CHYLOTHORAX PSEUDOCHYLOTHO RAX Dr Kalpesh Patel Junior resident



 “Constant only in its variability” Originates from the")































 • Administered subcutaneously. • It decreases lymphatic flow and triglyceride absorption.")

")






, ligation")



,")





 is a rare condition, affecting mostly women of")











- Slides: 67
CHYLOTHORAX PSEUDOCHYLOTHO RAX Dr. Kalpesh Patel Junior resident TBHP
Chylothorax • Definition : – It is an accumulation of fluid, rich in triglyceride and characterized by the presence of chylomicrons in the pleural space. • Chylothorax is formed when the thoracic duct is disrupted and chyle enters the pleural space.
Thoracic duct • It is the largest lymphatic vessel of lymphatic system. • Function – transport of digestive fat to the venous system. • Also known as left lymphatic duct, alimentary duct, chyliferous duct and van Hoome’s canal. • In adult, thoracic duct is typically 38 -45 cm in length and average diameter of about 5 mm. • It drains into the systemic circulation at the brachiocephalic vein between the left subclavian and left internal jugular veins. • It collects most of the lymph in the body other than from right side which is drained by right lymphatic duct.
Anatomy • • • Davis (1915) “Constant only in its variability” Originates from the cisterna chyli. Enters thorax through aortic hiatus. Ascends along anterior surface of the vertebral bodies. Posterior to esophagus, between the aorta and the azygos vein. At T 5 -T 7 crosses to the left behind the aorta and ascends on left side of the esophagus
• Above clavicle, duct turns laterally. • It turns inferiorly to enter the venous system at the subclavian-internal jugular vein junction. • A bicuspid valve prevents entry of blood into the lymphatic system. • The right duct is small (2 cm in length). Drains lymph from right head, and chest. • Injury below T 5 to T 6 results in right chylothorax. • Injury above this level results in left chylothorax.
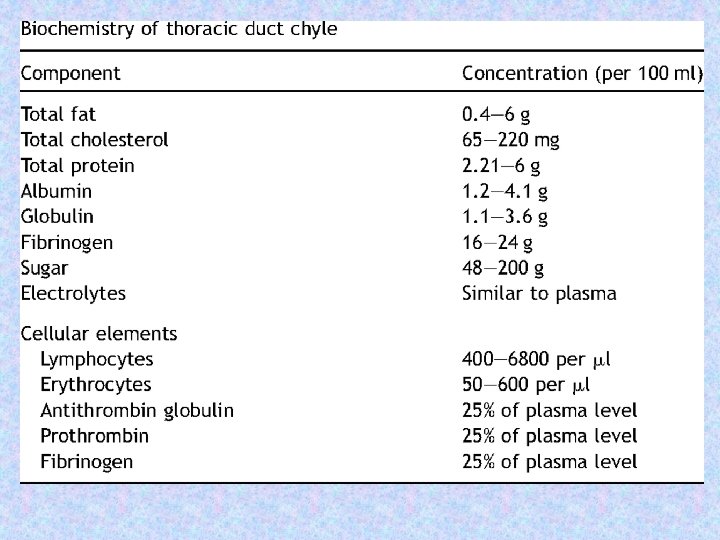
Chyle • The drainage from the thoracic duct is called chyle. • Chyle is a milky bodily fluid consisting of lymph and emulsified fats, or free fatty acids (FFAs). • It is formed in the small intestine during digestion of fatty foods, and taken up by lymph vessels specifically known as lacteals.
• Chyle separates into three layers upon standing: – a creamy uppermost layer containing chylomicrons, – a milky intermediate layer, and – a dependent layer containing cellular elements, most of which are small lymphocytes • Each day, between 1, 500 and 2, 500 m. L of chyle normally empties into the venous system. • Factors affecting chyle flow : – Ingestion of fat can increase the flow of lymph in the thoracic duct by 2 to 10 times the resting level. – Ingestion of liquid also increases the chyle flow. – Ingestion of protein or carbohydrates has little effect.
Etiology….
Modified De. Meester classification of chylothorax • Congenital – Atresia of thoracic duct – Birth trauma – Pleural thoracic duct fistula • Traumatic – Blunt – Penetrating – Surgical • Cervical – Excision of lymph nodes – Radical neck dissection • Thoracic – – – Ligation of patent ductus arteriosus Surgery for coarctation of aorta/aortic aneurysm Post-esophagectomy Surgery for mediastinal tumours Post-pneumonectomy • Abdominal – – – Post-sympathectomy Radical lymph node dissection Diagnostic procedures Lumbar arteriography Subclavian vein catheterisation • Neoplasms • Miscellaneous
Congenital Chylothorax • Congenital chylothorax is the leading cause of pleural effusion in the neonate. • Fluid initially clear but turns turbid with milk feeding. • Causes include birth trauma and congenital duct defect. • Associated with a variety of congenital syndromes like Turner's syndrome, Noonan's syndrome, or Down's syndrome. • Congenital chylothorax is also more common in infants who are hydropic or who have polyhydramnios. • Most neonatal chylothoraces are either right-sided or bilateral; only rarely are they left-sided.
Traumatic • Trauma is the leading cause of chylothorax. • Iatrogenic causes chiefly Thoracic surgery constitute the majority. • Oesophageal resection is perhaps the most common iatrogenic cause of chylothorax, with an incidence of 4%. • More likely in patients who undergo oesophageal resection by the transhiatal approach than the thoracic approach. • Other surgical procedures in the vicinity of the thoracic duct can inadvertently damage thoracic duct. Laceration of the thoracic duct during catheterisation of the subclavian vein can lead to a chyle leak. Extensive venous thrombosis complicating central venous catheterisation has resulted in bilateral chylothorax and chylopericardium.
• Non-iatrogenic causes are responsible for approximately 20% of cases of traumatic chylothorax. • Thoracic duct injury can occur following hyperextension of the cervical vertebral column and fracture-dislocation of the spine. • Chylothorax secondary to closed trauma is usually on the right side, and the site of rupture is most commonly in the region of the 9 th or 10 th thoracic vertebra. Such trauma includes falls from a height, motor vehicle accidents, compression injuries to the trunk, heavy blows to the back or stomach, and childbirth.
Neoplasms • Malignancy is one of the leading cause of chylothorax, 50% of chylothoraces in adults caused by tumors. • The most common malignancy to cause a chylothorax is a lymphoma and accounted for 75% of the chylothoraces due to malignancies. • Benign and malignant tumors may involve thoracic duct through lymphatic permeation, direct invasion or tumor embolus. • Most frequently found malignant tumors include lymphomas, lymphosarcomas, and primary lung carcinomas. • Benign lesions of the thoracic duct include: lymphangiomas, mediastinal hygromas, and pulmonary lymphangioleiomyomatosis.
Miscellaneous • Thrombosis of the superior vena cava or the subclavian vein – more common. • Hepatic cirrhosis - chylous pleural effusion results from the transdiaphragmatic passage of chylous ascitic fluid. Majority of hepatic chylothoraces are right sided. • Rarely associated with heart failure, nephrotic syndrome resulting in transudative chylous effusion.
• Other causes include – Gorham's syndrome, – Kaposi's sarcoma in patients with acquired immunodeficiency syndrome (AIDS), – filariasis, – giant lymph node hyperplasia (Castleman's disease), – lymphangiomatosis, – familial lymphedema, – lymphangitis of the thoracic duct, – obstruction of the superior vena cava secondary to Bechet's syndrome,
– tuberculosis, – sarcoidosis involving the intrathoracic lymph nodes, – aneurysms of the thoracic aorta that erode the duct, – abnormalities of the lymphatic vessels such as intestinal lymphangiectasis or reticular hyperplasia, – radiation-induced mediastinal fibrosis, and – hypothyroidism
Clinical manifestations • The symptoms, physical findings, and radiographic features of chylothorax are the same as those encountered in patients with comparably sized pleural effusions of any cause. • Half of all chylothoraces are right-sided, one-third is left-sided, and the remainder are bilateral. • Pleuritic chest pain and fever are rare because chyle is not proinflammatory. • With nontraumatic chylothorax, insidious onset of dyspnea on exertion is common.
• With traumatic chylothorax, there is usually a latent period of 2 to 10 days between the trauma and the clinical presentation of the pleural effusion. During this latent period, chyle may accumulate in the posterior mediastinum to form a chyloma—visible radiologically as a posterior mediastinal mass—which eventually ruptures into the pleural cavity, giving rise to a chylothorax. • Neonatal chylothorax may present with respiratory distress in the first few days of life. Fifty percent of the infants have symptoms within the first 24 hours, whereas 75% have symptoms by the end of the first week.
• Rarely, patients may experience a rapid accumulation of fluid in the pleural space, causing a tension chylothorax. This is of particular concern following a pneumonectomy. These patients experience a rapid hemodynamic and respiratory compromise, similar to classic tension pneumothorax. • The main threat to life with chylothorax is inanition from malnutrition if the chyle is drained externally. • The daily loss of 1. 5 to 2. 5 L of fluid rich in protein, fats, electrolytes, and lymphocytes will rapidly render patients malnourished and immunocompromised.
• Continued loss of proteins, immunoglobulins, and T-lymphocytes into the pleural space leads to immunosuppression. Furthermore, Blymphocyte-mediated immune functions are impaired by prolonged chyle drainage. • These factors predispose the patient to opportunistic infections. However, infection of a chylothorax itself is very uncommon because chyle is inherently bacteriostatic. • Electrolyte imbalance also occur.
Diagnosis • Distinctive white, odorless, milky appearance – suggestive of chylothorax • But requires differentiation from empyema and pseudochylothorax. • The milkiness with empyema is caused by the suspended white blood cells (WBCs), and debris and if such fluid is centrifuged, the supernatant is clear. • Chylous and chyliform pleural fluids remain opaque after centrifugation. • If cholesterol crystals are responsible for the turbidity, they may be easily demonstrated by examination of the pleural fluid sediment. • If the turbidity is due to high levels of cholesterol, the turbidity will clear when 1 to 2 m. L of ethyl ether is added to a test tube containing the fluid. • If the turbidity is due to chylomicrons or lecithin complexes, the turbidity does not clear.
Appearance…
• Not all chylous pleural effusions have the typical, milky appearance. With congenital chylothorax, the pleural fluid is initially serous and turns chylous only when milk feedings are started. • Chylothorax usually meets exudative criteria, but can be transudative. • Pleural fluid analysis for triglyceride content helps to confirm a diagnosis of chylothorax.
Triglyceride measurement • A level greater than 110 mg/d. L reflects a 99% chance that the fluid is chyle. • A level less than 50 mg/d. L reflects only a 5% chance that the fluid is chyle. • If the level is 50 -110 mg/d. L, use lipoprotein analysis to inspect the pleural fluid for chylomicrons or cholesterol crystals.
• If the pleural fluid triglyceride level is above 110 mg/d. L and Ratio of the pleural fluid to serum cholesterol is less than 1. 0, the diagnosis of chylothorax is established. • A ratio of pleural fluid cholesterol to triglyceride of less than 1 is also diagnostic. • Cholesterol ratio is used to exclude pseudochylothorax.
v Only other situation in which the pleural fluid triglyceride is above 110 mg/d. L is when intravenous fluid containing high levels of triglycerides leaks from a central vein into the pleural space. v Fasting may significantly reduce the triglyceride level in the pleural fluid and produce false-negative results having serous-appearing pleural fluid. To confirm the diagnosis, feed with high fat meal before sampling.
Chylomicrons If any doubt persist…. . • The demonstration of chylomicrons in the pleural fluid by lipoprotein analysis establishes the diagnosis of chylothorax.
Lipophilic Dye Ingestion • Ingestion of a fatty meal with a lipophilic dye, followed by a thoracocentesis 30 to 60 minutes later, to ascertain whether the pleural fluid has changed in color. • Most commonly used dye is Drug and Cosmetic Green No. 6, a coal-tar dye.
Imaging of thoracic duct • Lymphoscintigraphy : Technetium-99 m human serum albumin is injected into the dorsum of the foot or hand subsequently the thoracic duct is imaged in nuclear medicine. • Oral ingestion of iodine labelled BMIPP, the thoracic duct can be imaged approximately 80 minutes later.
Imaging studies • Chest roentgenography with lateral views as well as decubitus views may be helpful in determining the size and location of the chylothorax. • CT is useful when chylothorax is associated with trauma, or where an underlying tumour is suspected. Patients with chylothorax and no obvious trauma must undergo CT Chest and abdomen to look for lymphadenopathy, also useful in the diagnosis of lymphangioleiomyomatosis.
• MRI can confirm the high fat density of the pleural effusion and may support the diagnosis of chylothorax. • 3 D MRI with lymphoscintigraphy can provide additional anatomical and functional details of the lymphatic channels.
• N/B : examination of the pleura is unlikely to provide insight to the etiology of the chylothorax. • Hence, pleural biopsy or thoracoscopy is not usually indicated in the workup of patients with a chylothorax.
Treatment….
Treatment • It should be directed towards : 1. Maintaining nutrition and reducing the flow of chyle, 2. Relieving dyspnea by removing the chyle, and 3. Closure of the defect.
Maintaining Nutrition and Reducing the Volume of Chyle Circulation • Nil per oral or or a diet rich in low-fat, mediumchain triglycerides. • The patients nutritional status can be maintained with intravenous hyperailmentation. • It is preferred than medium chain triglycerides which are unpalatable and are recommended when one wishes to reduce the flow. • The flow of chyle is also decreased if the patient stays in bed because any lower extremity movement increases the flow of lymph.
Octreotide (somatostatin analogue) • Administered subcutaneously. • It decreases lymphatic flow and triglyceride absorption. • Mechanism of action unknown. Presumed lymphatic vessels may have somatostatin receptors and their stimulation could result in decreased lymphatic flow. • Side effects are related to suppressive actions of gastrointestinal motility and secretion and include loose stools, malabsorption, nausea, and flatulence. • Dose : in Adult 50 mg 8 hrly in children 0. 3 to 1 mcg/kg/hr
• Somatostatin : • Continuous i. v. infusion. • Usual starting dose is 3. 5 mcg/kg/hr can be increased upto 12 mcg/kg/hr. • Adverse effects includes diarrhea, hypoglycemia, and hypotension.
Relieving Dyspnea by Removing Chyle from the Pleural Cavity • Thoracentesis (short term only) • Tube thoracostomy (short term only) – To decompress the pleural space and to keep the lung expanded against the chest wall and mediastinum. – every attempt should be made to minimize the duration of tube drainage to avoid malnutrition or immunosuppression.
Pleuroperitoneal Shunt : • Optimal method to remove the chyle and alleviate the dyspnea. • Advantages : – Lymph is not removed from the body, and, therefore, the patient does not become malnourished or immunocompromised. – Can be inserted with local anesthesia as opposed to general anesthesia, which is required for thoracic duct ligation • When the chyle is shunted to the peritoneal cavity, it is absorbed without creating significant ascites.
• When a pleuroperitoneal shunt is implanted, the defect closes spontaneously in most cases and the shunt can be removed 30 to 90 days after its insertion. • Contraindicated if ascites is present, and is less likely to be successful if the chylothoraces result from central venous thrombosis. q Redirection of the chyle back into the systemic circulation has also been performed successfully via pleurovenous shunts
Surgical management • Indications for surgical intervention include the following: – Chyle leak greater than 1 L/d for 5 days or a persistent leak for more than 2 weeks despite conservative management – Nutritional or metabolic complications, including electrolyte depletion and immunosuppression – Loculated chylothorax, fibrin clots, or trapped lung – Postesophagectomy chylothorax (Patients with this carry a high mortality rate if treated conservatively. )
Percutaneous Transabdominal Thoracic Duct Blockage • Minimally invasive and relatively effective. • Developed by Cope and Kaiser • Pedal lymphography is initially performed to opacify large retroperitoneal lymph channels. Then a suitable duct (one that is more than 2 mm in diameter) is punctured transabdominally to allow catheterization and embolization of the thoracic duct under fluoroscopic guidance. • Embolization is performed using platinum microcoils or microparticles. • Glue has also been used singly or in combination with coils being more efficient to prevent recanalization.
Ligation of the Thoracic Duct through Thoracotomy • Definitive treatment for postoperative chylothorax. • Causes no ill effects (because of multiple anastomosis among various lymphatic channels and direct lymphatico-venous communication). • Lampson first demonstrated successful ligation in 1948. • Usually, the side of the chylothorax is ipsilateral to the original surgery, and reoperation can be performed through the original thoracotomy incision. • If the chylothorax is unilateral, the thoracotomy should be performed on the side of the fluid. • If the chylothorax is bilateral, a right thoracotomy should be performed because the duct is more readily approached from that side.
• Prerequisite : preoperative lymphangiogram should be obtained in every case to demostrate the site of leak or obstruction. • For identifying the thoracic duct intraoperatively Evans blue dye is injected in subcutaneous tissue of the leg, Within 5 minutes, the chyle will be stained blue. Dose 0. 7 to 0. 8 mg/kg, total dose not exceeding 25 mg. • Or place a tube in the duodenum and inject cream. • One should attempt to find the actual point of leakage from the duct and ligate the duct on both sides of the leak. • Parietal pleurectomy should be performed to obliterate the pleural space, if required. • If leak cannot be located the thoracic duct should be ligated. • Alternative approach by Mason et al. , who recommends ligation of thoracic duct just below the diaphragm through an intraabdominal approach.
Ligation of the Thoracic Duct through Thoracoscopy • With video-assisted thoracic surgery (VATS), ligation of the thoracic duct can be done with the videothoracoscope. • Thoracoscopy permits the entire pleural space to be visualized, as well as allowing direct suture of a lymphatic leak. • Wurnig et al. reported the successful use of VATS with ligation of the thoracic duct immediately above the diaphragm.
Pleurodesis • When the thoracic duct is unidentifiable, talc pleurodesis could be tried. • It has a success rate of 95% and negligible morbidity. • When the chylothorax is complicated, loculated, or the site of chyle leak cannot be established, pleural decortication and surgical pleurodesis may be indicated. • Fibrin glue has also been used to seal chyle leak by inducing pleurodesis.
Special considerations…
Nontraumatic Chylothorax • In general, the goals of management of nontraumatic chylothorax are the same as for traumatic chylothorax. • Establishment of cause is necessary. • The possibility of lymphoma should be considered in all patients with a nontraumatic chylothorax because it is the most common cause of nontraumatic chylothorax. • Mediastinal radiation adequately controlled the chylothorax for the remainder of the patient's life in 68% of those with lymphoma and in 50% of those with metastatic carcinoma. • If radiation therapy fails, embolization, pleurodesis, or pleuroperitoneal shunting should be considered.
• If the characteristics of the chyle are transudative, (low protein, low LDH), then most likely etiologies are cirrhosis, congestive heart failure, and the nephrotic syndrome. • The chylothorax associated with cirrhosis can be treated by a transjugular intrahepatic portosystemic shunt. • The chylothorax associated with thrombosis of the superior vena cava can resolve with the use of thrombolytic therapy and placement of a self expanding metallic stent.
• Chylothorax associated with sarcoidosis is likely to disappear if the patient is treated with corticosteroids. • If the cause of a nontraumatic chylothorax is unknown and, • If chest CT and lymphangiography are normal, the chylothorax can be assumed to be due to minor trauma, and spontaneous closure can be expected within weeks.
Fetal and Congenital Chylothorax • Chylothorax is the most common type of pleural effusion in infants. Chylothorax in infancy can be fatal. • If diagnosed in utero, maternal dietary restriction should be initiated. • Thoracentesis can be performed under ultrasound guidance to evacuate the chylothorax, as large effusions can cause pulmonary hypoplasia and respiratory distress at birth. • If the chylothorax reaccumulates, pleuro-amniotic shunting should be considered. • Also ultrasound-guided intrapleural administration of OK 432 or maternal blood has offered effective control of the chylothorax, presumably via creating a pleurodesis.
In neonates…. . • Initially, treat conservatively with repeated thoracenteses. • Total parenteral nutrition. • If the chylothorax recurs after the third pleural aspiration, a pleuroperitoneal shunt should be inserted. • Alternatively, octreotide can be administered. • Thoracic duct ligation is indicated if the pleuroperitoneal shunting fails. The advantage of the shunt over the thoracic duct ligation is that it is a much simpler procedure.
Gorham’s Syndrome • Gorham's syndrome is a rare disease that can occur at any age but is most often recognized in children or young adults. There is no sex predilection and no inheritance pattern. • The characteristic lesion of Gorham's syndrome is an intraosseous proliferation of vascular or lymphatic channels that leads to the disappearance of bones. • Patients with Gorham's syndrome have a high incidence of chylothorax
• All the patients with Gorham's syndrome and chylothorax had a rib, scapular, clavicular, or thoracic vertebral bony involvement • Patients with Gorham's syndrome and chylothorax should be treated with a pleuroperitoneal shunt or thoracic duct ligation
Pulmonary Lymphangiomyomatosis • Pulmonary lymphangioleiomyomatosis (LAM) is a rare condition, affecting mostly women of reproductive age, and is characterized by progressive dyspnea, recurrent pneumothoraces, and chylous effusions. • The reported incidence of chylothorax in patients with LAM ranges from 10% to 30%. It can occur in both the sporadic and the tuberous sclerosis complex –associated types of LAM—the former is associated with a higher incidence of chylothorax
• The chylothorax is thought to be the result of the combination of perilymphatic proliferation of smooth muscle leading to lymphatic obstruction and of infiltration of the lymph nodes in the mediastinum and retroperitoneal space by immature smooth muscle cells. • CT scan is usually diagnostic for LAM • The chylothorax associated with LAM should be managed as are chylothoraces secondary to other medical conditions. If the chylothorax is small and is asymptomatic, it need not be treated. If it is larger, it is probably best treated with thoracoscopic ligation of the thoracic duct or the implantation of a pleuroperitoneal shunt.
Prognosis of chylothorax • In the past, the mortality due to chylothorax was in excess of 50%. • Currently, the morbidity and mortality have improved due to the more aggressive management strategies adopted. • Introduction of aggressive therapeutic measures to reverse the adverse effects of chyle loss has led to the lowering of mortality rates for post-traumatic chylothorax. • Malignant chylothorax, chronic debilitating chylothorax and bilateral chylothoraces have worse prognosis. • The success of managing large chyle leaks involves aggressive nutritional support and early surgical intervention when indicated.
Pseudochylothorax • Pseudochylothorax, also known as chyliform pleural effusion or cholesterol pleural effusion, is the term applied to pleural fluid that mimics true chylous pleural effusion in appearance but lacks the biochemical criteria for chylothorax. • High cholesterol levels are typical of a pseudochylous pleural effusion. • Cholesterol levels are generally >200 mg/dl and may even exceed 1000 mg/dl. • The fluid may demonstrate rhomboid-shaped cholesterol crystals on microscopy, which do not stain with Sudan III stain.
Pathogenesis…. • Most patients with chyliform pleural effusions have long-standing pleural effusions (mean >5 years), and have thickened, at times, calcified pleura. • Most of the cholesterol in chyliform pleural effusions is associated with high-density lipoproteins in contrast to the cholesterol in acute exudates that is mostly bound to low-density lipoprotein (LDLs). • The precise origin of cholesterol in pseudochylothorax is unknown, but it is attributed to the continued breakdown of chronic inflammatory cells in a long-standing effusion. • Chyliform pleural effusions are usually unilateral
Causes…. • Tubercular pleural effusions account for approximately 54% of all cases. • Rheumatoid arthritis and trapped lung syndrome are rare causes of pseudochylothorax. • Patients who have had artificial pneumothoraces for pulmonary tuberculosis and in whom the lung remains atelectatic with a resultant pleural effusion are particularly prone to chyliform pleural effusions.
Clinical features • Many patients with chyliform pleural effusions are asymptomatic or at least no more symptomatic than when they initially developed the pleural effusion. • When symptoms occur, they are usually related to the underlying disease process or to the pulmonary restriction produced by the effusion and the thickened pleura.
Diagnosis • The pleural effusion is often chronic and associated with thickened or calcified pleura. • The fluid is milky, and the differential diagnoses of chylothorax and empyema need exclusion. • Cholesterol crystals—a diagnostic feature of pseudochylothorax. • The cholesterol crystals give a distinct satin-like sheen to the pleural fluid and microscopically have a typical rhomboid appearance. • Not all patients with chyliform pleural effusion have cholesterol crystals in their pleural fluid; however, most have an elevated pleural fluid cholesterol level (>250 mg/d. L, or 6. 45 mmol/L). Pleural fluid triglyceride levels can be high in pseudochylothorax.
Treatment • When a patient is diagnosed as having a chyliform pleural effusion, the possibility of tuberculosis should always be entertained. • A therapeutic thoracentesis should be performed. • Decortication should be considered if the patient is symptomatic and the underlying lung is believed to be functional.
Working algorithm in the management of chylothorax.
Results of Fluid Analysis Pseudochylothorax Chylothorax • TG level • <50 mg/dl > 110 mg/dl • Cholesterol level • >200 mg/dl < 200 mg/dl • Cholesteral crystals • Yes, common No • Chylomicrons • No Yes • Disease process is usually chronic & usually acute 2 pleural surfaces are pleural surfaces not thickened. 66