CLASS 6 18082015 2 INTRAMAMMARY MASTITIS BREAST ABSCESS

CLASS 6 18/08/2015
 A. Lactational abscess of the breast: Commonly seen in")
2. INTRAMAMMARY MASTITIS (BREAST ABSCESS) A. Lactational abscess of the breast: Commonly seen in lactating women Precipitating factors Cracked nipple Retracted nipple Improper cleaning of the nipple

Inadequate milk sucking by baby or milk expression causing stasis Infection from the mouth of the baby Haematoma getting infected Mode of infection: Bacteria (Staph. aureus—commonest) enters the breast during sucking through the cracked nipple. Occasionally haematogenous spread.

Gram negative and other bacterial infections can supervene later. Staphylococcus aureus causes clotting of milk in the blocked duct and multiply. Duct initially gets blocked by epithelial debris or by retracted nipple. Initially it begins in one quadrant but later involves entire breast.

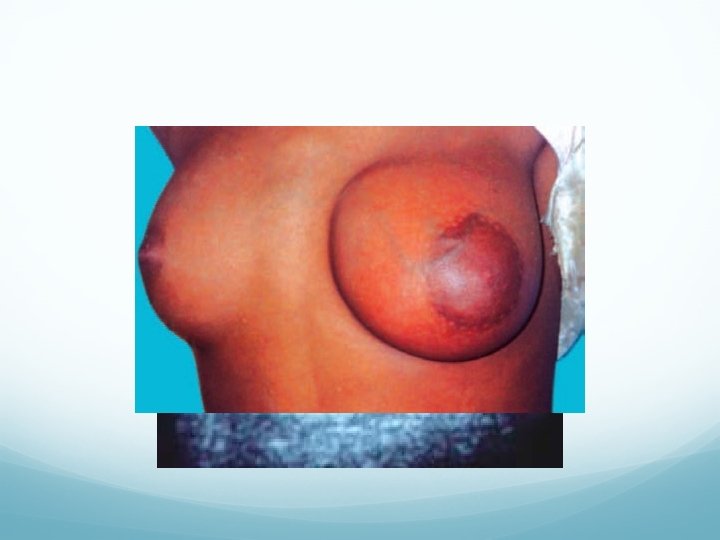
Clinical features: Continuous throbbing pain in the breast and fever. Diffuse redness, tenderness and brawny induration in the breast. Purulent discharge from the nipple. Entire breast may get involved eventually.
 from")
It is difficult to differentiate initial stage of mastitis (stage of cellulitis) from stage of breast abscess formation. When it is treated by antibiotics without incision and drainage eventually it may get organised to form a nontender, hard breast lump with sterile pus inside – stage of antibioma formation. Differential diagnosis: Inflammatory carcinoma of breast.


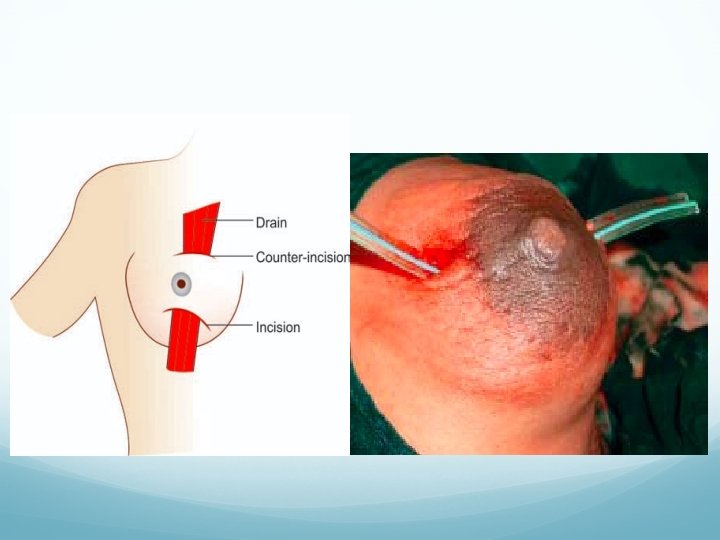
Treatment: Antibiotics—Cephalosporins, flucloxacillin and amoxicillin. Repeated US guided aspirations can be tried which avoids surgery and scar. Drainage under general anaesthesia, a counter incision may be needed. It is not advisable to wait till the formation of abscess.

Indications for drainage in mastitis/breast abscess– Mastitis not resolving with antibiotics in 48 hours Persistent fever and progression of mastitis Brawny induration Do not wait for abscess to form (fluctuation to develop)

Complications: Antibioma formation. Sinus formation, skin necrosis, fistula formation. Recurrent infection, bacteraemia, septicaemia. Suppression of lactation is often required by giving Bromocryptine 2. 5 mg BD for 2 weeks.

B. Non-lactational abscess of the breast: It commonly occurs in duct ectasia and periareolar infections. Common organisms are bacteroides, anaerobic streptococci, enterococci and gram negative organisms. It is commonly recurrent with tender swelling under the areola. Treatment: Antibiotics. Repeated aspirations. Drainage and later cone excision of the duct is done.

3. RETROMAMMARY MASTITIS It is due to tuberculosis of the intercostal lymph nodes or ribs beneath or suppuration of the intercostal lymph nodes. Breast is normal. Causes Tuberculosis of intercostal lymph nodes Tuberculosis of ribs beneath Suppuration of intercostal lymph nodes Empyema necessitans Infected haematoma.

Investigations: Chest X-ray. FNAC. ESR. Peripheral smear. U/S of breast and chest wall. Often CT scan chest may be needed.

Treatment: Cause has to be treated. Drainage through submammary/retromammary incision. Mastitis of infancy (witch’s milk) is due to maternal hormone in infant blood. It usually subsides but may cause suppuration. Mastitis of infancy affects both sexes equally.

Mastitis of puberty is common in boys, is invariably unilateral with tender, swollen and inflamed breast. Mumps --unilateral and can occur in both sexes. Bacterial mastitis is seen in adult women, commonly lactating and is due to staphylococci infection. Subareolar mastitis is due to infection of gland of Montgomery or due to areolar furuncle.

ANTIBIOMA If intramammary mastitis is not drained but only treated by antibiotics, pus localises and becomes sterile (flaques) with a thick fibrous tissue cover and it is called as antibioma. Clinical features Previous history of mastitis treated with antibiotics. Swelling which is painless, smooth, nontender, hard, fixed to breast tissue without involving the pectorals and chest wall.
. Investigations FNAC Mammography U/S breast Treatment Excision")
Differential diagnosis Carcinoma breast (scirrhous carcinoma breast). Investigations FNAC Mammography U/S breast Treatment Excision (submammary incision). Later antibiotics are given. It should be sent for histology.
 OF THE BREAST Includes variety of benign")
ABERRATION OF NORMAL DEVELOPMENT AND INVOLUTION (ANDI) OF THE BREAST Includes variety of benign breast disorders occurring at different periods of reproductive periods. Early, matured and involution phase. First coined at Cardiff breast clinic in 1987 by Le Hughes. Often mammography and FNAC/core cut biopsy should be done to rule out malignancy. ANDI includes different aberrations and diseases.
: Normal lobule formation—fibroadenoma as aberration and")
In early reproductive age group (15 -25 years): Normal lobule formation—fibroadenoma as aberration and giant fibroadenoma as diseased status. Normal stroma--juvenile hypertrophy as aberration and multiple fibroadenoma as diseased status.
: Normal cyclical hormonal effects on glands")
In mature reproductive age group (25 -40 years): Normal cyclical hormonal effects on glands and stroma get exaggerated by aberration causing generalized enlargement. Its diseased status is cyclical mastalgia with nodularity also called as fibrocystadenosis.
: Lobular involution – Macrocyst & Sclerosing adenosis is")
Involution age group (40 -55 years): Lobular involution – Macrocyst & Sclerosing adenosis is type of aberration. Ductal involution-- ductal dilatation and nipple discharge as aberration. Later disease status develops with periductal mastitis, bacterial infection, non-lactational breast abscess and mammary duct fistula. Periductal fibrosis may cause partial nipple retraction. Epithelial changes leads into epithelial hyperplasia and atypia.

FIBROADENOMA Benign encapsulated tumour occurring commonly in young females of 15 -25 years age group. Hyperplasia of a single lobule of the breast (classified under ANDI). Most common benign tumour of the breast. It is aberration in normal development of a lobule.
—Common in")
TYPES Gross: 1. Soft. 2. Hard. 3. Giant (> 5 cm in size)—Common in Africa.
. Stroma with distorted duct. 2. Pericanalicular—mainly")
Microscopy: 1. Intracanalicular—mainly fibrous tissue (small and hard). Stroma with distorted duct. 2. Pericanalicular—mainly cellular (large and soft). Stroma with normal duct.


Clinical features Painless swelling in one of the quadrants. Smooth, firm, nontender, well localized and moves freely within the breast tissue. Mouse in the breast Axillary lymph nodes are not enlarged.
. FNAC. Ultrasound (to confirm solid nature). Treatment Excision")
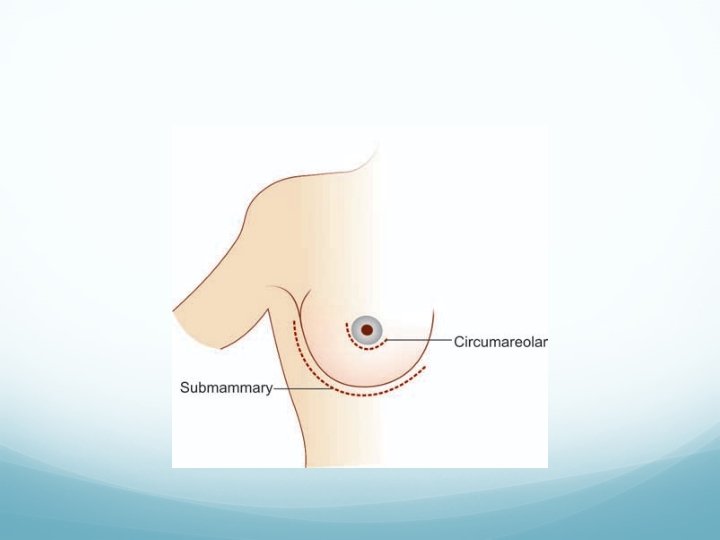
Investigations Mammography (well-localised smooth regular shadow). FNAC. Ultrasound (to confirm solid nature). Treatment Excision through a circumareolar incision (Webster’s) or Submammary incision (Galliard Thomas incision) is done.

FIBROCYSTADENOSIS FIBROCYSTIC DISEASE OF THE BREAST/MAMMARY DYSPLASIA Due to aberration of normal development and involution (ANDI). It is presently called as cyclical mastalgia with nodularity. It is an estrogen dependent condition.
 Hyperplasia (Epitheliosis)—in ducts and acini")
Microscopic changes Stromal fibrosis Microcyst formation Glandular proliferation (Adenosis) Hyperplasia (Epitheliosis)—in ducts and acini Papillomatosis—within the ducts, often with apocrine metaplasia

One of the cysts may get enlarged to become a clinically palpable, well-localised swelling—BLUEDOME CYST OF BLOODGOOD. It is fluctuant, transilluminant, nontender, often tensely cystic swelling (macrocyst) with thin bluish capsule. It should be aspirated initially. Surgical excision is done If it persists or recurs even after two aspirations; If it is blood stained; If there is residual lump after aspiration.

When diffuse small, multiple cysts are the main component, it is called as SCHIMMELBUSCH’S disease. It is the commonest breast disease. It is common in upper and outer quadrant.

Clinical Features Presentation is during menstruating age group as a bilateral, painful, diffuse, granular, tender, swelling which is better felt with palpating fingers. Pain and tenderness are more just prior to menstruation (cyclical mastalgia). It subsides during pregnancy, lactation and after menopause. Discharge from the nipple will be serous or occasionally greenish. Shotty enlargement of axillary lymph nodes, not fixed.
. Ultrasound. Mammography.")
Investigations FNAC (Epitheliosis, when florid is undoubtedly premalignant). Ultrasound. Mammography.

Treatment I. Conservative line of management is preferred. 1. Reassurance. 2. Oil of evening primrose (capsules): contains gamolenic acid which reverses the saturated fatty acids to unsaturated fatty acids. 320 -500 mg/day for 4 months. 3. Gamolenic acid— 120 mg. 4. Bromocriptine— 1. 25 -2. 5 mg BD for 3 months. 5. Vit E and B 6. 6. LHRH agonist.

7. Danazol— 200 mg BD for 3 months. 8. NSAIDs. 9. Tamoxifen—antioestrogen. 10. Diuretics II. Surgery: Subcutaneous mastectomy with prosthesis placement-- only in severe, persistent disease.

Excision of the cyst or localised excision of the diseased tissue. Indications for surgery 1. Intractable pain 2. Florid epitheliosis—on FNAC 3. Bloodgood cyst

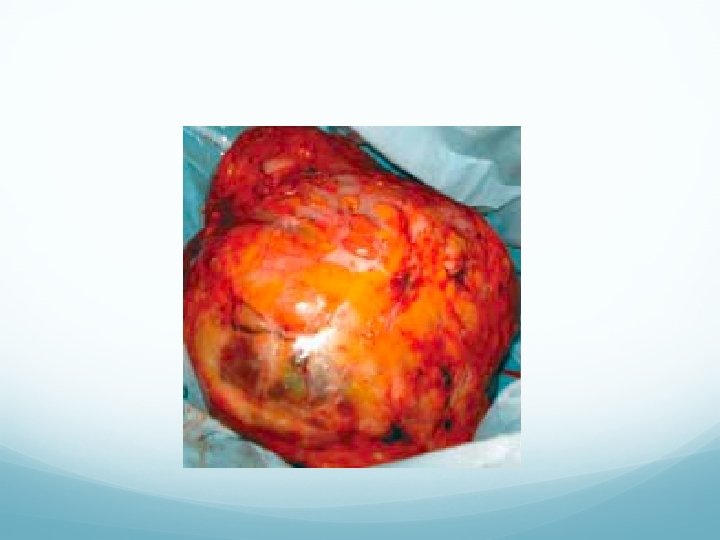
PHYLLOIDES TUMOUR CYSTOSARCOMA PHYLLOIDES/ SEROCYSTIC DISEASE OF BRODIE They are not simply giant fibroadenoma. They show a wide spectrum of activity, varying from benign condition (85%) to a locally aggressive and sometimes metastatic tumour (15%). Depending on mitotic index and degree of pleomorphism they are graded as low grade to high grade tumours. When malignant (sarcoma) spreads to lungs or bone.

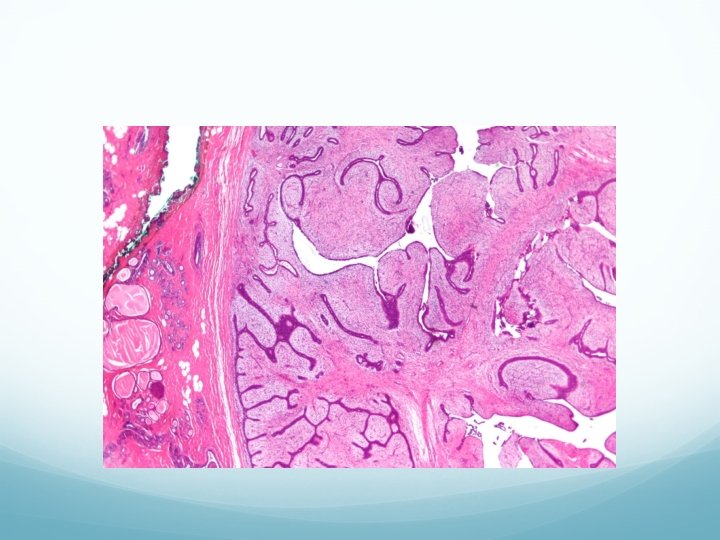
Gross: Large capsulated area with cystic spaces and cut surface shows soft, brownish, cystic areas. Microscopy: It contains cystic spaces with leaf like projections, hence the name (phylloides—greek—leaf-like). Cells show hypercellularity and pleomorphism. It may be a variant of intracanalicular fibroadenoma of breast (giant type).
. It is usually unilateral, Grows rapidly to")
Clinical features Premenopausal women (30 -50 yrs). It is usually unilateral, Grows rapidly to attain a large size with bosselated surface. Swelling is smooth, nontender, soft, fluctuant with necrosis of skin over the summit due to pressure. Skin over the breast is stretched, red and with dilated veins over it.

Tumor is warmer, not fixed to skin or deeper muscles or chest wall. Nipple retraction is absent. Lymph nodes are usually not involved. Tumor grows rapidly; undergoes necrosis at various places; causes cystic areas. Recurrence is common.


Investigations U/S. FNAC. Mammography. Chest X-ray CT chest in malignancy to see secondaries. Treatment Excision or subcutaneous mastectomy is done. If malignant (sarcoma), total mastectomy is indicated.
- Slides: 47