not progressing. І. Gingivitis associated with dental plaque only. I II. Gingival diseases modified by systemic factors III. Gingival diseases modified by medications. IV. Gingival diseases modified by malnutrition

I. Gingivitis associated with dental plaque only A. Without local contributing factors B. With local contributing factors These factors are contributory because of their ability to retain plaque microorganisms and inhibit their removal by patientinitiated plaque control techniques The plaque-host interaction can be altered by the effects of local factors, systemic factors, or both; medications; and malnutrition that can influence the severity and duration of the response.

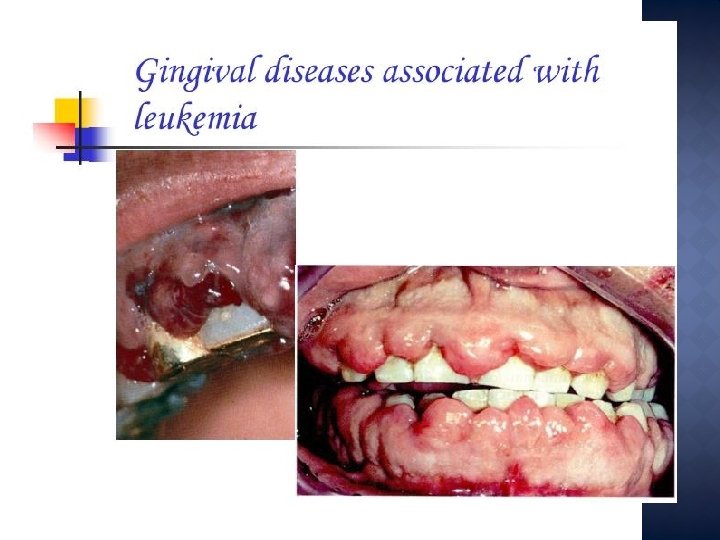
II. Gingival diseases modified by systemic factors A. Associated with endocrine system 1. Puberty-associated gingivitis 2. Menstrual cycle–associated gingivitis 3. Pregnancy associated a. Gingivitis b. Pyogenic granuloma 4. Diabetes mellitus–associated gingivitis B. Associated with blood dyscrasias Leukemia-associated gingivitis This appears to be caused by the effects of the systemic conditions on the cellular and immunologic functions of the host. The prevalence and severity of gingival inflammation may increase even in the presence of little plaque.

hormone exaggerated marginal and papillary inflammation, pyogenic granuloma in pregnant

Leukemia may alter immune function by disturbing the normal balance of immunologically competent white blood cells supplying the periodontium 1. Gingival enlargement and bleeding. 2. may be associated with swollen, spongy gingival tissues caused by excessive infiltration of blood cells. Leukemia

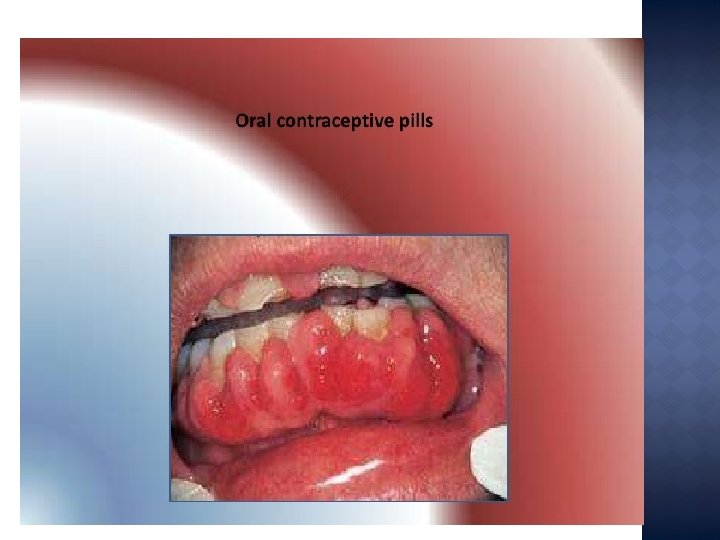
III. Gingival diseases modified by medications A. Drug-influenced gingival diseases 1. Drug-influenced gingival enlargements 2. Drug-influenced gingivitis a. Oral contraceptive–associated gingivitis b. Other phenytoin immunosuppressive drugs such as cyclosporine A kidney trans-plant patient. ) calcium channel blockers such as nifedipine, verapamil, sodium valproate and diltiazem. The development and severity of gingival enlargement in response to medications is patient specific and may be influenced by uncontrolled plaque accumulation. The increased use of oral contraceptives by premenopausal women has been associated with a higher incidence of gingival inflammation and development of gingival enlargement that may be reversed by discontinuation of the oral contraceptive.

severe gingival overgrowth secondary to cyclosporine therapy gingival overgrowth following use a of calcium channel blocker to control hypertension.

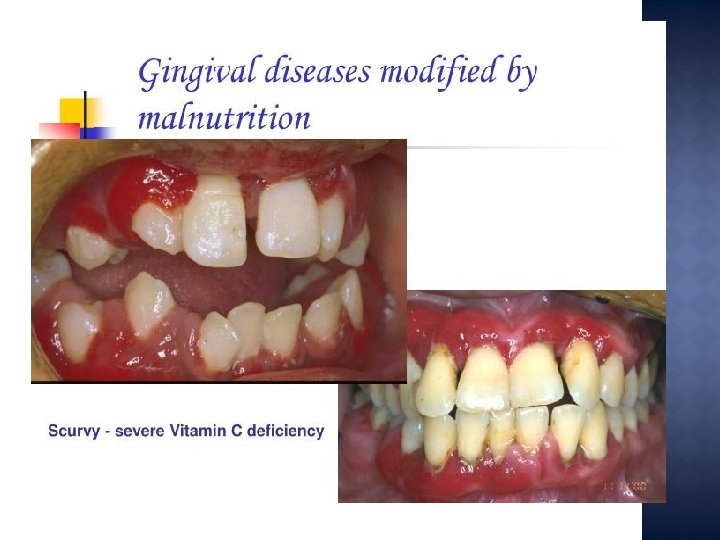
IV. Gingival diseases modified by malnutrition Ascorbic acid deficiency gingivitis Bright red, swollen, and bleeding gingiva. the relative absence of dental plaque Nutritional deficiencies are known to affect immune function and may have an impact on the host's ability to protect itself against some of the detrimental effects of cellular products
- Slides: 15