CHRONIC TONSILLITIS By Dr Sharwak Ramlan Is an

CHRONIC TONSILLITIS By Dr Sharwak Ramlan

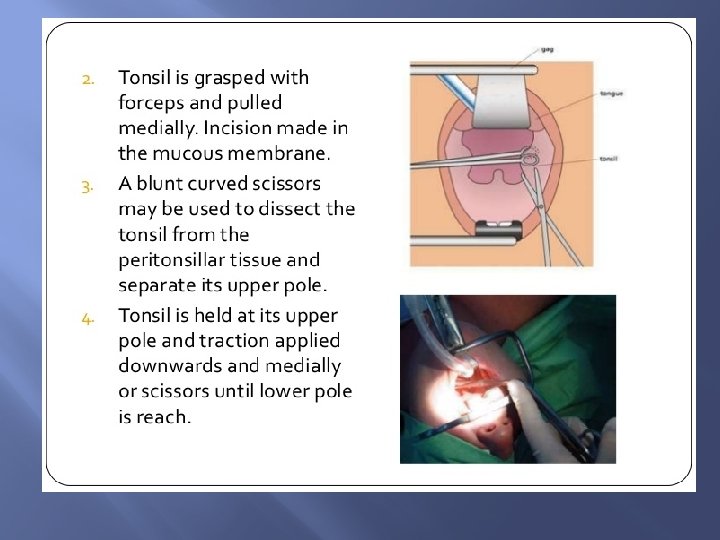
� Is an ovoid mass of lymphoid tissue � Situated in lateral wall of oropharynx b/w anterior and posterior pillars. � It has 2 surfaces: medial/lateral 2 poles: upper/lower.

Medial surface Covered by non keratinizing stratified sqamous epithelium which dips into crypts Opening of 12 -15 crypts can be seen on medial surface One of the crypt situated in the upper part of tonsil is very large and deep – CRYPTA – MAGNA/INTRATONSILLAR CLEFT - represents ventral part of 2 nd pharyngeal pouch From main crypt arises secondary crypt. Crypt serve to inc surface area of tonsils. Crypts filled with cheesy material- epithelial. Cell, bacteria, food debris. Can be expressed by pressure over the anteriorpillar

Lateral surface � fibrous capsule � B/W capsule and bed of tonsil- LOOSE AREOLAR TISSUE. � It makes easy to dissect in the plane � Site for collection of pus in peritonsillar abscess(QUINSY)

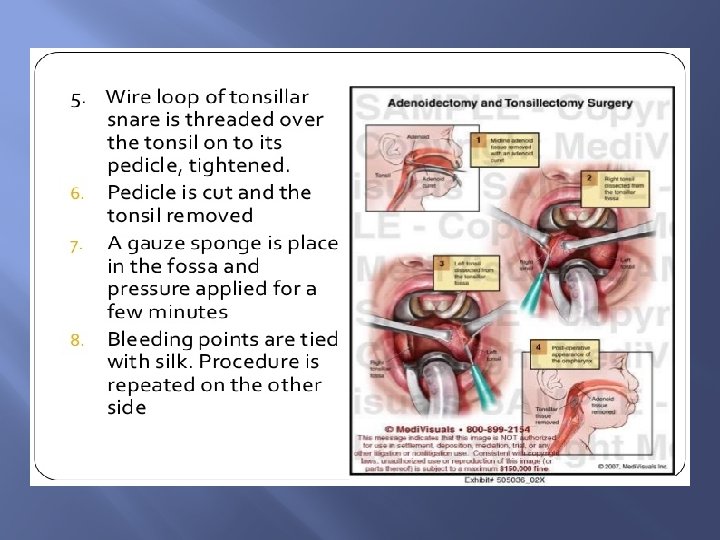
Upper pole � It extends into soft palate � Medial surface is covered by semilunar fold extending b/w anterior & posterior pillar – enclosing a potential space --- SUPRA TONSILLAR FOSSA

Lower pole � � Attached to tongue A triangular fold of mucous membrane extends from ant: pillars to anteroinferior part of tonsil. � It encloses a space --- ANTERIOR TONSILLAR SPACE. � Tonsil is seperated from tongue by a sulcus--TONSILLO LINGUAL SULCUS---- seat of carcinoma.

Bed of tonsil
 2. Ascending pharyngeal artery from")
Blood supply 1. Tonsilar branch of facial artery (MAIN) 2. Ascending pharyngeal artery from external carotid artery 3. Ascending palatine branch of facial artery 4. Dorsal linguae branches of lingual artery 5. Descending palatine branch of maxillary artery

Venous drainage Veins from tonsil Paratonsillar vein Common facial vein & pharyngeal venous plexus
 � Glossopharyngeal nerve")
Nerve supply � Lesser palatine branches of sphenopalatine ganglion (CN V) � Glossopharyngeal nerve provide sensory nerve supply.

Functions of tonsils � � Act as sentinels to guard against foreign intruders like , viruses , bacteria & other antigens coming in contact through inhalation & ingestion. Two mechanisms: 1. Providing local immunity 2. Providing a surveillance mechanism so that entire body is prepared for defence. Both these mechanisms are operated through humoral and cellular immunity.

Chronic tonsillitis � May be complication of acute tonsillitis � Subclinical infections of tonsils with out an acute attack. � Mostly affects children and young adults. Rare after 50 yrs � Chronic infections in teeth or sinuses.

Types � Chronic follicular tonsillitis: tonsillar crypts are full of infected cheesy material shows as yellow spots on the surfaces. � Chronic parenchymatous : hyperplasia of lymphoid tissue. Tonsils are very much enlarged and may interfere with speech, deglutition, & respiration. Attacks of sleep apnoea may ocurr Long standing cases develope features of cor pulmonale.

� � � Chronic fibroid tonsillitis : tonsils are small but infected, with H/O repeated sore throats CLINICAL FEATURES Recurrent attacks of sore throat or acute tonsillitis. Chronic irritation in throat with cough Bad taste in mouth / foul breath(halitosis) due to pus in crypts. Difficulty in swallowing

Examination � � � Tonsils show varying degree of enlargement. Some times they meet in midline(CHRONIC PARENCHYMATOUS TYPE) Yellowish beads of pus on medial surface of tonsil (CHRONIC FOLLICULAR TYPE) Tonsils are small; Pressure on anterior pillar expresses frank pus/ cheesy material (CHRONIC FIBROID TYPE) Flushing of anterior pillar – important sign Enlargement of jugulodigastric lymph node

TREATMENT � Conservative Treatment – General health, diet, treatment of co-existent infection of teeth, nose & sinuses � Tonsillectomy – Indicated when tonsil interfere with speech, deglutition & respiration or in recurrent attacks

COMPLICATIONS 1. 2. 3. 4. 5. 6. Peritonsillar Abscess Parapharyngeal Abscess Intratonsillar Abscess Tonsillolith Tonsillar Cyst Focus of infection like Rheumatic Fever, Acute Glomerulo Nephritis, Eye & Skin Disorders
 2) 3) 4) 5) Absolute Recurrrent infection of throat Peritonsillar")
TONSILLECTOMY INDICATION A. 1) 2) 3) 4) 5) Absolute Recurrrent infection of throat Peritonsillar Abscess Tonsillitis Hypertrophy of tonsil Suspicion of malignancy B. 1) 2) 3) 4) C. 1. 2. 3. Relative Diphtheria Carriers Streptococcal Carriers Chronic Tonsillitis With bad taste Recurrent Streptococcal Tonsillitis As a part of another Operation Palaptopharyngoplasty Glossopharyngeal Neurectomy Removal of Styloid Process

� � � � HB level less than 10 g% Presence of acute infection (risk of bleeding) Children under 3 yrs Overt or submucous cleft palate Bleeding disorders At the time of epidemic polio Uncontrolled systemic diseases During the period of menses

� ANAESTHESIA : GA � POSITION : Rose’s position : pt lies supine with head extended by placing a pillow under shoulders a rubber ring placed under head to stabilize it

STEPS

Post operative care IMMEDIATE GENERAL CARE � Keep the pt in coma position untill fully recovered from anaesthesia � Keep a watch on bleeding from the nose & mouth � Keep check on vital signs DIET � After fully recovered –liquids , cold milk or ice creams � Soft to solid � Plenty of fluids

ORAL HYGIENE : Condy’s or salt water gargle 3 -4 times a day. � Mouth wash with plain water after every feed. ANALGESIC ANTIBIOTICS

Complications IMMEDIATE 1. Primary haemorrhage : at the time of operation controlled by pressure, ligation or electrocoagulation 2. Reactionary haemorrhage : within a period of 24 hr 3. Injury to tonsillar pillars, uvula, soft palate, tongue, superior constrictor muscle 4. Injury to teeth 5. Aspiration of blood 6. Facial oedema 7. Surgical emphysema

DELAYED 1. Secondary haemorrhage : B/W 5 th to 10 th post OP days. It is the result of sepsis & premature seperation of membrane 2. Infection : of tonsillar fossa lead to parapharyngeal abscess or otitis media 3. Lung complications : aspiration – atelectasis/lung abscess 4. Scarring in soft palate and pillars 5. Tonsillar remenants : repeated infections 6. Hypertrophy of lingual tonsils : compensatory to loss of palatine tonsils.

Other methods � � � � � Guillotine method Electrocautery Laser tonsillectomy(co 2 or KTP-512) (in coagulation disorder) Laser tonsillotomy(reduce size of tonsil) Intra capsular tonsillectomy : powered instrument – debrider Harmonic scalpel (ultasound) Plasma-mediated ablation technique : protons are energized to break molecular bonds b/w tissue. Coblation tonsillectomy Cryosurgical technique

THANK YOU
- Slides: 29