CHRONIC SUUPURATIVE OTITIS MEDIA Chronic suppurative otitis media
 is a long-standing infection (3")
 Anteroinferior part of middle ear")



 Presence of granulations, in-growth of squamous epithelium from")

- Slides: 11
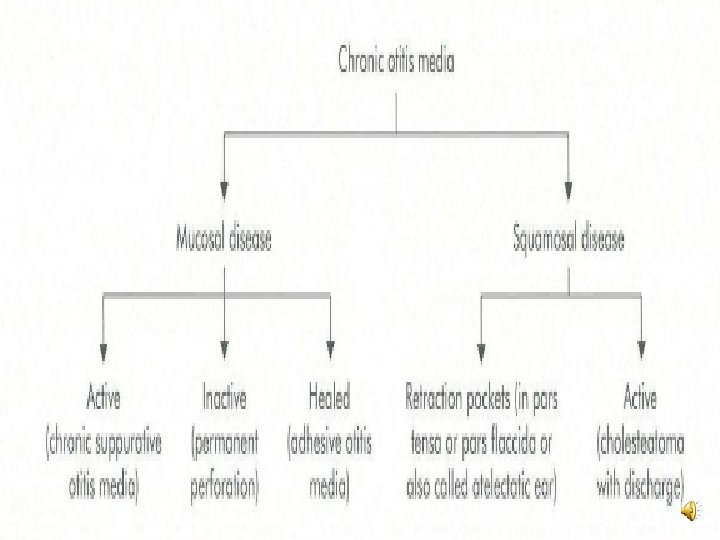
CHRONIC SUUPURATIVE OTITIS MEDIA Chronic suppurative otitis media (CSOM) is a long-standing infection (3 months) of a part or whole of the middle ear cleft characterised by ear discharge and a permanent perforation. Permanent perforation • Edges are covered by squamous epithelium. • Does not heal spontaneously. • Epithelium-lined fistulous track.
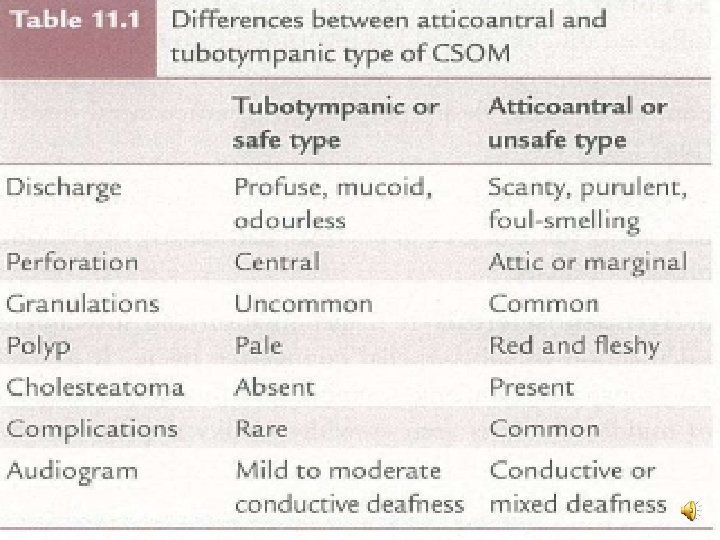
Types of CSOM • Tubotympanic (safe or benign type) Anteroinferior part of middle ear cleft, i. e. eustachian tube and meso tympanum associated with a central perforation. No risk of serious complications. • Atticoantral (unsafe or dangerous type) Posterosuperior part of the cleft (i. e. attic, antrum and mastoid) with an attic or a marginal perforation. (boneeroding process such as cholesteatoma, granulations or osteitis) Risk of complications is high in this variety.
MICROBIAL SPECTRUM • Common aerobic organisms are Ps aeruginosa, Proteus, Esch. coli and Staph, aureus, while anaerobes include Bacteroides fragi. Us and anaerobic Streptococci.
CLINICAL FEATURES • Ear discharge a. Non-offensive, mucoid or mucopurulent, constant or intermittent. b. Upper respiratory tract infection or on accidental entry of water into the ear. • Hearing loss a. Conductive type; severity varies but rarely exceeds 50 d. B. Paradoxical effect, i. e. hears better in the presence of discharge than when the ear is dry. This is due to "round window shielding effect" produced by discharge which helps to maintain phase differential. In the dry ear with perforation, sound waves strike both the oval and round windows simultaneously, thus cancelling each other's effect. c. In long standing cases, cochlea may suffer damage due to absorption of toxins from the oval and round windows and hearing loss becomes mixed type.
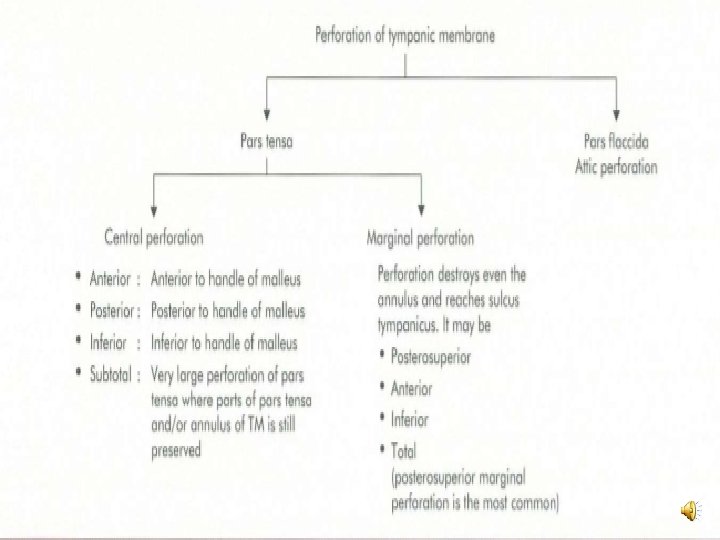
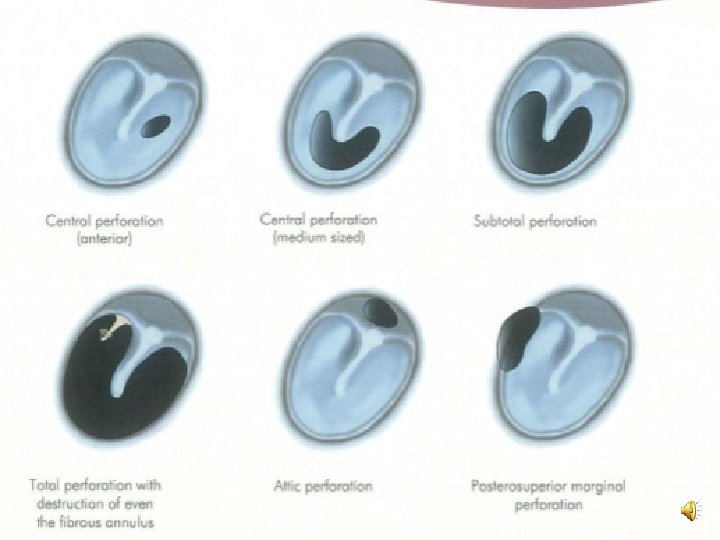
CLINICAL FEATURES • Perforation a. Always central, anterior, posterior or inferior to the handle of malleus. b. Small, medium or large or extending up to the annulus, i. e. subtotal. • Middle ear mucosa. (pale pink and moist) a. Inflamed looks red, oedematous and swollen. b. Polyp
Investigations • Examination under microscope (EUM) Presence of granulations, in-growth of squamous epithelium from the edges of perforation, status of ossicular chain, tympanosclerosis and adhesions. An ear which appears dry may show hidden discharge under the microscope. Rarely, cholesteatoma may co-exist with a central perforation and can be seen under a microscope. • Audiogram Assessment of degree of hearing loss and its type. (conductive but a sensorineural t may be present). • Culture and sensitivity of ear discharge. • Mastoid X-rays/CT scan temporal bone Mastoid is usually sclerotic but may be pneumatised with clouding of air cells. There is no evidence of bone destruction. (bone destruction is a feature of atticoantral disease).
TREATMENT Control infection and eliminate ear discharge and at a later stage, to correct the hearing loss by surgical means. • Aural toilet • Ear drops • Systemic antibiotics • Precautions • Treatment of contributory causes • Surgical treatment Aural polyp or granulations • Reconstructive surgery Once ear is dry, myringoplasty with or without ossicular reconstruction can be done to restore hearing.