City and Hackney Clinical Commissioning Forum Thursday 2

















")


 G&A")



 Develop care plans")





 nursing posts ceasing with effect from")









 in")



- Slides: 45
City and Hackney Clinical Commissioning Forum Thursday 2 nd February 2017 St Joseph’s Hospice
Agenda Items Led by 1. Welcome Clare Highton 2. Westminster Drug Project Information Sarah Metcalf, Marie Tiquet 3. Community Minor Surgery Service Information Deborah Colvin, Mikael Prevost 4. Unplanned - New Model Consultation May Cahill 5. Adult Community Nursing Information Tracey Fletcher 6. RSM Due Diligence Exercise Results Information Sunil Thakker Members’ Forum 1. 2. Lay Member Extension - Vote Constitution Changes - Vote Matthew Knell The next Clinical Commissioning Forum will be held on Thursday 2 nd March 2017, 1. 00 pm in the 1 st Floor Education Centre, St Joseph’s Hospice, Mare Street, Hackney
Hackney Recovery Service Integrated Substance Misuse Service
• Each provider brings expertise and quality to the ISMS partnership • Two Hackney based incumbent providers Counselling
Treatment Interventions WDP • • • • • Screening and Assessment Case Management Treatment Groups Psychosocial Interventions including Keyworking Assertive Outreach High Risk Client Management Stimulant Users Club Drugs NPS Young People/Transitional Older Adults Women Only Services SPOC Dual Diagnosis Arrest Referral Prison Link Court Liaison/ATR/DRR Criminal Justice Interventions including IOM Recovery Interventions St Mungo’s Clinical Interventions CNWL • • • Prescribing/Medically Assisted Recovery Complex Case/Risk Management Pharmacological Interventions Services for Hospital Patients at Homerton Hospital Community Detoxification Primary Care Training GP Shared Care Health Assessment & Checks GUM Clinic Satellites Sexual Health Support Services Blood Borne Virus Service • • • • Abstinence Based Courses Peer Led Services Health and Wellbeing Gym Access Counselling Family Carer/Parent Network Parenting Programme Lifeskills Housing/Welfare Advice Time Bank Vouchers Peer Support Training Service User Group Training Mutual Aid Recovery Check ups Recovery College
Current Provision 102 -110 Mare Street, E 8 3 SG E 9 7 QL • Assessment • Drop In & Open Access • Needle Exchange • Access to prescribing • Community detox • BBV & Health interventions • Group work • Keyworking • Housing & benefit support Westgate Street • Group work • Keyworking • Families & Carers • Counselling • Services for Women • BBV & Health interventions • Re-integration activities • Education, training & employment • Housing & benefit support • Abstinence based services Contact details: Phone number: 0300 3032611 24/7 Service User Freephone: 0808 1688669 Email: hackney@wdp. org. uk
Priority Development Areas • PHE Alcohol Priority Partnership and increasing alcohol successful completions • New self referral clinics • Dedicated slots for GP and Mental health referrals • Development of Dual Diagnosis support and interventions • Implementation of Phased Treatment • Development of Reducing Medications group, Pre-Tox group, Overdose management and Induction groups • Targeting NPS and Chem sex users and developing needle exchange packs • Outreach in partnership with Young Hackney, Multiple Needs Service and community Safety teams • Review of Treatment Pathways and increasing reintegration involvement from initial assessment • Hackney Recovery Service Website
End/Notes
ADVERT The CCG membership and engagement team have recently launched a CCG member’s twitter account with the aim of delivering quick updates and reminders to our members.
Community Minor surgery The same 3 surgeries as before working together: Well Street Surgery, Lawson Practice, Nightingale Practice. The same service as before, same referral form (word version on the CCG website - http: //www. cityandhackneyccg. nhs. uk/gp/pathways/)
Services provided No changes compared to last year regarding excision/cautery and injections For the cryotherapy, it is important to know that we can use it for Actinic Keratosis…. (Routine WARTS are not part of this service – Practices should treat under additional service as part of GMS. If your practice has opted out of the additional service please contact commissioners at the CCG. ) Specific areas: Nightingale: vasectomy, Lawson: Meibomian cysts within the eyelid, Eyelid skin tag, Vulval lumps and bumps. What we do not do: Treat lesion which do not fit the POLCV criteria- please make sure that they do fit the criteria to avoid difficult discussion with the patient when they are in clinic, Surgery on children, Hand surgery: removal of cyst or ganglion on fingers, Lesion more than 5 cm, Between 4 and 5 cm it will depends on where the lesion is.
POLCV The lesion is unavoidably and significantly traumatised on a regular basis AND This results in significant infections such that the patient requires 2 or more courses of oral or intravenous antibiotics per year OR The lesion is obstructing an orifice OR impairing field vision OR The lesion significantly impacts on function e. g. restricts joint movement by >20 degrees. Keloid Scars: WELC CCGs will not fund procedures to re-fashion keloid scars for cosmetic purposes. Symptomatic keloid scars may be treated if the scar: interferes with function OR causes pain or itchiness which is persistent and unrelieved by standard medication for over one year.
Request from provider to help with better care For all lesions, please include a clear description of appearance, site and measurement in your referral letter. This is very important be able to accept the referral and give the best service to the patient. Please use the form provided on the website rather than handwritten form, Please let us know for example if the patient: is immunosuppressed ( HIV. . . ) If there is a possibility of capacity issue. . Pyogenic Granuloma do grow quickly, please write clearly on the letter this is a possible one and we will aim to see the patient quickly.
Outcome of minor surgery Outcomes are good in terms of post surgical complication- if the patient respects the post operative advice (each patient is given a post op info leaflet). Infection are rare: 2 that I am aware in the Nightingale site out of >159 surgeries this year- please let us know if you see our patients with an infection post surgery. Discharge typically after the first appointment and letter is send to referring GP.
End/Notes
ADVERT
UNPLANNED CARE UPDATE TO CCF FEBRUARY 2017
RING FENCE • Our PBR spend (emergency admissions and A&E attendances at all providers) and services that are about good community care and keeping people out of hospital (FHV, ACERs, Duty doc, District Nurses) gone into a ring fence budget • Budget to be managed collectively by providers and commissioners • Worth in total about 110 m – half/half split on PBR and other • Focusing just on adults – ie over 19 s and excludes maternity
Living within the ring fence Block contracts If PBR increases puts other services at risk as the ring fence needs to remain in balance Unplanned care recommend what to do to rebalance PBR Emergency admiss ions DD FHV Acers Community Nursin g CHUHSE etc A&E attendances
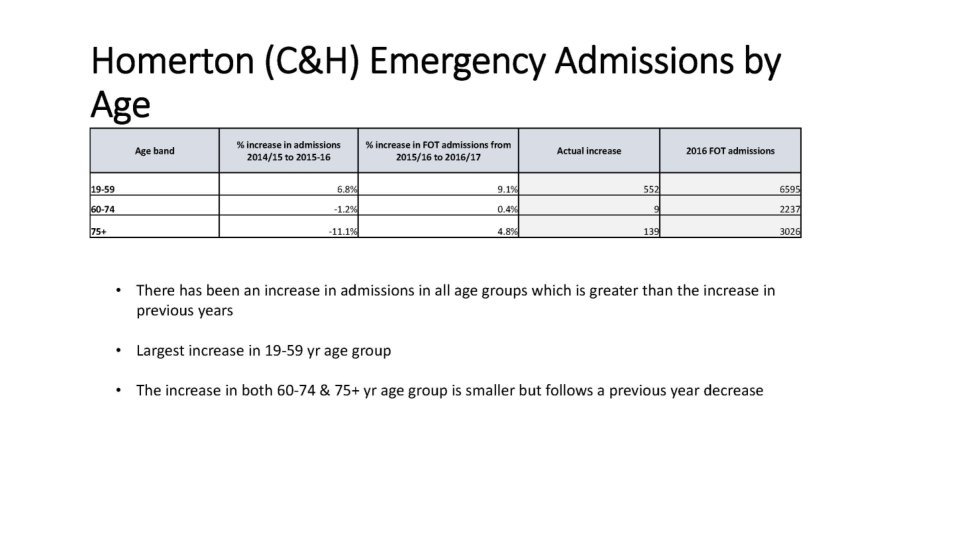
Key headlines • • • Spend on PBR emergency care is £ 0. 75 m more this year than last Emergency admission rate is up – particularly for 19 -59 s and over 75 s Emergency bed days are down -> more shorter stay admissions (up by 22%) Discharge delays are down Increases in admissions and length of stay at UCLH 4% increase in people attending A&E Message – we are holding it thanks to all the services we have in place But its volatile and increased PBR spend will put other services at risk in 18/19
Metric 4: Emergency Admission rate per 100, 000 registered population (benchmarked NEL CCGs) G&A Emergency Admissions (Adults Only) for City & Hackney CCG benchmarked against NEL CCG's 2015 -16 & 2016 -17 FOT at M 7, Rate Per 100, 000 Population 12 000 2015 -16 10 000 2016 -17 FOT NEL 1516 NEL 1617 CCG Name 8 000 6 000 4 000 NHS Camden CCG NHS Tower Hamlets CCG NHS Haringey CCG NHS Barnet CCG NHS Waltham Forest CCG NHS City and Hackney CCG NHS Islington CCG NHS Enfield CCG NHS Redbridge CCG NHS Newham CCG NHS Barking and Dagenham CCG - NHS Havering CCG 2 000 NHS Havering CCG NHS Barking and Dagenham CCG NHS Newham CCG NHS Redbridge CCG NHS Enfield CCG NHS Islington CCG NHS City and Hackney CCG NHS Waltham Forest CCG NHS Barnet CCG NHS Haringey CCG NHS Tower Hamlets CCG NHS Camden CCG 10, 776 10, 492 Percentage change -2. 63% 10, 384 8, 764 8, 783 8, 818 7, 950 7, 567 8, 313 7, 824 7, 700 7, 333 6, 825 9, 953 8, 994 8, 400 8, 391 8, 346 8, 067 7, 772 7, 723 7, 421 7, 351 7, 098 -4. 15% 2. 63% -4. 36% -4. 84% 4. 98% 6. 61% -6. 50% -1. 29% -3. 63% 0. 24% 4. 00% 2015 -16 2016 -17 FOT • C&H FOT admission rate has increased by 6. 61% from 2015/16 to FOT 2016/17 • However C&H remains below the NEL average and neighbouring boroughs 21
WHAT’S OUR PLAN
Building block 1 LAS alternative to A&E More work to do to define interface with practices Urgent response for GPs Pulling people out of hospital – discharge from wards and A&E IIT & Paradoc
Questions for CCF • Does this make sense • What needs to improve • IIT to link with practices to sort out package to stop someone being admitted? • More consultant advice when you do a home visit or is that what IIT should do? • More communication with the practice/DD – what and how? ?
Building block 2 • Practice FHV • Monthly at risk (NELIE) Develop care plans Discuss complex cases via MDT To deliver joined up care need team, linking to practices (“quadrant”) made up of • Community Matron • District Nursing • Access to vol sector services • Geriatrician/consultant advice • IIT + access to ACERs, DNS, HF etc • CPN/Mental health • Social Work
Questions for CCF • To help you what does quadrant team need to do more of/differently • What skills and functions do you need in the quadrant team • What were good things about OH need to keep • • Care coordinator to sort out complex care packages across teams? Teams attending practice MDTs – everyone or just some individuals – who? ? 1 lead GP for complex patients per practice ? Quadrant MDTs • To manage unwell patients at home rather than admit them to hospital • what support do you need • If the scope of FHV extends to at risk and removes the “home” requirement • What else would be needed
HOMERTON PERSPECTIVE • 2 Community Nursing pilots • Tracey as Chair of the Board
End/Notes
ADVERT Orthopaedic Masterclasses March 2017 Book your space via CCG Intranet Managing Shoulder Pain in Primary Care Wednesday 1 March 2017 7 pm – 8. 30 pm (supper from 6. 30 pm) Homerton Education Centre Speakers Mr Toby Baring - Consultant Orthopaedic Surgeon Mr David Boardman - Shoulder Specialist Spinal Assessment and Management in Primary Care Wednesday 8 March 2017 7 pm – 8. 30 pm (supper from 6. 30 pm) Homerton Education Centre Speakers Elizabeth Slee and the ESP Team The Management of Knee Arthritis in Primary Care Wednesday 15 March 2017 7 pm – 8. 30 pm (supper from 6. 30 pm) Homerton Education Centre Speaker Mr Deepu Sethi - Consultant Knee Surgeon
Adult Community Nursing Tracey Fletcher Homerton University Hospital Chief Officer Verbal Update
Adult Community Nursing Impact Hackney (non recurrent funding) nursing posts ceasing with effect from 31. 03. 17 o 4. 00 wte band 7 matron o 4. 00 wte band 6 senior staff nurse o 10. 00 wte band 5 staff nurse Future Referrals There will be no change in the current practice, the referral criteria will remain the same, as will the need for the service to meet the required response times. In addition, patients will continue to be allocated a 2 hour timeslot for their appointment. Consequences Each nurse will, however, experience a rise in their daily caseload which will impact on the delivery of holistic care due to the reduced time per patient per visit. The service over the next month will also be reviewing the initiatives implemented as a result of the additional funding - these include the Clinical Triage Team and Matron weekend working. The attendance at Quadrant and monthly GP meetings will remain a priority but will need to be balanced carefully against patient care need. Any decision not to attend a key meeting will only be made after review by a senior member of staff and a full explanation will be provided to the relevant meeting chair. Incorporating hospital and community health services, teaching and research
Adult Community Nursing Mitigation Mobile working is now fully operational in clusters 2 and 3 and funding has been received to roll this out into clusters 1 and 4. The onset of fully electronic documentation at the point of care will therefore reduce administrative time which can then be transferred into increased clinical care hours. Continual review of the caseload for each cluster will be undertaken to ensure that each patient continues to receive appropriate community nursing input. Initiatives such as working with the Community Diabetes Nurse Specialists to promote “self care” for patients who are insulin dependant diabetics will continue in this regard as will the joint working with IIT. The senior nursing team will review daily staffing levels in the context of care delivery and also quality of care and action will be taken immediately if this is compromised. The Trust will formally review the position in June to ensure there are no systematic clinical risks occurring as a result of the reduction in posts. Should this be evident intervention and escalation to the CCG will take place via appropriate channels. With the development of the new quadrant model, some additional Matron posts may be available. If so this will mitigate the reduction in nursing posts and have the potential to contribute to continuing the weekend Matron working which has received very positive feedback. Incorporating hospital and community health services, teaching and research
End/Notes
RSM Due Diligence Exercise Results Sunil Thakker CCG Joint Chief Financial Officer Verbal Update
End/Notes
ADVERT Recruiting now! Quality and Adult Safeguarding GP Clinical Lead JD and how to apply on the CCG Intranet
Request for approval of changes to the CCG Constitution and extension of Governing Body Member Presentation to the Thursday 2 February 2017 Members Forum FOR DECISION
Three decisions • • We are seeking Members Forum approval of the latest changes to the CCG’s Constitution to allow us to take on the commissioning of primary care, delegated from NHS England the updates to the document clarifying the arrangements for how we’ll operate in an integrated commissioning environment; In addition, we are requesting Members Forum approval for a six month extension to our Lay Member for Governance term of office.
Changes to the CCG’s Constitution • A new version of the CCG’s Constitution, with changes marked up in track changes is available at goo. gl/Xk. XR 9 U; • The changes focus on: Inclusion of NHS England requested text to allow the CCG to receive delegated responsibility for the commissioning of primary care. These changes are mandatory for NHS England to agree the delegation agreement with us: 1. • These changes are included in sections 7. 4 to 7. 6 on pages 21 to 24; • Changes to the Scheme of Delegation outlining the authority held by the Local GP Contracts Committee are covered on page 68; Changes to better reflect the environment in which we will be working under the integrated commissioning arrangements with the London Borough of Hackney and City of London Corporation: 2. • These changes are indicated in track changes and explanatory comments through the main Constitution and Scheme of Delegation. Minor tweaks to streamline processes, for instance: 3. • Moving Terms of Reference from the Constitution into stand alone documents. This allows us to hold one true source of information and for Terms of Reference to only be updated in one document; • To widen the potential membership of Committees of the Governing Body, which had been too narrow historically and excluded, for instance, Health. Watch representatives or patient representatives from being members of our Committees. • To remove references to frequency and sources of reporting information to allow them to change as needed and better reflect reality. • All changes have been produced with and consulted on with our solicitors and explanatory comments are included in the linked document; • None of the changes to the Constitution affect the role or powers of the Members Forum, which retains the ability to reverse CCG decisions (except when regarding the commissioning of primary care); • None of the changes to the Constitution affect the ability of the Members Forum to call a vote of no confidence in the Governing Body.
Extension to our Lay Member for Governance terms of office • • We are seeking Members Forum agreement to a six month extension to the term of office for our Lay Member for Governance, Mariette Davis to start from 1 April 2017 until 30 September 2017; Mariette Davis has occupied the role since 01/04/2013. She took up a second two year term on 01/04/2015 and her final term is due to end on 31/03/2017. We are seeking to extend this by six months to 30/09/2017 as the candidate who had accepted the Associate Lay Member for Governance position has had to pull out due to personal reasons; To ensure continuity while we re-advertise and appoint to the Associate Lay Member for Governance, as well as provide support and advice in the transition to appointing a new Lay Member for Governance, we recommend that Mariette Davis is retained for a six month period.
Mariette Davis Mariette is a Fellow of the Institute of Chartered Accountants (ICA) in England Wales and has thirty six years of executive experience. She has held senior positions in a professional accountancy firm and also in the financial services industry. Mariette was a Partner in Grant Thornton, a Director of Strategy in NM Rothschild & Sons Asset Management and Finance Director of Legal and General Ventures. She has worked in a non-executive capacity for the NHS since April 2010, including the position of Audit Chair of Tower Hamlets PCT and City and Hackney PCT. Currently, in addition to roles as Lay Member for Governance for City and Hackney CCG and Tower Hamlets CCGs, Mariette operates as a consultant, providing services to the private equity sector. Member of the CCG Governing Body, 1 April 2013 – current Member of the Finance and Performance Committee, 1 April 2013 – current Chair of the Audit Committee, 1 April 2013 – current Chair of the Remuneration Committee, 1 April 2013 – current Mariette has declared interests as Lay Member for Governance for Tower Hamlets CCG and as an Advisor for Acanthus Capital Limited.
Next steps • • If the Members Forum agrees the changes to the CCG Constitution, the changes will be presented to the CCG Governing Body on Friday 24 February 2017, along with further detailed information on the integrated commissioning arrangements for approval. The Constitution will then be submitted to NHS England for approval; If the Members Forum agrees to the extension of Mariette Davis term of office, the CCG Governing Body will be asked to ratify the agreement and a letter confirming the extension will be issued in early March 2017.
End/Notes
ADVERT T-spot test for latent TB – has your practice signed the service level agreement? Planned care have commissioned Oxford Immunotec to provide the T-Spot test for Latent TB – if your practice has not filled out a service level agreement, please email james. courtney 1@nhs. net