Chronic Venous Disease Gabor Menyhei MD Ph D

Chronic Venous Disease Gabor Menyhei MD, Ph. D Professor of Vascular Surgery

Classification of venous diseases • Acute superficial thrombophlebitis deep venous thrombosis injuries • Chronic venous insufficiency primary (superficial or deep) secondary (postthrombotic syndrome) arteriovenous fistula(rare)

Etiology of chronic venous insufficiency • Primary Risk factors: long-term standing, multiple birth, adiposity, genetic factors • Secondary Deep venous thrombosis Arteriovenous fistula (acquired or congenital)

Pathophysiology of chronic venous insufficiency Valve incompetence Raised venous pressure Oedema, varicose veins, skin changes, venous ulcer

Teleangiectasia

Varicose veins

Skin changes in CVI

Venous ulcer

Anatomic patterns of CVI • Superficial LSV or SSV reflux • Perforating veins • Deep veins valve incompetence occlusion

Diagnosis of chronic venous insufficiency • • • Physical examination Hand-held Doppler Duplex scan Phlebography Plethysmography Radionuclide venography

Duplex assessment
")
Treatment of venous insufficiency • • • Compression therapy Sclerotherapy Surgery Local treatment (ulcer) Venotonic drugs

Surgery in superficial insufficiency • High ligation of long or short saphenous vein • Stripping • Multiple avulsions

High ligation

Stripping of LSV



Stripping of LSV

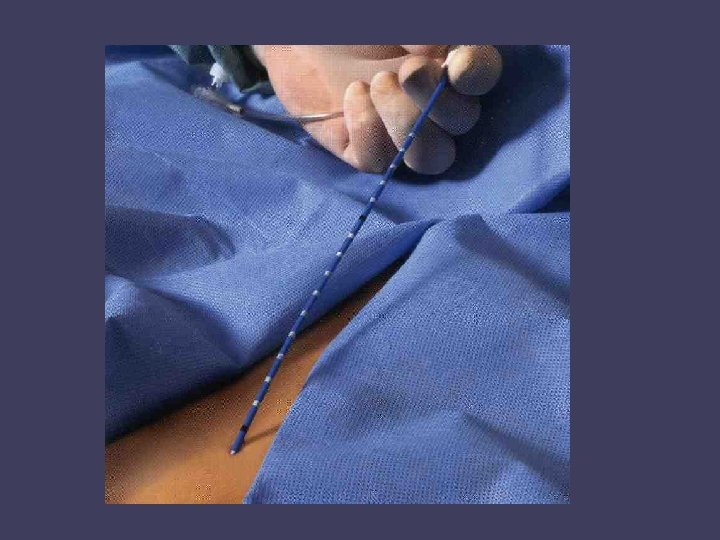
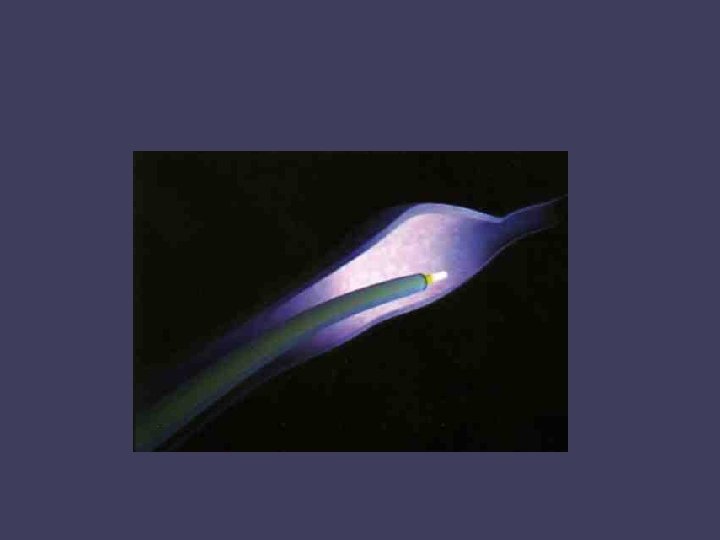
Endovenous laser treatment

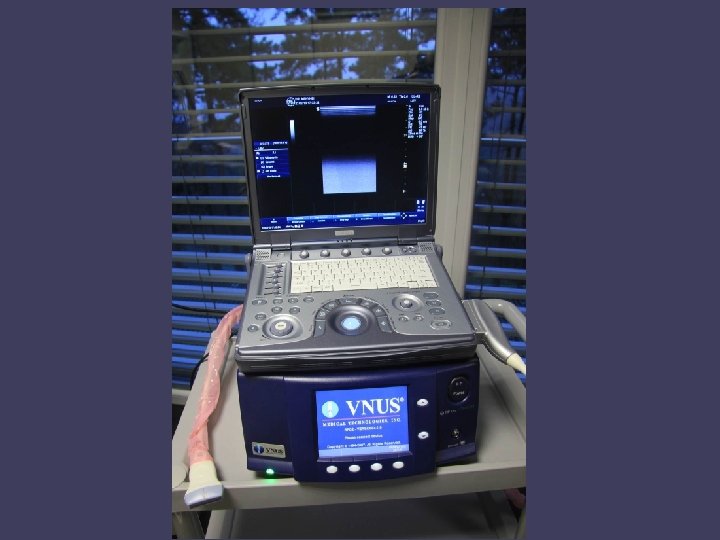
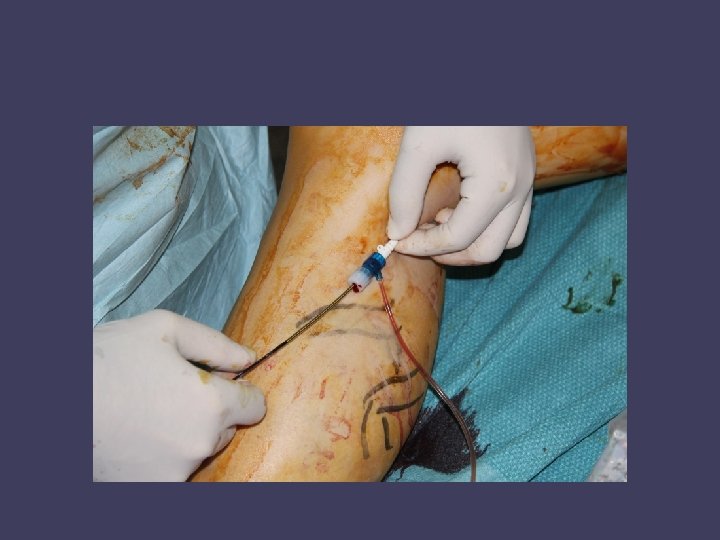
Radiofrequency ablation

Surgery of incompetent perforators • Ligation of perforators through small incisions • Cockett operation (one long medial incision) • Endoscopic dissection (SEPS)

Perforator vein incompetence

SEPS

Löfqvist tourniqet for SEPS

SEPS – Two-port technique

Advantages of SEPS • • • Minimally invasiv Less complications Shorter hospital stay Shorter recovery Good cost-benefit

Mid term clinical outcome after subfascial endoscopic perforator surgery CEAP grade C 6 n=40 C 4 -5 n=11 Total n=51 Healed/Improved Unchanged Ulcer recurred 25 (62%) 7 (18%) 8 (20%) 8 2 1 33 (64%) 9 (18%) C 4 : skin changes, C 5: healed ulcer, C 6: active ulcer

Surgery of deep vein occlusion • Palma operation if chronic iliac vein occlusion femoro-femoral crossover saphenous bypass
")
Femoro-femoral crossover saphenous bypass (Palma operation)

Dinamic radionuclide venography after Palma operation
 Phlebography findings Improved Unchang ed")
Long term results of Palma operation (after 6 years) Phlebography findings Improved Unchang ed Total Iliac vein occlusion and intact deep veins below 10 (83%) 2 (17%) 12 Iliac vein occlusion and postthrombotic deep veins below 19 (64%) 11 (46%) 30 Total 29 (69%) 13 (31%) 42
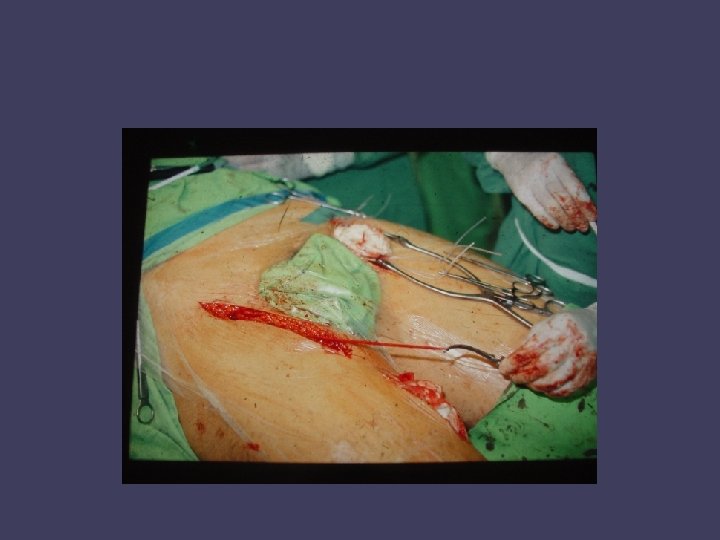

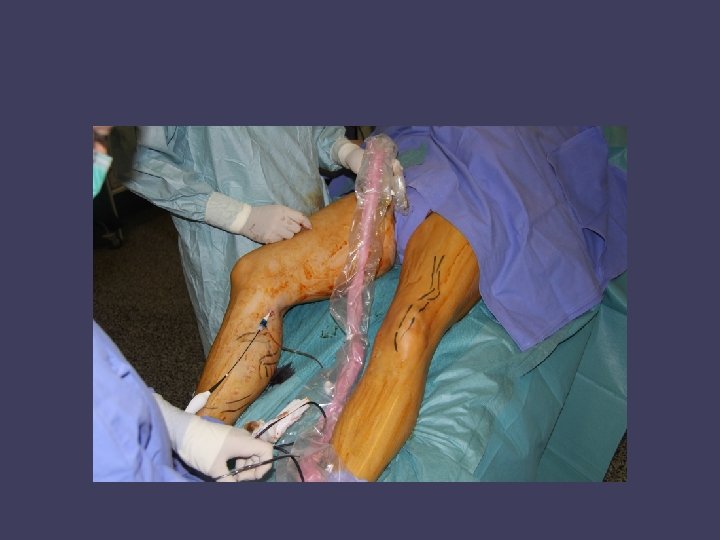
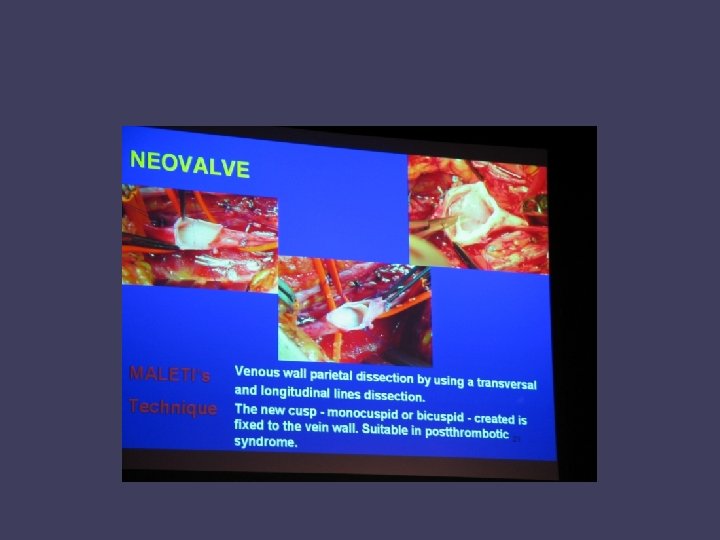
Surgery of deep vein incompetence • Vein segment transplantation • External or internal valvuloplasty • Vein transposition

Primary deep vein incompetence: External or internal valve plasty Ulcer free at 5 years: 65 -83% Kistner, 1996. Raju, 2000.
 deep vein incompetence: Vein-segment transplantation Ulcus recurrence at 5 years: - if")
Secunder (postthrombotic) deep vein incompetence: Vein-segment transplantation Ulcus recurrence at 5 years: - if good patient compliance: 29% - if not: 100% Mayberry, 2002

Vein segment transplantation

Thank you for your attention.
- Slides: 43