CLASS 7 25082015 GALACTOCELE Seen in lactating women



. Abscess when formed should be drained under")






Occasionally mutation of BRCA 3 and p 53 suppressor gene is also involved. 3)Li-Fraumen’s")
Attaining early menarche and late menopause Early child bearing and breast feeding reduces the")
Benign breast diseases with atypia, hyperplasia and epitheliosis has got higher risk in a")


 In situ carcinoma DCIS (Ductal carcinoma")

 without any")
.")














 because breast tissue is")


.")



 (70%)—Lumbar vertebrae, femur, ends of long bones, thoracic vertebrae, ribs,")



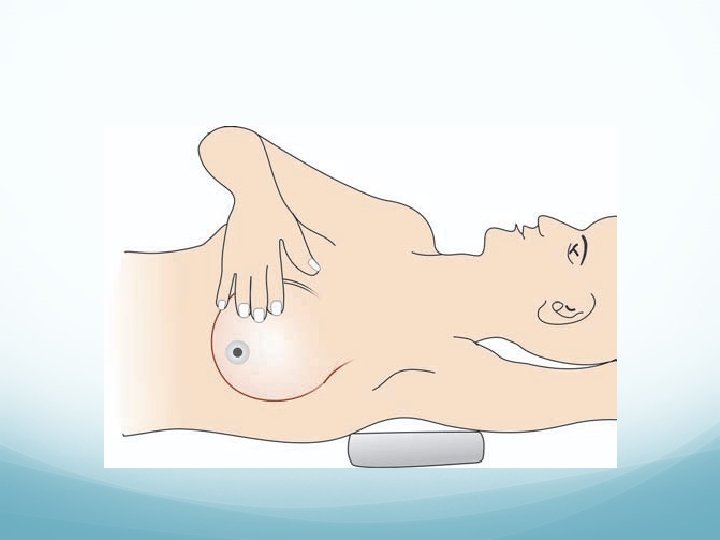
 Plays a major role in early detection and intervention of breast")
- Slides: 50
CLASS 7 25/08/2015
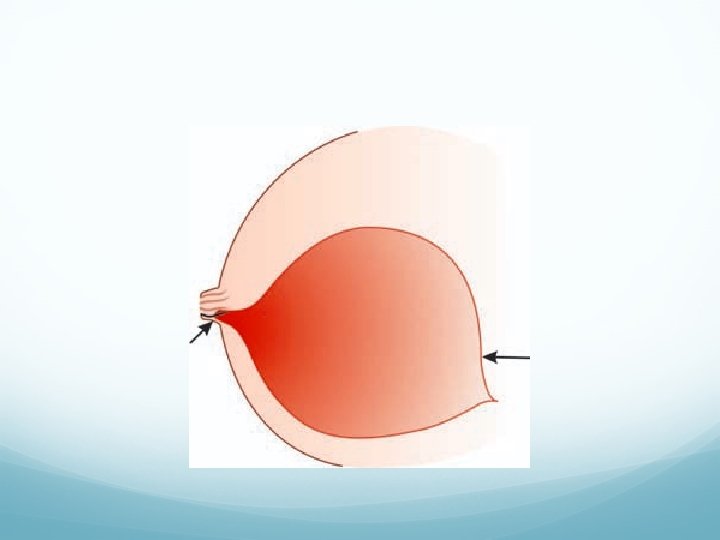
GALACTOCELE Seen in lactating women. It is due to the blockage of lactiferous duct resulting in enormous dilatation of lactiferous sinus. It contains milk within. It is a retention cyst in subareolar region attaining large size.
Clinical Features Lump in the lower quadrant of the breast which is usually unilateral, large, soft, fluctuant, with smooth surface. It is usually nontender. It may get precipitated, inspissated or get calcified. When it is calcified it mimics carcinoma breast. If it gets infected it will form an abscess.
Investigations U/S. FNAC. Treatment Excision (submammary incision). Abscess when formed should be drained under general anaesthesia under cover of antibiotics.
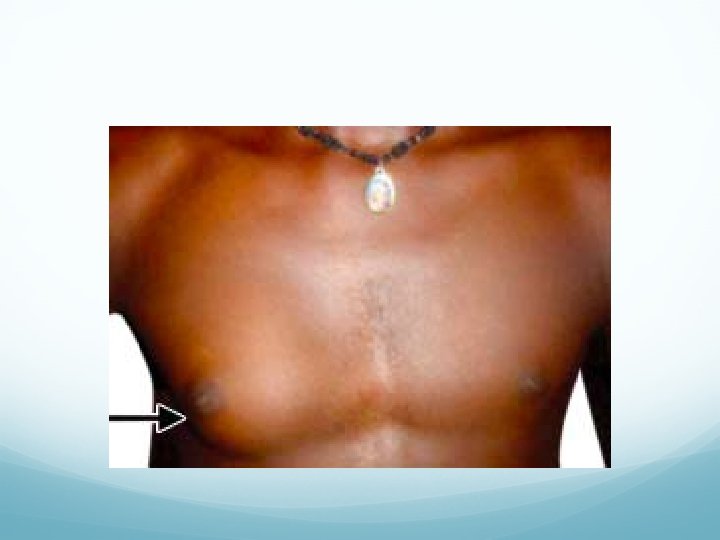
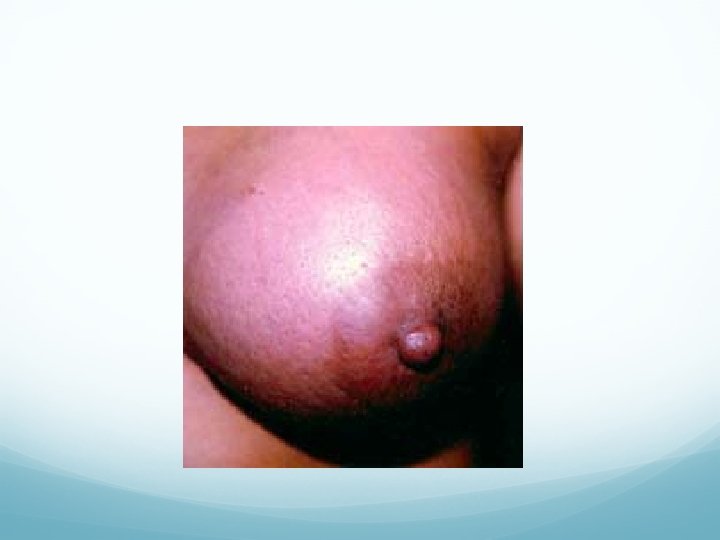
GYNAECOMASTIA It is hypertrophy of male breast more than usual due to increase in ductal and connective tissue elements often attaining features of female breast. It can be unilateral or bilateral.
Presentations Diffuse enlargement of breast occupying all quadrants. Often well-localised, small, firm or hard nodule under the areola which is often painful and tender. Causes Idiopathic Teratoma testis Ectopic hormonal production in bronchial carcinoma
Anorchism, after castration Adrenal and pituitary disease Leprosy, because of bilateral testicular atrophy Drugs: Stilbestrol, digitalis, cimetidine, spironolactone, INH, phenothiazides Liver diseases and liver failure Klinefelter’s syndrome (XXY Trisomy)
Investigations Relevant to the cause, e. g. liver function tests, DNA study, hormone assay. Treatment When symptomatic or large or of long-standing, excision through circumareolar incision is done. For large size subcutaneous mastectomy has to be done.
CARCINOMA BREAST More common in developed, western countries. In African-American women, it is more aggressive. It is less common in japan. It is second most common carcinoma in females. Incidence is 19 -34%. Median age is 47 years. Carcinoma in one breast increases the risk of developing carcinoma on opposite breast by 3 -4 times.
Incidence of bilateral carcinoma is 2%. It is more common after middle age, but can occur at any age group, after 20 years. It can be familial in 2 -5% cases. Predisposing factors 1)Mutation of tumour suppressor genes BRCA 1/ BRCA 2 BRCA 1 mutation is having more risk (35 -45%) than BRCA 2 mutation. It is located in long arm of chromosome 17, whereas BRCA 2 is located in long arm of chromosome 13.
2)Occasionally mutation of BRCA 3 and p 53 suppressor gene is also involved. 3)Li-Fraumen’s syndrome (LFS) is autosomal dominant condition with breast cancer inheritance (90%) along with sarcoma, leukemia, brain tumours, adrenocortical tumours. 4)Diet low with phytoestrogens and high alcohol intake have high risk of breast cancer. 5)It is more common in nulliparous woman.
6)Attaining early menarche and late menopause Early child bearing and breast feeding reduces the chances 7)It is more common in obese individuals. Breast cancer risk is qualified as relative risk (RR). If RR is 2. 0 means, risk is twice the normal population. If RR is 0. 5 means, risk is 50% less than normal population. Risk is 3 -5 times more if 1 st degree relative is having breast cancer. 8)In males, occasionally gynaecomastia turns into carcinoma.
9)Benign breast diseases with atypia, hyperplasia and epitheliosis has got higher risk in a patient with family history. 10)Cowden’s syndrome—It is an autosomal dominant condition, with cutaneous facial lesion (100%), bilateral breast lesion (50%), GI polyps, brain, thyroid tumours. It is often associated with ataxia telangiectasia. 11)Oral contraceptive pills and hormone replacement therapy (HRT) for more than 5 years.
Presently carcinoma breast is considered as a systemic disease. Halsted concept of spread is sequential spread. Breast—axillary lymph node— systemic spread. Fischer concept is early to begin with itself, there is distant blood spread because of micro metastasis without nodal disease. Only tumour lesser than 1 cm size can be sequential. Spectrum concept is new one where disease spreads loco regionally as well as systemically which makes it to aim at both loco regional disease control as well as systemic disease control.
Pathology Breast carcinoma arising from lactiferous ducts is called as ductal carcinoma. Breast carcinoma arising from lobules is called as lobular carcinoma. It is 10% common. In-situ carcinoma is preinvasive carcinoma which has not breached the epithelial basement membrane. It may be - Ductal in situ carcinoma (Ductal Carcinoma In Situ, DCIS) or - Lobular in situ carcinoma (Lobular Carcinoma In Situ, LCIS). Invasive carcinoma can occur eventually.
Classifications I. Ductal carcinoma Lobular carcinoma. II. (a) In situ carcinoma DCIS (Ductal carcinoma in situ). LCIS (Lobular carcinoma in situ). (b) Invasive ductal carcinoma. Invasive lobular carcinoma. It is commonly multifocal and often bilateral.
III. Unilateral. Bilateral— 2 -5% common. IV. Unifocal. Multifocal—tumour tissues within the same quadrant at multiple foci. Multicentric—tumour tissues within the same breast but in different quadrant.
DCIS It is intraductal carcinoma (proliferation of malignant mammary ductal epithelial cells) without any invasion into the basement membrane. It is 5%-20% common. It can be— Solid. Comedo with necrosis is high grade with increased chances of microinvasion. Cribriform. Papillary. Micropapillary.
It is associated with high expression of C – erb 2 gene (80%). It can be high grade DCIS or low grade DCIS. It can be comedo DCIS (more malignant and more likely to be invasive later) or non-comedo DCIS (less malignant). Nipple discharge and often small swelling are main presentations.
Management of DCIS FNAC confirms the disease but will not differentiate from DCIS and invasive carcinoma Mammography, U/S breast, MRI breast Routine metastatic work up Breast conservative surgery with RT to breast and axillary dissection after SLNB Hormone therapy (tamoxifen) prevents both local recurrence and development of new primary breast carcinoma.
Total mastectomy is done in DCIS when – positive margin after wide local excision; two or more primary tumour; when radiation to breast is not possible; tumour/breast size ratio is not appro-priate for conservative surgery and DCIS in pregnancy. Skin sparing mastectomy (SSM) may be ideal in such occasions.
Risk of lymph node spread in DCIS is less than 4%. So axillary dissection is not necessary. Sentinel Lymph Node Biopsy and proceed is the preferred method.
Types 1. Scirrhous carcinoma: It is 60% common. It is hard, whitish, or whitish yellow, noncapsulated, irregular, with cartilaginous consistency. It contains malignant cells with fibrous stroma. 2. Medullary carcinoma: Also called as ‘encephaloid type’ because of its brain like consistency. It contains malignant cells with dispersed lymphocytes.
3. Inflammatory carcinoma/Lactating carcinoma/Mastitis carcinomatosis: Most malignant type of carcinoma breast. It is 2% common. It is common in lactating women or pregnancy. It mimics acute mastitis because of its short duration, pain, warmth and tenderness.
Clinically, it is a rapidly progressive tumour of short duration, often involving whole of breast tissue with occurrence of Peau d’ orange, often extending to the skin of chest wall also. It rapidly metastasises to chest wall, bone and lungs. It is always stage IV carcinoma (T 4 d). FNAC confirms the diagnosis—It contains undifferentiated cells.
Total count is normal. Treatment External radiotherapy and chemotherapy. It has got worst prognosis. Differential diagnosis Acute mastitis—Total count is increased.
4. Colloid carcinoma: it produces abundant mucin. 5. Paget’s disease of the nipple It is superficial manifestation of an intraductal carcinoma. The malignancy spreads within the duct up to the skin of the nipple and down into the substance of the breast. It mimics eczema of nipple and areola.
There is a hard nodule just underneath the areola, which later ulcerates and causes destruction of nipple. Histologically, it contains large, ovoid, clear paget’s cells with malignant features.
6. Tubular, papillary, cribriform are other types of duct carcinomas. 7. Atrophic scirrhous carcinoma: Seen in elderly females. It is a slow growing tumour which has got better prognosis. FNAC is diagnostic. Mastectomy or curative brachytherapy (using breast moulds) is the treatment of choice. It is curable.
8. Lobular carcinoma in situ Predominantly premenopausal. Need not be detected by mammography, as it does not provoke calcification. It is an incidental pathological entity. Multifocal and bilateral. Clinically, it do not form a lump. Does predispose to invasive cancer.
50% cancers can develop in the contralateral breast. Immunohistochemistry using e-cadherin antibody shows positive reaction in lobular carcinoma. It has poor prognosis due to bilateral, multifocal nature and difficulty in identifying it. 9. Disease of Reclus: It is a rare intracystic papilliferous carcinoma of breast presenting as a cystic swelling with bloody discharge from the nipple.
Grading of the Tumour It is based on Nuclear pleomorphism; Tubule formation; Mitotic rate. It can be – Well-differentiated--grade 1 Moderatelydifferentiated--grade 2 and Poorly differentiated--grade 3.
Clinical Features Most common site is upper outer quadrant (60%) because breast tissue is more in this quadrant. Cutaneous Manifestations of Carcinoma Breast Peau d’orange: Due to obstruction of dermal lymphatics, openings of the sebaceous glands and hair follicles get buried in the oedema giving rise to orange peel appearance. Dimpling of skin due to infiltration of ligament of Cooper.
Retraction of nipple due to infiltration of lactiferous duct. Ulceration, discharge from the nipple and areola. Skin ulceration and fungation. Cancer-en-cuirasse: Skin over the chest wall and breast is studded with cancer nodules appearing like an armour coat. Tethering to skin.
Spread into the Deeper Plane Into pectoralis major muscle (is confirmed by observing the restricted mobility of the swelling while contracting the PM muscle). Into latissimus dorsi muscle (extending the shoulder against resistance). Into serratus anterior (by pushing the wall with hands without flexing the elbow). Into the chest wall (breast will not fall forward when leaning forward, and while raising the arm above the shoulder, breast will not move upwards as it is fixed to the chest wall).
Lymphatic Spread Occurs through – subareolar Sappey’s lymphatic plexus (presently its significance is discounted). – cutaneous lymphatics. – intramammary lymphatics. Lymphatic drainage of the breast is predominantly through axillary (75%) and internal mammary lymph nodes.
Spread to these lymph nodes occur by lymphatic permeation. Interpectoral, lies between pectoralis major and minor muscle (Rotter’s nodes). Groups 1 st and 2 nd are commonly involved. Groups 3 rd and 4 th are rarely involved. Finally Group 5 th is involved. From axillary lymph nodes spread occurs to supraclavicular lymph nodes by lymphatic embolisation.
Through dermal lymphatics, it may spread to opposite breast or to opposite axillary lymph nodes. Spread may occur into internal mammary lymph nodes of same side and then to mediastinal lymph nodes. Contralateral internal mammary lymph nodes can also get involved by retrograde spread. Fixed enlarged axillary nodes can cause lymphoedema due to lymphatic block; venous thrombosis and venous oedema due to venous block; and severe excruciating pain along the distribution of nerves.
Tumour infiltration of the cords of brachial plexus. Often it is difficult to differentiate between lymph node in pectoral region and tumour invasion of axillary tail. Mobility will be independent if it is a lymph node, but if it is an axillary tail tumour, it is along with the primary tumour in the breast.
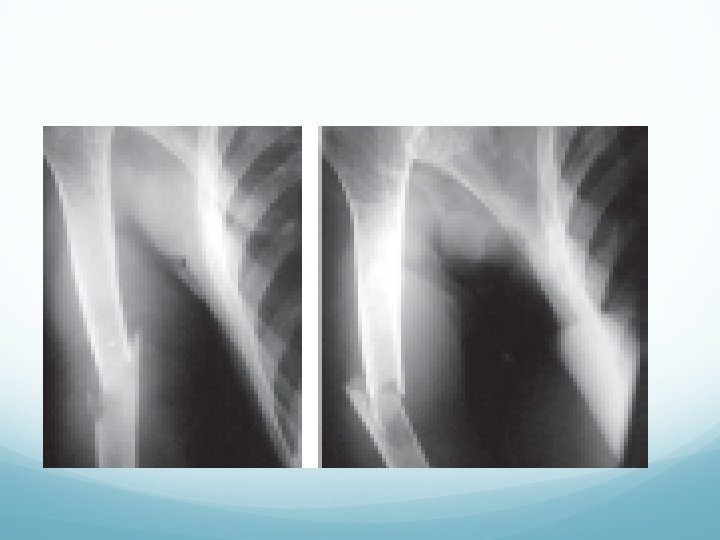
Haematogenous Spread Bone (Commonest) (70%)—Lumbar vertebrae, femur, ends of long bones, thoracic vertebrae, ribs, skull, in order. They are osteolytic lesion often with pathological fracture. Present with painful, tender, hard, non-mobile swelling, with disability. 70% of secondaries in bone in a women is due to carcinoma breast. Spine secondaries can cause paraplegia.
Liver—either through blood, occasionally through transcoelomic spread. Lung—causes malignant pleural effusion and cannon ball secondaries. Brain—causes increased intracranial pressure, coning. Adrenals and ovaries.
Common sites of distant spread in carcinoma breast Bones— 70% - (lumbar vertebrae, pelvic bones, long bones) Lungs and pleura— 20 -30% Soft tissues— 5 -15% Liver— 10 -12% Brain— 2 -5% Adrenals— 2 -5%
Transcoelomic spread Through mediastinal lymph nodes, it may spread into peritoneal cavity causing secondaries in liver, peritoneum, ovary (krukenberg secondaries) Occurs in menstruating age groups. During ovulation, cells get attached over the ovarian capsule Present concept of krukenberg tumour is haematogenous and lymphatic modes of spread. Older concept of transcoelomic spread is no longer well-accepted.
Breast self-examination (BSE) Plays a major role in early detection and intervention of breast carcinoma. This underlines the importance of advocating selfexamination of the breast.