Chronic lymphocytic leukemia HANAN A ELTIB 2014 OVERVIEW

Chronic lymphocytic leukemia HANAN. A. ELTIB 2014

OVERVIEW � The most prevalent type of adult leukemia in western countries � Median age of diagnosis of CLL is ~ 72 years, with only 10% of patients younger than 50 years of age � CLL morbidity rapidly increases with age � More common in men than women (2: 1 ratio)

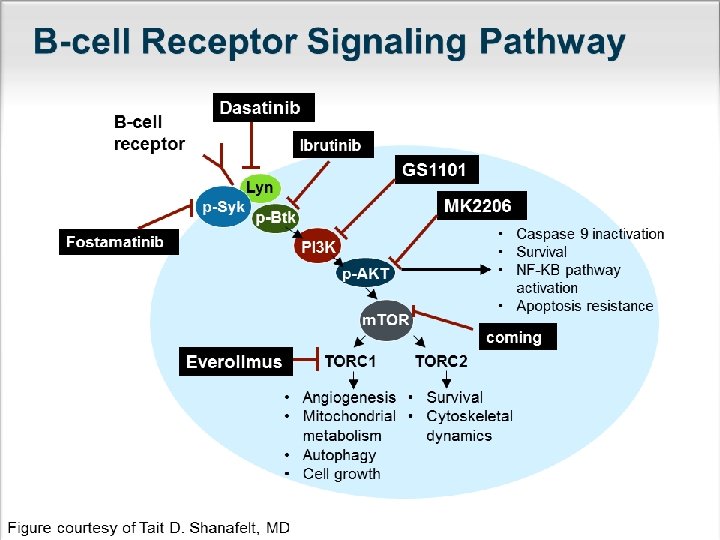
hophysiology �Historically CLL considered disease of accumulation due to defect in apoptosis �CLL more proliferative disease than previously thought �CLL cells up regulate gene signature consistent with BCR and NF-KB pathway activation

Diagnosis �CBC: at least 5000 monoclonal B-lymphocytes/cml in the peripheral blood �Morphologically : small mature lymphocytes �N. B : Fewer clonal B-Cells LNS less 1. 5 cm no anemia or thromocytopenia +/_ the immunophenotybe of the CLL ALymphoproliferative disorders : monoclonal Blymphocytosis(MPL)

CLL/SLL Different manifestation of the same disease managed in the same way �The major difference SLL: the abnormal lymphocytes are predominantly found in the LNS-diagnosis mainly by LN biopsy-no more than 5000 clonal B-cells in the peripheral blood CLL: significant number of the abnormal lymphocytes are also found in the BM and blood §

Initial Work-up of CLL Patients Flow cytometry of the peripheral blood � Kappa/lambda � CD 5 + � CD 19 + � CD 23 + � CD 10 � CD 20 dim � Surface IG dim � Cycline D 1 – � Atypical CLL : t(11; 14) by FISH : LN biopsy with IHC CD 3 CD 5 CD 10 CD 23 Cyclin D 1

Initial Work-up of CLL Patients � Anemic pt : RC count - direct combs‘ test � LN biopsy only if diagnosis not confirmed by flowcytometry � Bone marrow aspirate and biobsy not necessary in absence of cytopenias � No CT scan unless symptoms are present; PET scan be helpful if Richter’s suspected � Informative for prognostic and/or therapy determination flowcytometry or IHC: cytogenetics analysis : mollecular analysis : serum level : CD 38 -CD 70 +12, del(13 q), del(17 p)and del(11 q) IGVH gene status assessment-TP 53 β 2 -microglobulin

Initial Work-up of CLL Patients � Physical Exam LNs : size-symptoms liver-spleen size � B-symptoms � Performance � Useful under certain circumstaces Ø haptoglobin Ø Serum QIG level Ø uric acid Ø LDH Ø HBV

RAI’s CLINICAL STAGING SYSTEM Stage 0 Low risk Clinical Features at Diagnosis Blood lymphocytosis>5000/mcl, Bone marrow lymphocytosis>30% Median Survival (years) >12, 5 I Intermediate risk Stage 0 and enlarged lymph node(s) 8 II Intermediate risk Stage 0 -I and enlarged spleen and/or liver 6 III High risk Stage 0 -II and anemia (Hb < 11 g/dl) 1, 5 -2 IV High risk Stage 0 -III and thrombocytopenia(< 100 000 /mcl) 1, 5 -2

When to Treat CLL Patient No advantage to treating CLL until symptoms develop § Constitutional symptoms due to disease (fatigue, B symptoms) § Enlarging, symptomatic lymph nodes (> 10 cm) § Enlarging, symptomatic spleen (> 6 cm BCM) §Cytopenias due to CLL (hemoglobin < 11 g/d. L, platelets < 100, 000 cells/μL) § Poorly controlled AIHA or ITP §Absolute lymphocytic count alone is not indication for treatment unless above 200 -300× 109/L Or symptoms related to leukostasis

Treatment options ØAlkylating agents ØPurine anologue vs Alkylators Higher RR and PFS Better QOL Not OS ØPurine/alkylator combo vs. purine: Higher RR and PFS Not OS

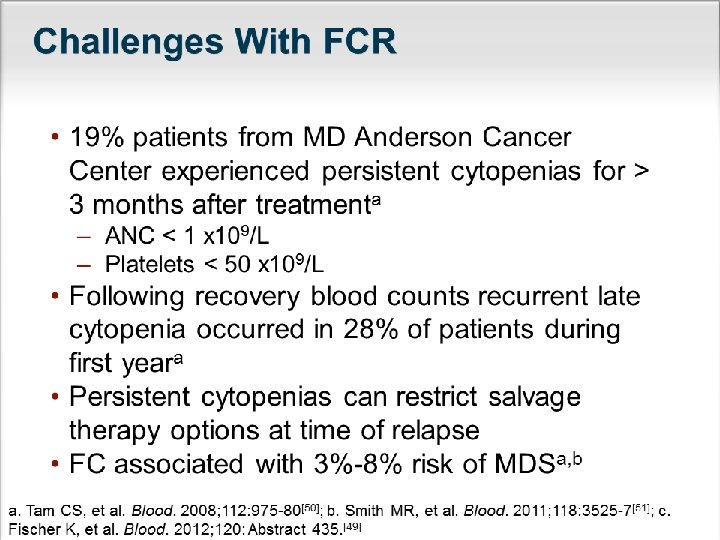
Treatment options Ø CLL 8 study ; chemoimmunotherpy : FCR VS FC • More neutropenia • A better therapy for young –physically fit pt • Significantly improves ORR and CR • Significantly improves PFS • Significantly improves OS 7% Most genetic groups benefit from FCR therapy except for del(17 p 13)

Treatment options CLL 10 study; FCR VS BR Ø Bendamastin: An Alkylator agent with apurine like benzimidazole ring component Ø Identical ORR Ø Higher CR rates observed with FCR ØPFS significantly longer with FCR ØAcute (and long-term? ) toxicity greater with BR PCR Ø Pentostatin: purine analog Ø No advantage over FCR Ø Cyclophoshamide is an important component Alemtuzumab ØHuminazied Monoclonal Ab target CD 52 ØNot as afirst line treatment option except in the setting of del (17 p)

Treatment options : In elderly �FCR not well tolerated –less effective by pts 70 ys �Fludrabine vs chloreambucil 65 ys Better ORR CR TTTF QOL analysis favoured fludrabine NO PFS OS difference SO Chloreambucil is avalid option

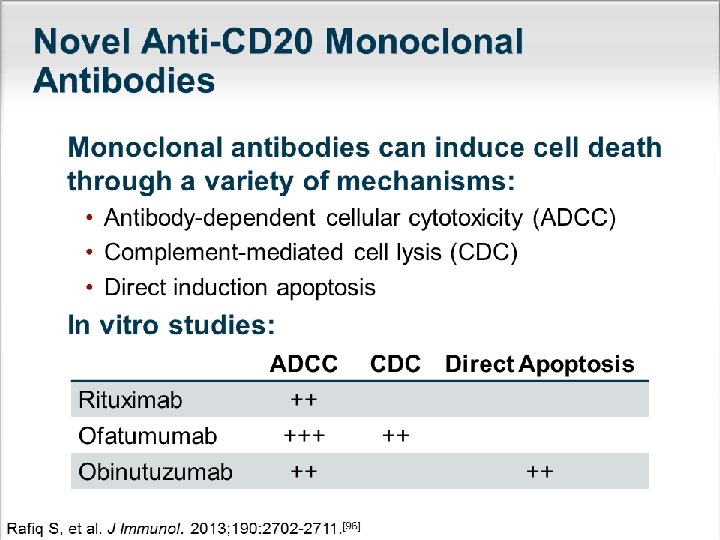
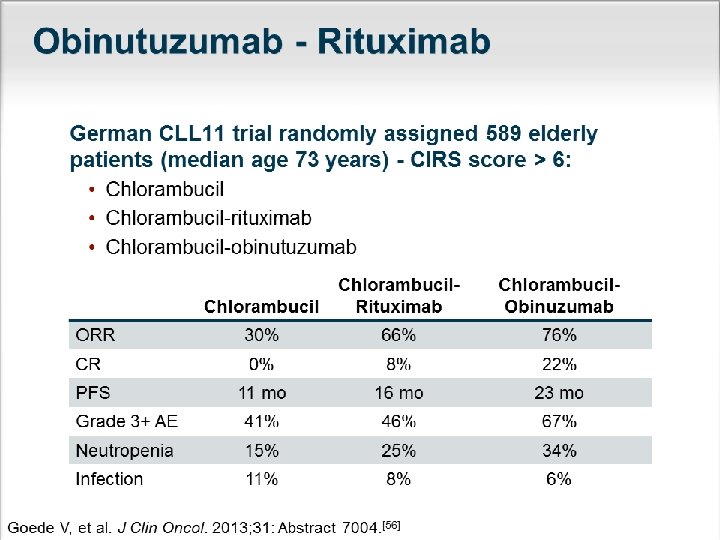
Treatment options : In elderly �Bendamastin vs chlorambucil Higher RR/PFS Higher toxicity � CLL 11 study : Obinituzumab + chlorambucil is an effective, well-tolerated therapy Most appropriate for elderly ? question of whether obinituzumab is superior to rituximab in other clinical contexts

First line therapy �Fit patient Chemoimmunotherapy e. g FCR/FR/BR/PCR �Elderly pt-comorbidity Chlorambucil+/- R Fludarabine+/- R Cyclophosphamide , prednisolone+/-R Bendamastin+/-R Rituximab

First line therapy �Frail pt Chlorambucil Pulse steroides Rituximab
 Trial Ø FCR Ø HDM+R Ø Alemtuzumab+/-R")
Molecular guided therapy �Pt with del(17 p) Trial Ø FCR Ø HDM+R Ø Alemtuzumab+/-R Ø Ibrutinib for patients with relapsed/refractory disease § Pt with del(11 q) Ø Regimens containing an alkylator Ø

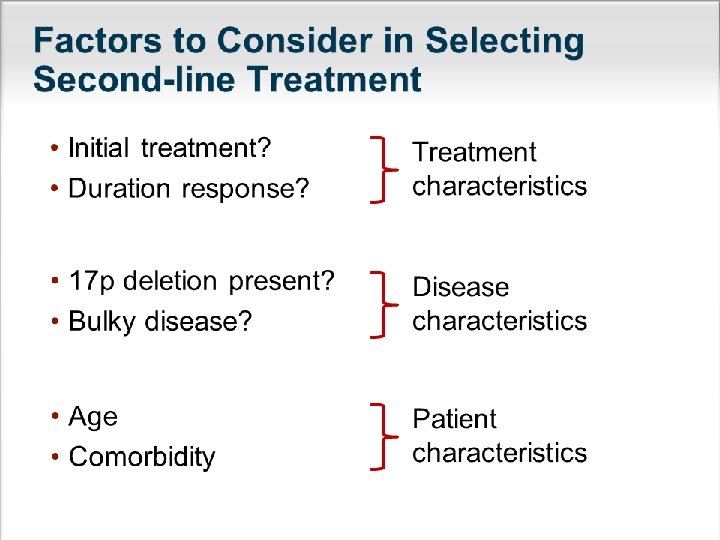
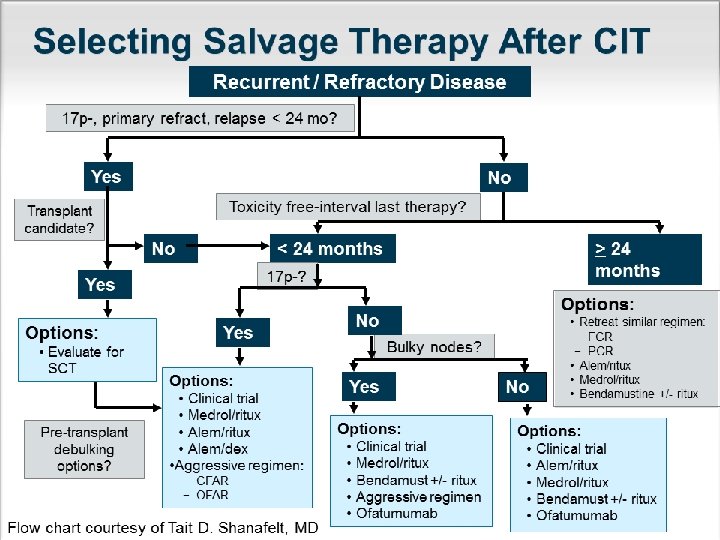
Considerations for Relapsed CLL � Outcome of patients at time of relapse dependent on: – Interphase cytogenetics, β 2 -microglobulin, and stage – Previous therapy (ie, monotherapy or chemoimmunotherapy) – Time of remission with last treatment � Treat relapsed patients when symptomatic only � Interphase cytogenetics should be repeated prior to initiating salvage therapy � All patients with cytopenias should have repeat bone marrow to assess for MDS if prior FCR given � Transplant evaluation should be considered early in this population if any unfavorable features present

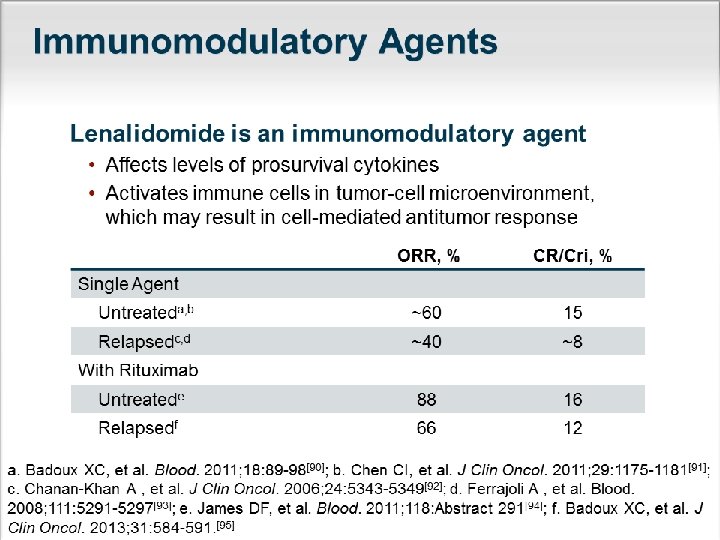
Salvage therapy �Ibrutinib �Chemoimmunotherapy �Ofatumab �Lenalidomide+/- R �Alemtuzumab+/- R

Supportive Care for pts with CLL � 1 -Recurrent infection Antimicrobials as appropriate IVIG, if <500 mg/dl � 2 -Antinfective prophylaxis PCP-Herpes virus CMV HBV � 3 -vaccination Annual INFLUENZA vaccine Pneumococcal vaccine/5 y

Supportive Care for pts with CLL �Blood product : irradiate all blood product �Tumor lysis syndrome �Tumor flare reaction : lenalidomide �Thromboprophylaxis : lenalidomide �Autoimmune cytopenias - Steroides - IVIG - Cyclosporin A - Rituximab - Splenectomy
 �Constitutional symptoms �Physical Examination Organomegally LNS �Blood parameters blood")
Follow up (In clinical practice) �Constitutional symptoms �Physical Examination Organomegally LNS �Blood parameters blood counts �+/_BM
 �DLBCL or HL � 2 -5 % �Increase with NO. of")
Histological Transformation(Richter's syndrome) �DLBCL or HL � 2 -5 % �Increase with NO. of prior regimens �Poor prognosis �Extra nodal involvement, Sharp rise in LDH �Chemoimmunotherapy e. g R-CHOP/ R-HYPERCYVAD � Allogeneic HSCT, considered following initial therapy �Prolymphoctic leukemia. > 55% increase in prolymphocytes Progression of splenomegaly & cytopenias Refractoriness to treatment.
- Slides: 36