Chronic Obstructive Pulmonary Disease COPD Spring 2014 References
 Spring 2014")
Chronic Obstructive Pulmonary Disease (COPD) Spring 2014

References • Pharmacotherapy: A Pathophysiologic Approach • Pharmacotherapy: Principles and Practice • Applied Therapeutics: The Clinical Use of Drugs • The Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines (Feb 2014) http: //www. goldcopd. com

Case Study Chief complaint : A 67 year old man presents to the chest clinic with a three month history of increasing shortness of breath and decreased exercise tolerance. 3

History: He was in his usual state of health until three months ago when he began to experience dyspnea while climbing stairs. He denies any acute changes in his breathing, but he does have a chronic cough that produces one to two tablespoons of clear sputum daily. The cough and sputum production have not recently changed. He smokes one pack of cigarettes a day for 20 years. 4
 is characterized by airflow")
COPD – Introduction and Definitions Chronic obstructive pulmonary disease (COPD) is characterized by airflow obstruction. The airflow obstruction is usually: progressive, not fully reversible does not change markedly over several months. associated with an abnormal inflammatory response of the lung to noxious particles or gases. The disease is predominantly caused by smoking. COPD is a preventable and treatable disease with some significant extrapulmonary effects that may contribute to the severity in individual patients. The most common conditions comprising COPD are chronic bronchitis and emphysema.

Epidemiology COPD prevalence, morbidity, and mortality vary across countries and across different groups within countries. COPD is projected to be the Fourth leading cause of death and the fifth leading cause of morbidity worldwide by 2030. COPD includes chronic bronchitis, emphysema, or a combination of these conditions but does not include conditions in which airflow limitation is the differential diagnosis (e. g. , asthma, bronchiectasis, and cystic fibrosis).

Prevalence of asthma and COPD in the United States 2006

Etiology and Risk Factors � Multiple pathogenetic mechanisms likely contribute to the development of COPD. � The most important risk factor is cigarette smoking, which can affect the lungs by a variety of mechanisms. � Age of starting, total pack-years, and current smoking status are predictive of COPD mortality. � Children and spouses of smokers are also at increased risk of developing significant pulmonary dysfunction by passive smoking, � Other exposures also contribute, probably through similar pathways. � Both genetic and acquired conditions, also play a role and likely account for much of the variable susceptibility of individuals to the effects of cigarette smoke and other exposures. � Other risk factors for COPD include; lung growth, airway hyperresponsiveness, asthma, environmental and occupational exposures [e. g. , grain, coal, asbestos], indoor and outdoors air pollution, and respiratory infections.

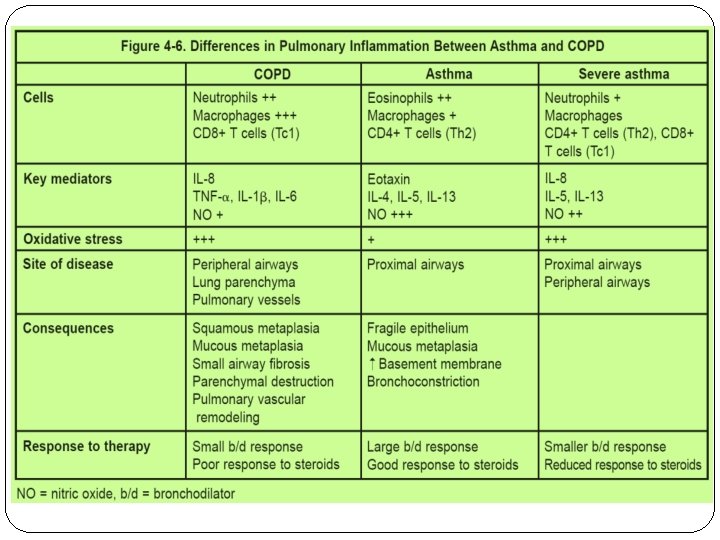
Pathophysiology emphasis is currently placed on the pathophysiologic features of small airways disease and parenchymal destruction as contributors to chronic airflow limitation. Most patients with COPD demonstrate features of both problems. The underlying problem is persistent exposure to noxious particles or gases that sustain the inflammatory response. The airways of the lung and the parenchyma are both susceptible to inflammation and the result is chronic airflow limitation that characterizes COPD

Clinical Presentation

Global Strategy for Diagnosis, Management and Prevention of COPD Symptoms of COPD The characteristic symptoms of COPD are chronic and progressive dyspnea, cough, and sputum production that can be variable from day-to-day. Dyspnea: Progressive, persistent and characteristically worse with exercise. Chronic cough: May be intermittent and may be unproductive. Chronic sputum production: COPD patients commonly cough up sputum. © 2013 Global Initiative for Chronic Obstructive Lung Disease

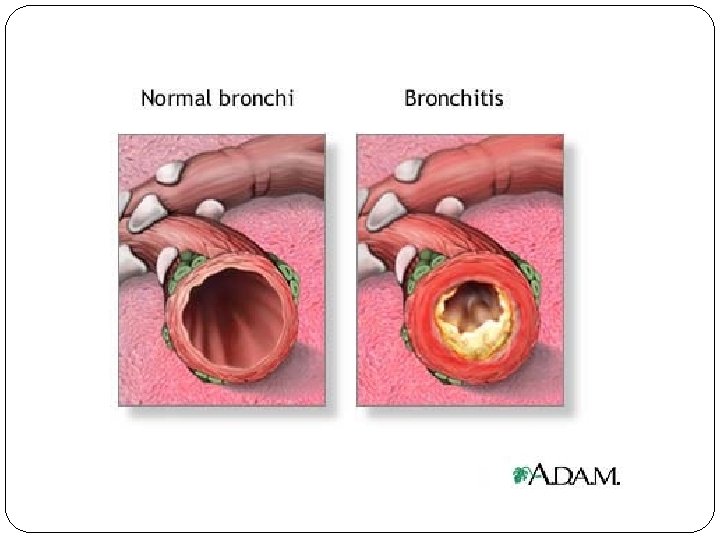
Chronic Bronchitis Chronic bronchitis presents clinically as: chronic excessive mucus production and secretion resulting in airflow obstruction secondary to inflammation and edema. Persistent productive cough is present on most days for three months or more during the year over at least twoincreased consecutive The mucusyears. is an excellent media for recurrent bronchial infections resulting in further damage. Repeated infections result because of inability to clear the mucus and mucous plugs.

cor pulmonale Chronic hypoxia Pulmonary vasoconstriction Muscularization Pulmonary hypertension Intimal hyperplasia Cor pulmonale Fibrosis Obliteration Edema Death

Emphysema results from anatomical defects of the lung characterized by abnormal permanent enlargement of the air spaces distal to the terminal bronchiole, accompanied by destruction of alveolar walls, but without obvious Destruction of alveolar tissue results in loss of elastic recoil and fibrosis. structural support; thus, obstruction and airway collapse occurs during expiration. Commonly, associated with a history of cigarette smoking and typically occurs after age 60. Rarely, associated with α 1 -antitrypsin enzyme deficiency caused by a genetic defect in the production of the α 1 antitrypsin enzyme, which normally is protective to the alveolar lining of the lung. α 1 antitrypsin

Chronic obstructive pulmonary disease Interrelationship of chronic bronchitis and emphysema Normal Chronic bronchitis Emphysema Mixed (in variable degree) 24 © Novartis

COPD diagnosis

Spirometry: Normal and Patients with COPD Spirometry should be performed after the administration of an adequate dose of a shortacting inhaled bronchodilator to minimize variability. A post-bronchodilator FEV 1/FVC < 0. 70 confirms the presence of airflow limitation that is not fully reversible. Where possible, values should be compared to age -related normal values to avoid overdiagnosis of COPD in the elderly

Management of COPD

Goals of Therapy Prevent disease progression Relieve symptoms Improve exercise tolerance Improve overall health status Prevent and treat exacerbation Prevent and treat complications Reduce morbidity and mortality

Four Components of COPD Management 1. Assess and monitor disease 2. Reduce risk factors 3. Manage stable COPD � Education � Pharmacologic � Non-pharmacologic 4. Manage exacerbations

Global Strategy for Diagnosis, Management and Prevention of COPD Assessment of COPD §Assess degree of airflow limitation using spirometry §Assess symptoms §Assess risk of exacerbations §Assess comorbidities © 2013 Global Initiative for Chronic Obstructive Lung Disease

Classification of COPD Severity by Spirometry The hallmark of obstructive disease is a decrease in the forced expiratory volume in one second (FEV 1), and the ratio of FEV 1 to the forced vital capacity (FVC) is <75%.


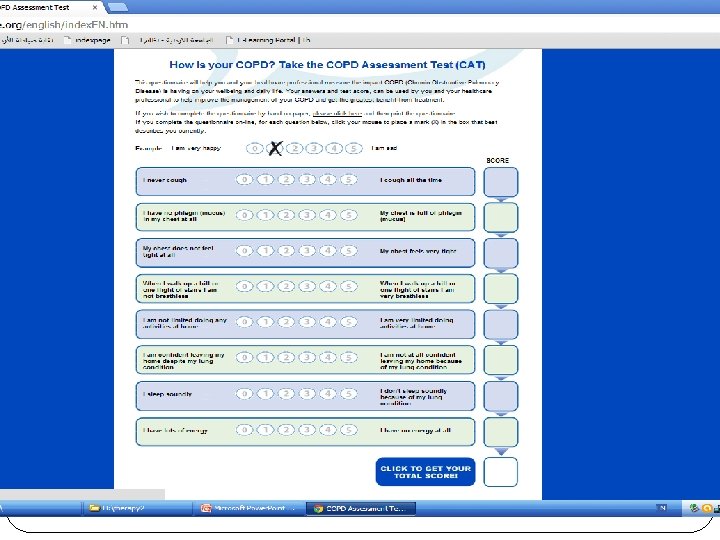
COPD Assessment Test

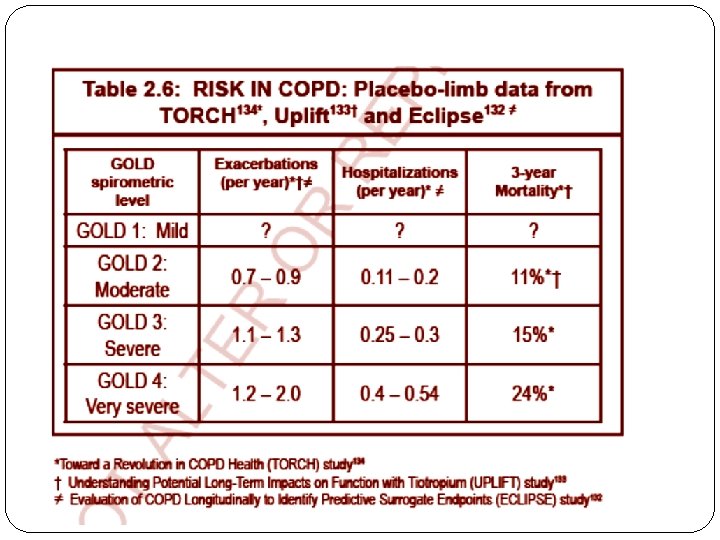
GOLD 2014 Update – Risk Assessment There are three methods of assessing exacerbation risk. Ø One is a population-based method using the GOLD spirometric classification (Table 2. 5), with GOLD 3 or GOLD 4 categories indicating high risk. Ø The second based on the individual patient’s history of exacerbations with two or more exacerbations in the preceding year indicating high risk. Ø The third is a history of hospitalization due to an exacerbation in the preceding year. (If there is a discrepancy between these criteria, the assessment pointing to the highest risk should be

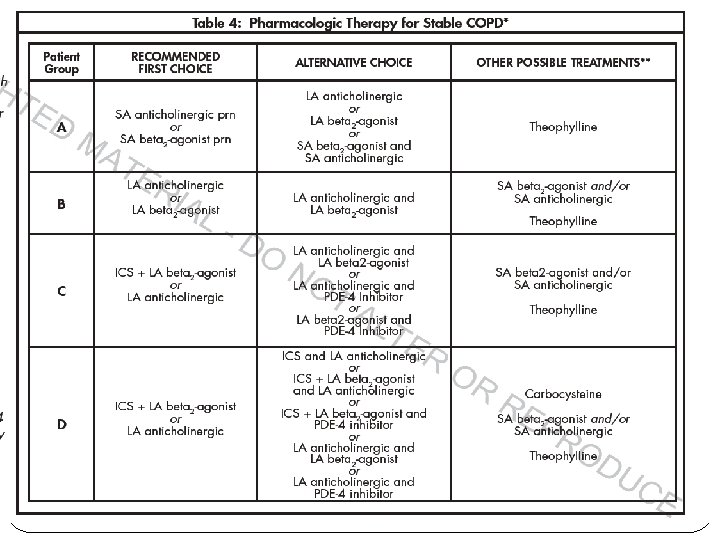
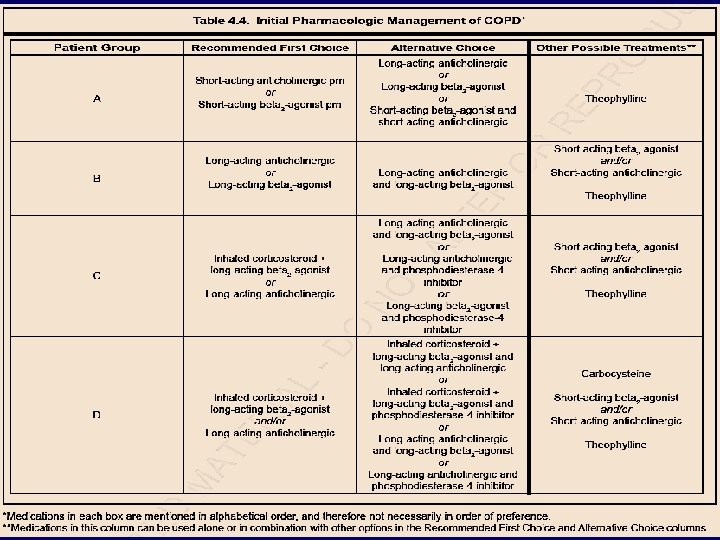
The groups can be summarized as follows: • Patient Group A – Low Risk, Less Symptoms Typically GOLD 1 or GOLD 2 (Mild or Moderate airflow limitation) and/or 0 -1 exacerbation per year and m. MRC grade 0 -1 or CAT score < 10 • Patient Group B – Low Risk, More Symptoms Typically GOLD 1 or GOLD 2 (Mild or Moderate airflow limitation) and/or 0 -1 exacerbation per year and m. MRC grade ≥ 2 or CAT score ≥ 10 • Patient Group C – High Risk, Less Symptoms Typically GOLD 3 or GOLD 4 (Severe or Very Severe airflow limitation) and/or ≥ 2 exacerbations per year and m. MRC grade 0 -1 or CAT score < 10 • Patient Group D – High Risk, More Symptoms Typically GOLD 3 or GOLD 4 (Severe or Very Severe airflow limitation) and/or ≥ 2 exacerbations per year and m. MRC grade ≥ 2

Patient Categories in COPD to Determine the Severity of the Disease using GOLD Airflow Limitation Grades, Exacerbations and Level of Symptoms

Global Strategy for Diagnosis, Management and Prevention of COPD Manage Stable COPD: Non-pharmacologic Patient Group Essential A Smoking cessation (can include pharmacologic treatment) B, C, D Smoking cessation (can include pharmacologic treatment) Pulmonary rehabilitation Recommended Depending on local guidelines Physical activity Flu vaccination Pneumococcal vaccination © 2013 Global Initiative for Chronic Obstructive Lung Disease

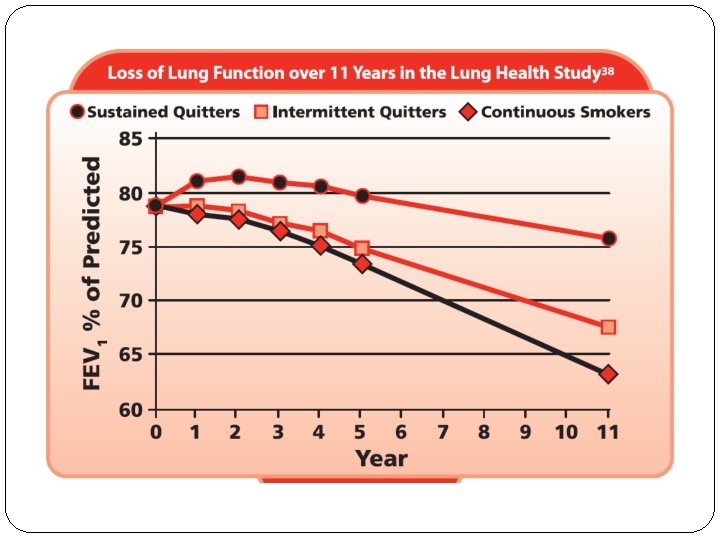
Reduce Risk Factors: Key Points Reduction of total personal exposure to tobacco smoke, occupational dusts and chemicals, and indoor and outdoor air pollutants are important goals to prevent the onset and progression of COPD. Smoking cessation is the single most effective — and cost effective — intervention in most people to reduce the risk of developing COPD and stop its progression (Evidence A). Counseling delivered by physicians and other health professionals significantly increases quit rates over selfinitiated strategies. Even a brief (3 -minute) period of counseling to urge a smoker to quit results in smoking cessation rates of 5 -10%. Numerous effective pharmacotherapies for smoking cessation are available and pharmacotherapy is recommended when counseling is not sufficient to help
,")
Anticholinergics Tiotropium reduces exacerbations and related hospitalizations, improves symptoms and health status (Evidence A), and improves the effectiveness of pulmonary rehabilitation (Evidence B). In a large, longterm clinical trial on patients with COPD, there was no effect of tiotropium added to other standard therapies on the rate of lung function decline and no evidence of cardiovascular risk. In another large trial, tiotropium was superior to salmeterol in reducing exacerbations although the difference was small. The long-acting anticholinergics aclidinium and glycopyrronium seem to have similar action on lung function and breathlessness as tiotropium, whereas far

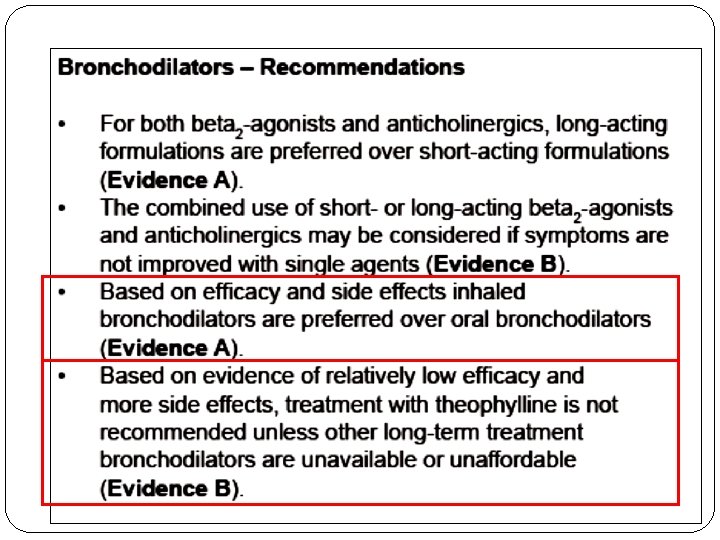
Long-acting β-agonists compared to other bronchodilators � They are also useful to reduce nocturnal symptoms and improve quality of life. � When compared to short-acting bronchodilators or theophylline, both salmeterol and formoterol: �improve lung function, symptoms, exacerbation frequency and quality of life. �These benefits are apparent even in patients with poorly reversible lung function and are related to improvements in inspiratory capacity. � Both salmeterol and formoterol have been compared to ipratropium. In separate studies, each agent improved FEV 1 compared to ipratropium and, in addition, the longacting bronchodilator was more effective for other selected outcomes (e. g. , prolonged time to exacerbation for

Other Pharmacologic Therapies Antioxidant agents. Antioxidants, in particular N- acetylcysteine, have been reported in small studies to reduce the frequency of exacerbations, leading to speculation that these medications could have a role in the treatment of patients with recurrent exacerbations (Evidence B). However, a large randomized controlled trial found no effect of N-acetylcysteine on the frequency of exacerbations, except in patients not treated with inhaled glucocorticosteroids.
 and Antioxidant Agents (ambroxol, erdosteine, carbocysteine, iodinated glycerol). The regular")
Mucolytic (mucokinetic, mucoregulator) and Antioxidant Agents (ambroxol, erdosteine, carbocysteine, iodinated glycerol). The regular use of mucolytics in COPD has been evaluated in a number of long-term studies with controversial results. Although a few patients with viscous sputum may benefit from mucolytics, the overall benefits seem to be very small; the widespread use of these agents cannot be recommended at present.

Nedocromil and leukotriene modifiers. These have not been adequately tested in COPD patients and cannot be recommended. There was no evidence of benefit -and some evidence of harm (malignancy and pneumonia)- from an anti-TNF-alpha antibody (infliximab) tested in moderate to severe COPD. Use of endothelin-receptor antagonist bosentan fails to improve exercise capacity and may increase hypoxemia; it should not be used to treat patients with severe COPD

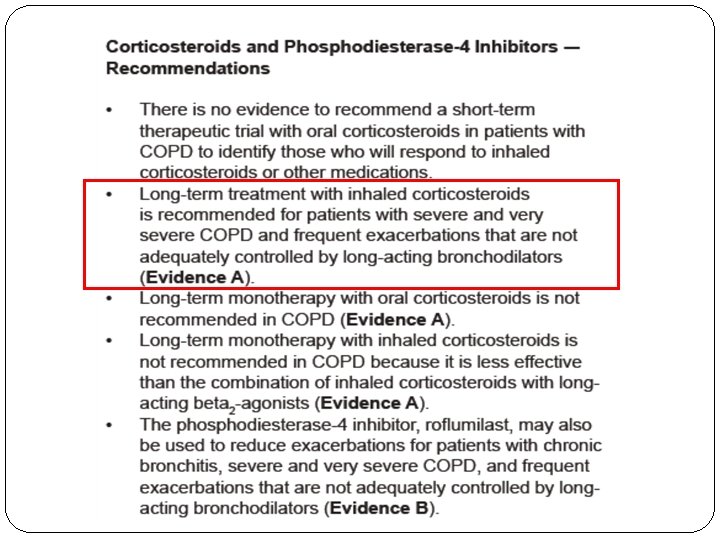
The phosphodiesterase-4 inhibitor roflumilast has been approved for use only in some countries (FDA approved in 2011, brand names Daliresp, Daxas). It is a once daily oral medication with no direct bronchodilator activity, although it has been shown to improve FEV 1 in patients treated with salmeterol or tiotropium. Roflumilast reduces moderate and severe exacerbations treated with corticosteroids by 1520% in patients with chronic bronchitis, severe to very severe COPD, and a history of exacerbations(Evidence A). The effects on lung function are also seen when roflumilast is added to long-acting bronchodilators (Evidence A), whereas the effects on patient-related outcomes and particularly exacerbations remain controversial. There are no comparison or add-on studies of roflumilast and inhaled corticosteroids.

COPD Exacerbations

Acute COPD Exacerbations � Common symptoms include: � increased shortness of breath � an increase in the amount and purulence of sputum. � Hypoxemia and hypercapnia may also be present. � With an exacerbation, patients using rapid-acting bronchodilators may report an increase in the frequency of use. � Exacerbations are commonly staged as mild, moderate, or severe according to the criteria summarized in the Table Mild (type 1) One cardinal symptom plus at least one of the following: URTI within 5 days, fever without other explanation, increased wheezing, increased cough, increase in respiratory or heart rate >20% above baseline Moderate (type 2) Two cardinal symptoms Severe (type 3) Three cardinal symptoms Cardinal symptoms include worsening of dyspnea, increase in sputum volume, and increase in sputum purulence.

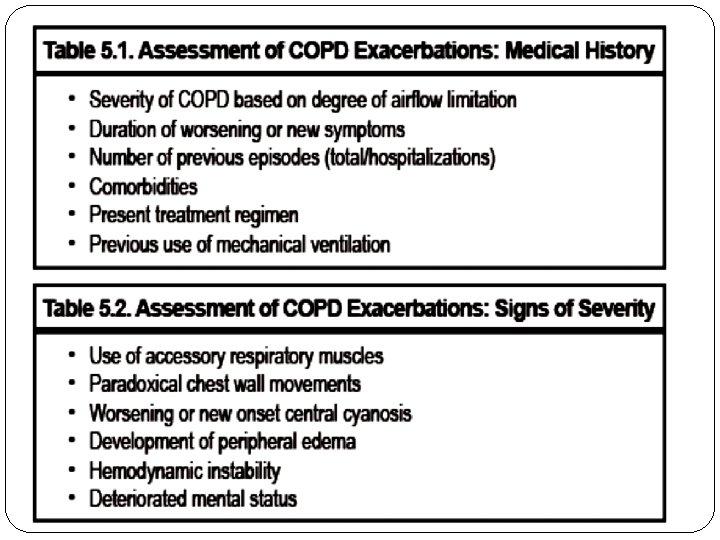
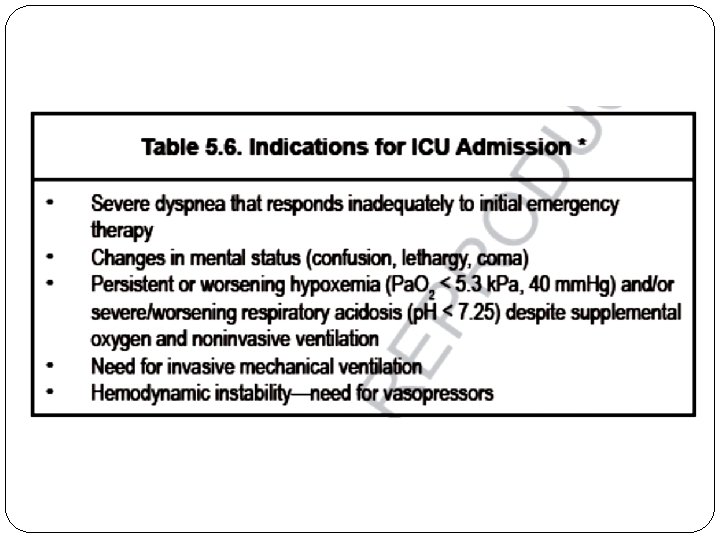
An important complication of a severe exacerbation is acute respiratory failure. In the emergency department or hospital, an ABG usually is obtained to assess the severity of an exacerbation. The diagnosis of acute respiratory failure in COPD is made on the basis of an acute change in the ABGs. Defining acute respiratory failure as a Pa. O 2 of less than 50 mm Hg or a Pa. CO 2 of greater than 50 mm Hg often may be incorrect and inadequate because these values may not represent a significant change from a patient's baseline values. A more precise definition is an acute drop in Pa. O 2 of 10 to 15 mm Hg or any acute increase in Pa. CO 2 that decreases the serum p. H to 7. 3 or less. Additional acute clinical manifestations of

Global Strategy for Diagnosis, Management and Prevention of COPD Manage Exacerbations: Assessments Arterial blood gas measurements (in hospital): Pa. O 2 < 8. 0 k. Pa with or without Pa. CO 2 > 6. 7 k. Pa when breathing room air indicates respiratory failure. Chest radiographs: useful to exclude alternative diagnoses. ECG: may aid in the diagnosis of coexisting cardiac problems. Whole blood count: identify polycythemia, anemia or bleeding. Purulent sputum during an exacerbation: indication to begin empirical antibiotic treatment. Biochemical tests: detect electrolyte disturbances, diabetes, and poor nutrition. Spirometric tests: not recommended during an exacerbation. © 2013 Global Initiative for Chronic Obstructive Lung Disease

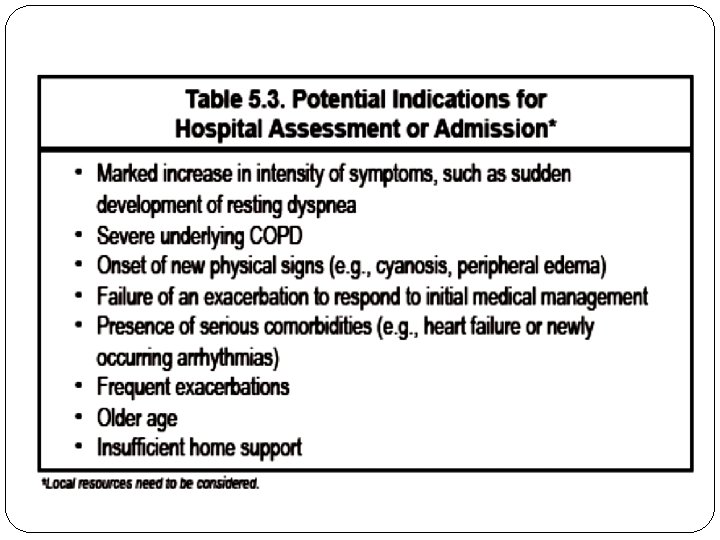
Goals of Therapy The goals of therapy for patients experiencing exacerbations of COPD: prevention of hospitalization or reduction in hospital stay, prevention of acute respiratory failure and death, resolution of exacerbation symptoms and a return to baseline clinical status and quality of life.
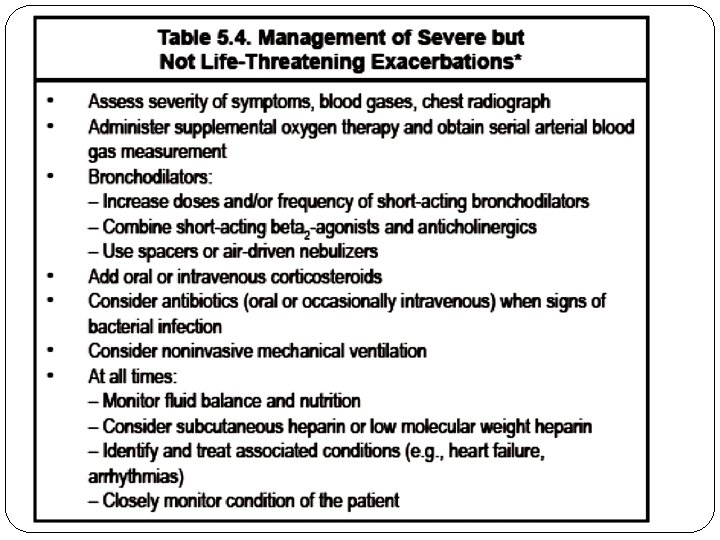

Treatment of Acute COPD Exacerbations Therapy Comments Antibiotics Recommended if two or more of the following are present: Increased dyspnea Increased sputum production Increased sputum purulence Corticosteroids Oral or intravenous therapy may be used. If intravenous is used, it should be changed to oral after improvement in pulmonary status. If continued longer than 14 days, then the dose should be tapered to avoid hypothalamic–pituitary–adrenal axis suppression. Bronchodilator Metered-dose inhalers and dry-powder inhalers equal in efficacy to s nebulization. β-Agonists also may increase mucociliary clearance. Long-acting β-agonists should not be used for quick relief of symptoms or on an as-needed basis. Controlled Titrate oxygen to desired oxygen saturation (>90%). oxygen therapy Monitor arterial blood gas for development of hypercapnia. Noninvasive mechanical Consider for patients with acute respiratory failure. Not appropriate for patients with altered mental status, severe

Global Strategy for Diagnosis, Management and Prevention of COPD Manage Exacerbations: Key Points § Short-acting inhaled beta 2 -agonists with or without short-acting anticholinergics are usually the preferred bronchodilators for treatment of an exacerbation. § Systemic corticosteroids and antibiotics can shorten recovery time, improve lung function (FEV 1) and arterial hypoxemia (Pa. O 2), and reduce the risk of early relapse, treatment failure, and length of hospital stay. § COPD exacerbations can often be prevented. © 2013 Global Initiative for Chronic Obstructive Lung Disease

Rothberg, et al. completed a retrospective cohort study of 84, 621 patients hospitalized for acute exacerbations of COPD at 413 acute care facilities throughout the U. S. The study objective was to compare outcomes of patients treated with antibiotics in the first 2 days of hospitalization with those treated later or not at all. The main outcome measure was a composite of treatment failure (defined as the initiation of mechanical ventilation after the second hospital day), inpatient mortality, or readmission for acute COPD exacerbations within 30 days of discharge as well as length of stay and hospital costs. The authors conclude that early antibiotic administration was associated with improved outcomes among patients hospitalized for acute exacerbations of COPD regardless of the risk of

A systematic review of the very few available placebo- controlled studies has shown that antibiotics reduce the risk of short-term mortality by 77%, treatment failure by 53% and sputum purulence by. 44% The choice of the antibiotic should be based on the local bacterial resistance pattern. Usually initial empirical treatment is an aminopenicillin with or without clavulanic acid, macrolide, or tetracycline. In patients with frequent exacerbations, severe airflow limitation and/or exacerbations requiring mechanical ventilation, cultures from sputum or other materials from the lung should be performed, as gram-negative bacteria (e. g. , Pseudomonas species) or resistant pathogens that are not sensitive to the above-

Global Strategy for Diagnosis, Management and Prevention of COPD Manage Exacerbations: Treatment Options Antibiotics should be given to patients with: § Three cardinal symptoms: increased dyspnea, increased sputum volume, and increased sputum purulence. § Sputum purulence an one other cardinal symptom § Who require mechanical ventilation. © 2013 Global Initiative for Chronic Obstructive Lung Disease

115

116

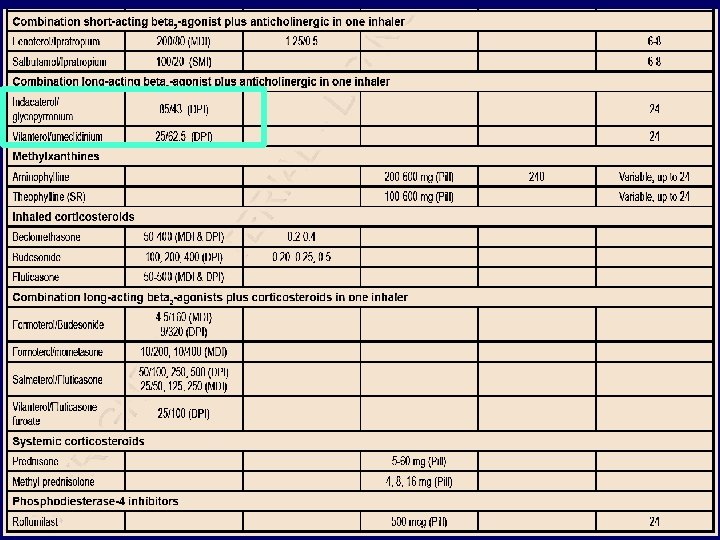
PHARMACOLOGIC THERAPIES
- Slides: 62