CHRONIC OTITIS MEDIA Classification of Chronic Otitis Media





































 • Metaplasia • Epithelial migration")



")












")










- Slides: 76
CHRONIC OTITIS MEDIA
Classification of Chronic Otitis Media • Chronic Non Suppurative Otitis Media – Otitis media with effusion “OME” – Adhesive otitis media • Chronic Suppurative Otitis Media “CSOM” – Tubotympanic (Safe) – Atticoantral (Unsafe)
OTITIS MEDIA WITH EFFUSION
DEFINITION Presence of non-purulent fluid within the middle ear cleft
SYNONYMS • • Secretory otitis media Middle ear effusion Sero-mucinous otitis media Catarrhal otitis media Glue ear Serous otitis media Non-suppurative otitis media
PREVALENCE • Between 20% and 50% of children do have OME at some time between 3 and 10 years of age • Two peaks at 2 and 5 years of age
RISK FACTORS • • Race Age Gender Season Nasopharyngeal anatomical abnormalities Cleft palate Smoking ? Allergy
HISTOPATHOLOGY • Changes in the mucosa – Vasodilatation & mononuclear cell infiltration – Metaplasia of the epithelium to ciliated columnar – Mucus secreting gland formation • Formation of fluid in the middle ear – Transudate – Exudate – Secretion
ETIOPATHOLOGY • Eustachian tube dysfunction • Chronic inflammation
ETIOLOGY • Eustachian tube dysfunction – Poor muscular function – Adenoids – Barotrauma – Others • Infections – Unresolved AOM – Adenoiditis and other URTIs
SYMPTOMS • Hearing impairment • ± Otalgia • Fluid sensation
Diagnosis
DIAGNOSIS
DIAGNOSIS • Otoscopy • Tuning fork tests
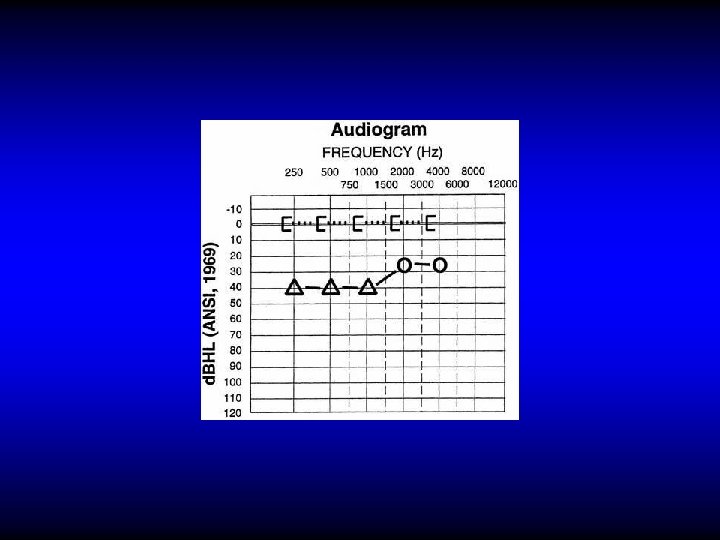
DIAGNOSIS • Otoscopy • Tuning fork tests • PTA
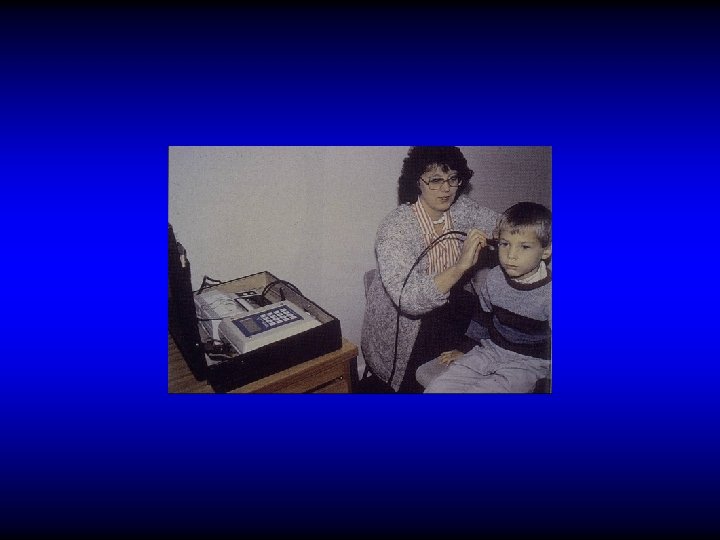
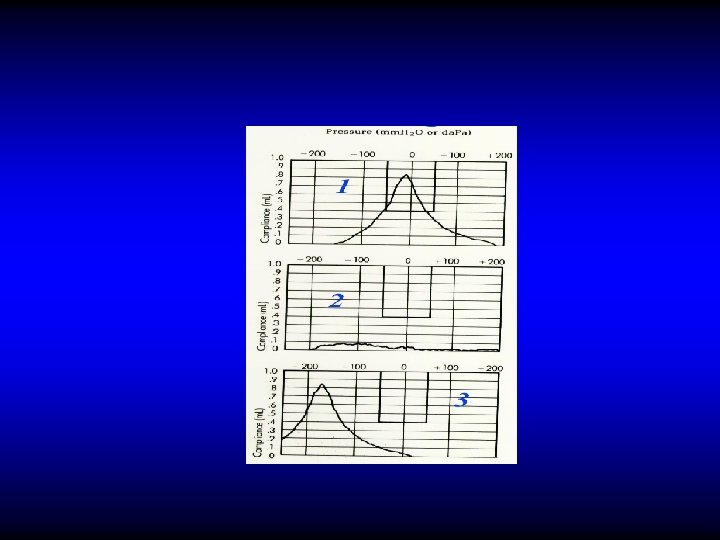
DIAGNOSIS • Otoscopy • Tuning fork tests • PTA • Tympanometry
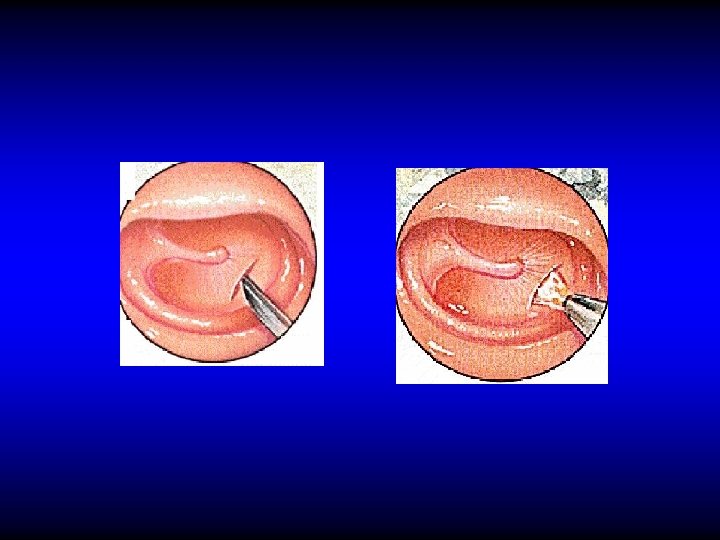
DIAGNOSIS • Otoscopy • Tuning fork tests • PTA • Tympanometry • Myringotomy
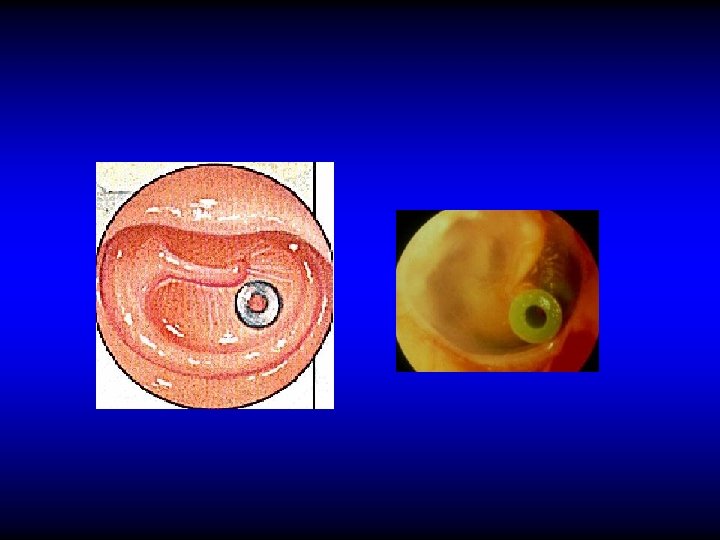
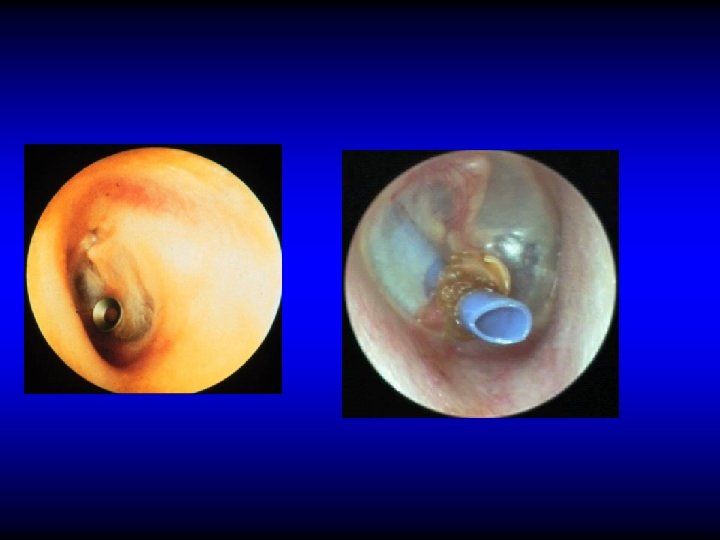
TREATMENT • Treatment of the cause if feasible • Observation • Medical treatment – Antibiotics – Decongestants, ? Auto-inflation – ? Steroids • Surgical – Myringotomy – Ventilation tubes (grommets)
COMPLICATIONS OF VENTILATION TUBES INSERTION • Infection • Blockage • Extrusion • Tympanosclerosis • Perforation
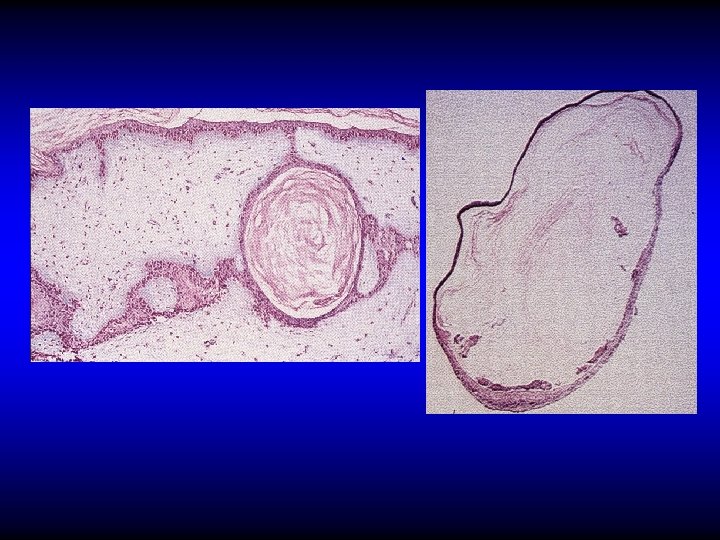
Iatrogenic Cholesteatoma
FACTORS AFFECTING TREATMENT • • Age Duration Unilateral or bilateral Degree of hearing impairment Previous treatment Associated conditions Tympanic membrane changes Others
SEQUELAE • Spontaneous resolution – 50% resolve within 3 months. Only 5% persists for more than 12 months • Tympanosclerosis • Scarring, retraction and atelectasis • Cholesteatoma
Conclusion • OME is very common in children • Etiology is associated with ET dysfunction and or chronic infection • In adults: Nasopharyngeal pathology should be considered • Most cases resolve spontaneously • Conservative treatment is of doubtful value • VT insertion restore hearing in the selected cases
Classification of Chronic Otitis Media • Chronic Non Suppurative Otitis Media – Otitis media with effusion “OME” – Adhesive otitis media • Chronic Suppurative Otitis Media “CSOM” – Tubo-tympanic (Safe) – Attico-antral (Unsafe)
Chronic Adhesive Otitis Media • Formation of adhesion in the middle ear after reactivation and subsequent healing of either CSOM or OME
Clinical Features • History of CSOM or OME • Deafness is usually the only symptoms • TM shows various structural changes
Treatment • Observation • Surgical treatment • Hearing aid
Classification of Chronic Otitis Media • Chronic Non Suppurative Otitis Media – Otitis media with effusion “OME” – Adhesive otitis media • Chronic Suppurative Otitis Media “CSOM” – Tubo-tympanic (Safe) – Attico-antral (Unsafe)
CHRONIC SUPPURATIVE OTITIS MEDIA
ETIOLOGY • Environmental • Genetic • Previous OM • Upper respiratory tract infections • Eustachian tube dysfunction
CLINICO-PATHOLOGICAL TYPES Tubo-tympanic Attico-antral
PATHOLOGY • Signs of suppurative infection – Discharge & perforation – Chronic inflammatory reaction in the mucosa and the bone (ostietis) • Signs of healing attempts – Granulation tissue & polyps – Fibrosis & tympanosclerosis • Cholesteatoma (attico-antral type)
CHOLESTEATOMA
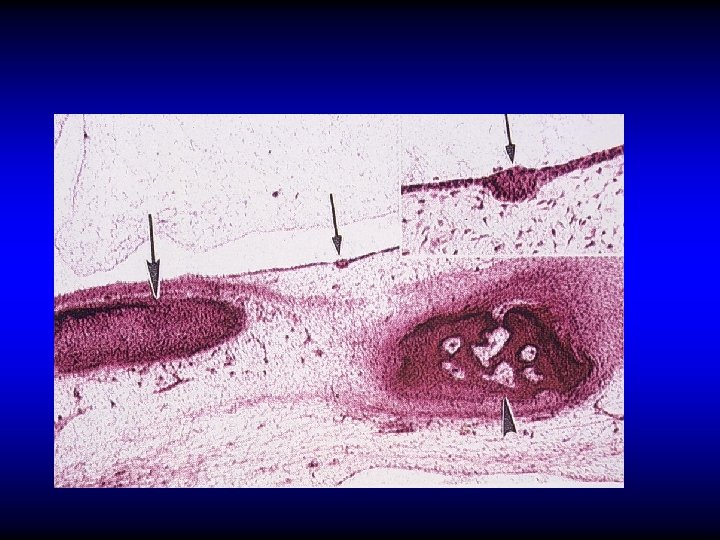
DEFINITION • The presence of a desquamating stratified squamous epithelium in the middle ear
PATHOGENESIS OF CHOLESTEATOMA • Implantation (congenital or acquired) • Metaplasia • Epithelial migration
CLASSIFICATION OF CHOLESTEATOMA • Congenital • Acquired – Primary – Secondary
Effect of Cholesteatoma • Keratin encourages persistence of the infection • Matrix causes bone erosion
Clinical Features of CSOM
CLINICO-PATHOLOGICAL TYPES Tubo-tympanic Attico-antral (cholesteatoma)
SYMPTOMS OF CSOM • Otorrhea – Intermittent, profuse & odorless in TT type – Persistent, scanty & malodorous in AA type • Deafness • Tinnitus N. B. Any other symptom means complication
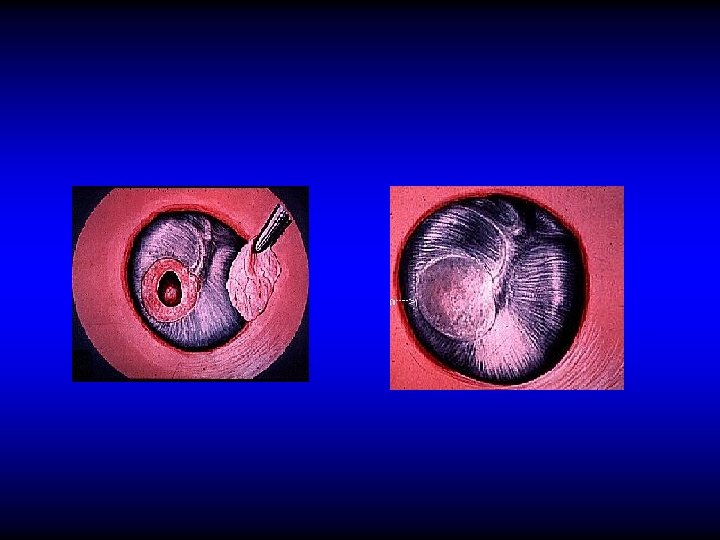
OTOSCOPIC EXAMINATION • Discharge – Present in TT type if active but may be absent – Usually is present in AA type • Perforation – Central: in TT type – Marginal or attic in AA type with cholesteatoma
PERFORATION IN TT CSOM
PERFORATION IN AA CSOM
OTOSCOPIC EXAMINATION • Discharge – Present in TT type if active but may be absent – Usually is present in AA type • Perforation – Central: in TT type – Marginal or attic in AA type with cholesteatoma • Polyps, granulation tissue, tympanosclerosis
Bacteriology
INVESTIGATIONS • Audiometry • Bacteriology • Imaging
Congenital Cholesteatoma
Cloudy middle ear in CSOM
Cholesteatoma with attic erosion
TREATMENT OF CHRONIC SUPPURATIVE OTITIS MEDIA • Depends on the type and presentation
Active TT type Inactive TT type Attico-antral type (usually active)
Conservative treatment Active TT type Inactive TT type Conservative Treatment • Treat any predisposing factor • Keep the ear dry TYMPANOPLASTY • Ear toilet • Antibiotics • Removal of polyps and granulations
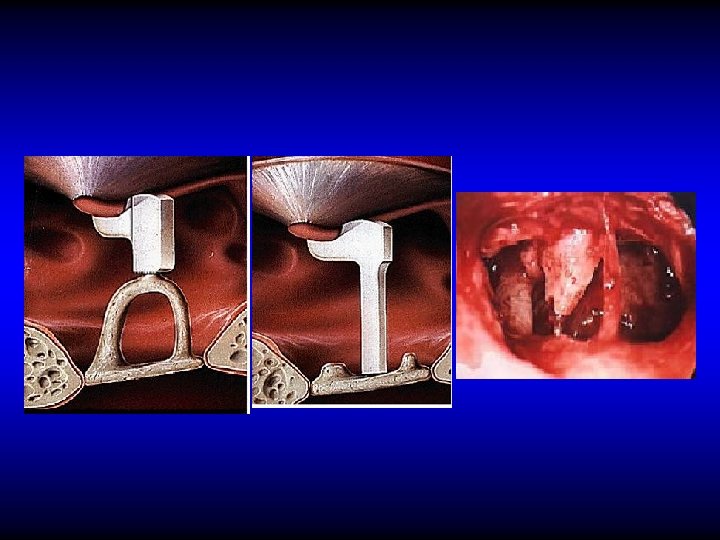
TYMPANOPLASTY An operation performed to eradicate disease in the middle ear cavity and to reconstruct the hearing mechanism
MYRINGOPLASTY An operation performed to repair the tympanic membrane
AIMS OF TYMPANOPLASTY • To close the perforation • To prevent re-infection • To improve hearing
TREATMENT OF ATTICOANTRAL CSOM Removal of cholesteatoma by mastoid operation
RADICAL MASTOIDECTOMY An operation in which the mastoid antrum and air cells, attic and middle ear are converted into common cavity, exteriorized to the external canal. The tympanic membrane, malleus and incus are removed leaving only the stapes in situ.
MODIFIED RADICAL MASTOIDECTOMY An operation in which the mastoid antrum and air cells, attic and middle ear are converted into common cavity, exteriorized to the external canal. The tympanic membrane and ossicles remnants are retained
AIMS OF RADICAL & MODIFIED RADICAL MASTOIDECTOMY • Safety • Dry ear • Preserve hearing
Conclusion • In TT type the discharge is usually copious, intermittent and odorless. The perforation is central. Treatment is conservative (if there is active infection) followed by tympanoplasty to prevent re-infection and improve hearing. • In the AA type the discharge is usually scanty, persistent and of bad odor. The perforation is attic or marginal with cholesteatoma. Treatment is by mastoidectomy to provide safety and dry ear
THANK YOU