Chronic obstructive pulmonary diseases Chronic obstructive pulmonary diseases

Chronic obstructive pulmonary diseases
,")
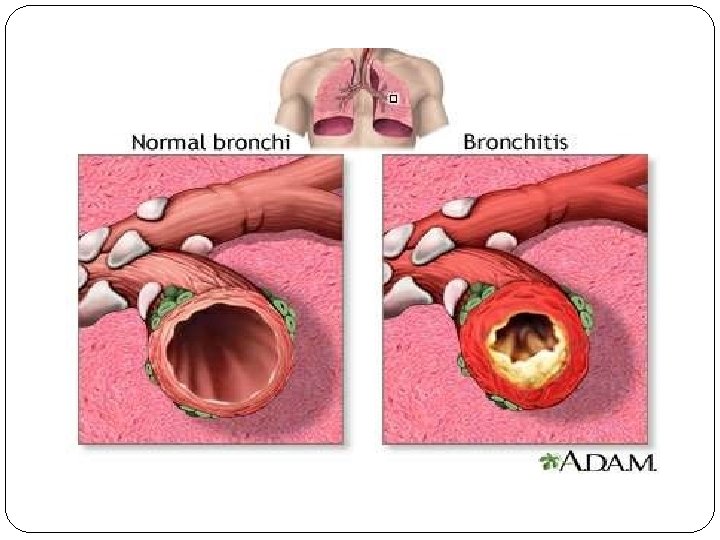
Chronic obstructive pulmonary diseases COPD is also known as chronic obstructive lung disease (COLD), chronic obstructive airway disease (COAD), chronic airflow limitation (CAL) and chronic obstructive respiratory disease (CORD) Chronic obstructive pulmonary disease (COPD) refers to chronic bronchitis and emphysema, a pair of two commonly coexisting diseases of the lungs in which the airways become narrowed.

This leads to a limitation of the flow of air to and from the lungs causing shortness of breath.

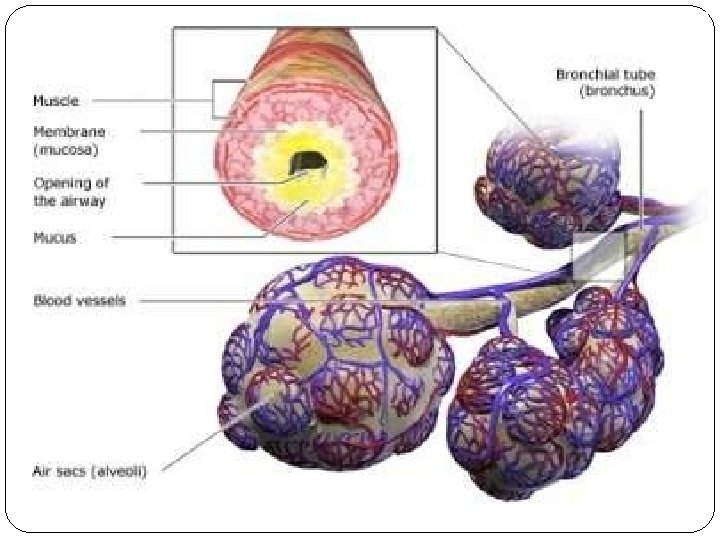
In COPD, less air flows in and out of the airways because of one or more of the following: �The airways and air sacs lose their elastic quality. �The walls between many of the air sacs are destroyed. �The walls of the airways become thick and inflamed. �The airways make more mucus

Incidence �It is the 4 th leading cause of mortality and 12 th leading cause of disability in the united states. �In 2020 COPD is the 3 rd leading cause of death.

CAUSES Smoking is primary risk factors for COPD. The numerous irritants found in cigarette smoke stimulate excess mucus production and coughing, destroy ciliary function and lead to inflammation and damage of bronchiolar and alveolar walls.


Air pollution high levels of urban air pollution are harmful to persons with existing lung disease. However, the effect of outdoor air pollution as a risk factor for COPD. Another risk factor for COPD development is fossil fuels that used for indoor heating and cooking.

Occupational exposures- exposure to workplace dusts found in coal mining, gold mining, and the cotton textile industry and chemicals such as fumes from welding have been implicated in the development of airflow obstruction. Exposure of these irritants causes the airway to be hyper responsive.

Infection : infections is risk factor for developing COPD. Severe recurring respiratory tract infection in childhood have been associated with reduced lung function and increased respiratory symptoms in adulthood. Recurring infections impair normal defense mechanisms, making bronchioles and alveoli more susceptible to injury.

Genetics-Alpha 1 -antitrypsin deficiency is a genetic condition that is responsible for about 2% of cases of COPD. In this condition, the body does not make enough of a protein, alpha 1 -antitrypsin. Alpha 1 antitrypsin protects the lungs from damage caused by protease enzymes, such as elastase and trypsin, that can be released as a result of an inflammatory response to tobacco smoke

RISK FACTORS FOR COPD

Pathophysiology

CLINICAL FEATURES �Chronic cough �Sputum production �Wheezing �Chest tightness �Dyspnoea on exertion �Wt. loss �Respiratory insufficiency �Respiratory infections �Barrel chest- chronic hyperinflation leads to loss of lung elasticity.

In later stages: CO 2 elimination is disturbed and increase in CO 2 tension in arterial blood causing respiratory acidosis

DIAGNOSIS Blood Test Blood tests can help determine if symptoms are being caused by an infection. An arterial blood gas test will measure the amount of oxygen in blood. This is one indication of how well lungs are working. This can help doctor determine how severe COPD is and whether need oxygen therapy.

. Chest X-ray or CT scan A CT scan is a type of X-ray that creates a more detailed image than a standard X-ray. Whichever type doctor chooses, an X-ray will give a picture of the structures inside chest. These include your heart, lungs, and blood vessels. Your doctor will be able to see if client has evidence of COPD. If symptoms are being caused by another condition such as heart failure, the doctor will be able identify that as well

Sputum Examination Doctor may order a sputum examination, especially if the client has a productive cough. Sputum is the mucus the client cough up. Analyzing sputum can help identify the cause of breathing difficulties and may rule out some lung cancers. If there is a bacterial infection, it can be identified and treated. ECG The doctor might request an ECG to determine if your shortness of breath is being caused by a heart condition.
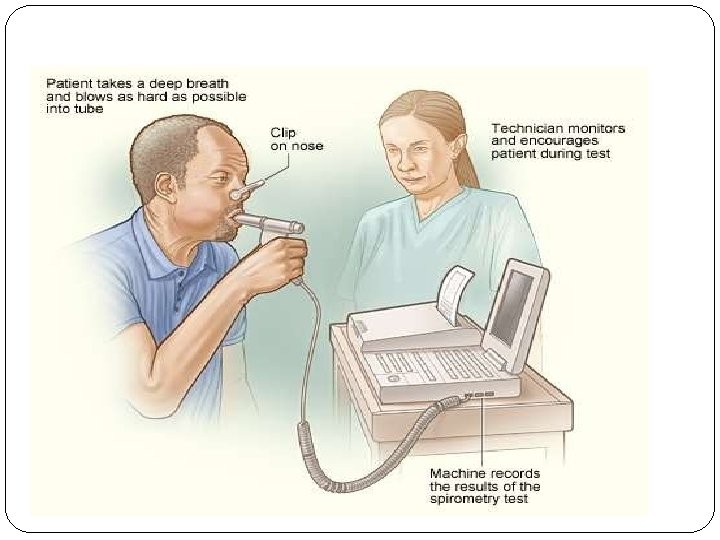
 is the most common of the pulmonary function")
�Spirometry (meaning the measuring of breath) is the most common of the pulmonary function tests (PFTs). It measures lung function, specifically the amount (volume) and/or speed (flow) of air that can be inhaled and exhaled.

MANAGEMENT MEDICAL MANAGEMENT SURGICAL MANAGEMENT NURSING MANAGEMENT

MEDICAL MANAGEMENT The treatment goal for the client with COPD are: To improve ventilation To facilitate the removal of bronchial secretions To promote health maintenance To reduce complications, and To slow progression of the disease

Smoking cessation Cessation of cigarette smoking is single most effective and cost effective intervention to reduce the risk of developing COPD and stop the progression of the disease. After discontinuation of smoking, the accelerated decline in pulmonary function slows and pulmonary function usually improves.

Drug therapy Medications for COPD: Reduce symptoms Increase the capacity of exercise, Improve overall health and Reduce the severity of exacerbations.

Bronchiodilator drug therapy are agents that widen the air passages by relaxing the bronchial smooth muscle and improve the ventilation of lungs. They are usually administered via inhalation route but in rare occasions may be given orally or administered intravenously. Regular treatment with long acting bronchiodilators is more effective and convenient than treatment with short acting forms.

The principal bronchiodilator treatment are Beta 2 agonists, anticholinergics, and methylxanthines used singly or combination. The choice of bronchioldilators depends on availability and patient’s response. Beta 2 agonists are sympathomimetic drugs that acts on the beta-adrenoceptors in the smooth muscles of the airway and cause bronchioldilation. These drugs may also enhance mucus clearance and improve the endurance of respiratory muscles.
have minimal adverse effects with rapid onset")
�Short acting Beta 2 agonists(e. g. , albuterol)have minimal adverse effects with rapid onset of action, a peak effect in 60 to 90 minutes and duration of 4 to 6 hour. �Side effects that may develop with the use of these drugs are tachycardia, tremor, nervousness, and nausea.

Oxygen therapy O 2 therapy is frequently used in the treatment of COPD another problem associated with hypoxemia. Long term o 2 therapy improves survival, exercise capacity, cognitive performance and sleep in hypoxemic patients. O 2 is colorless, odorless testless gas that constitutes 20. 95% of the atmosphere. O 2 raises the partial pressure of oxygen(PO 2) in inspired air. Indications for use: goals for 02 therapy are �To reduce the work of breathing, �To maintain the Pa. O 2 �To reduce the workload of heart �To keep the Sa. O 2 more than 90% during rest

Oxygen is usually administered to treat hypoxemia caused by �Respiratory disorders such as COPD pulmonary hypertension pneumonia and pulmonary emboli �Cardiovascular disorders such as myocardial infraction, angina pectoris and cardiogenic shock �Central nervous system disorders such as overdose of opiods

SURGICAL MANAGEMENT bullectomy Bullae are enlarged airspaces that do not contribute to ventillation but occupy space in the thorax, these areas may be surgically excised lung volume reduction surgery It involves the removal of a portion of the diseased lung parenchyma. this allows the functional tissue to expand. lung transplantation

Nursing management Nursing diagnosis Impaired gas exchange related to decreased ventilation Objectives Improve ventilation Intervention a. Monitor lung sounds every 4 to 8 hours. b. Perform chest physiotherapy c. Advice the client to drink at least 8 to 10 glasses of fluid per day unless contraindicated d. Teach the client in coughing technique e. Asses the condition of oral mucus membrane and perform oral care

Nursing diagnosis Disturbed sleep pattern related to dyspnea Objectives Getting adequate rest Intervention �Promote relaxation by providing a darkened, quiet environment, ensure adequate room ventilation. �Avoid use of sleeping pills �Schedule care activities to allow periods of uninterrupted sleep.

Nursing diagnosis Activity intolerance related to inadequate oxygenation Objective Improve to perform daily activity Intervention �Monitor the severity of dyspnea �Stop or slow any activity that leads to change in respiratory rate �Advice the client to avoid conditions that increase oxygen demand

Nursing diagnosis Anxiety related to acute breathing difficulties and fear of suffocation Objectives Relieve fear of dying Intervention �Provide a quiet, calm environment. �During acute episodes, open doors and curtains and limit the number of people in the room. �Encourage the use of breathing retraining and relaxation technique �Give sedative and tranquilizers with extreme caution. �Nonpharmacological methods of anxiety reduction are more useful

Nursing diagnosis Ineffective airway clearance related to excessive secretions and ineffective coughing Objective Effective airway clearance Intervention �Monitor lung sounds every 4 to 8 hours. �Perform chest physiotherapy �Advice the client to drink at least 8 to 10 glasses of fluid per day unless contraindicated �Teach the client in coughing technique �Asses the condition of oral mucus membrane and perform oral care

Complications �More frequent lung infections, such as pneumonia. �An increased risk of thinning bones (osteoporosis), especially if you use oral corticosteroids. �Problems with weight. If chronic bronchitis is the main part of your COPD. �Heart failure affecting the right side of the heart (cor pulmonale). �A collapsed lung (pneumothorax). �Sleep problems.
- Slides: 38