Chronic Kidney Disease Brandon Mickelsen DO Director ISU

Chronic Kidney Disease Brandon Mickelsen DO Director ISU FM Residency

Quiz Kahoot. it

Main Sources NKF: National kidney foundation NICE: National institute for clinical excellence
 Define 2) Identify what is for us 3) Monitoring 4)Treatment of")
Game Plan 1) Define 2) Identify what is for us 3) Monitoring 4)Treatment of complications

Problem About 12% of Americans Significantly increased mortality as progresses n 9 th leading cause of death in America Tripled since 1990 72% from HTN or DM 2012 29 Billion in Medicare spending

Kahoot 1, 2, 3, 4

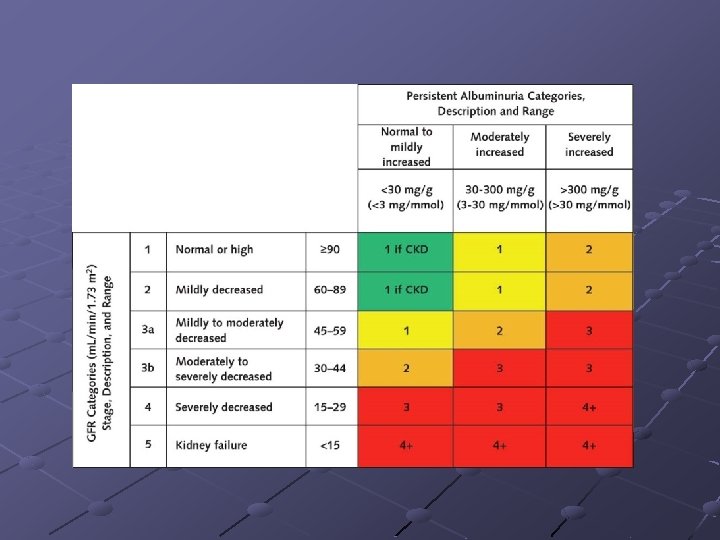
Diagnosis CKD is defined as abnormalities of kidney structure or function, present for >3 months, with implications for health and CKD is classified based on cause, GFR category, and albuminuria category (CGA). (NKF)

GFR Do I rely on the lab print out? Which Formula to I use?

Name that GFR 90 yo white female 120 pounds creatinine 0. 9 what is her GFR n Cockcroft-Gault 35. 7 CKD-EPI 56. 3 55 yo black male 280 pounds Creatinine 1. 9 what is his GFR n Cockcroft-Gault 79 CKD-EPI 45

Name that GFR 75 yo black female 150 pounds creatinine 1. 2 what is her GFR n Cockcroft-Gault 44 CKD-EPI 51 30 yo white male 220 pounds creatinine 2. 9 what is his GFR Cockcroft-Gault 52 CKD-EPI 32

CKD-EPI “The best way to determine drug dosing is with the CKD-EPI Creatinine Equation (2009) or the MDRD Study. Both have been shown to be more accurate than the CG formula. ” NKF NICE recommends CKD-EPI as well.

Adaptations Be aware that GFR will be overestimated in people with significant muscle mass

When to refer ACR above 70 mg/mmol unless from diabetes Proteinuria combined with hematuria Rapid progression Young age Known/suspected genetic cause Renal artery stenosis

CKD 3 for Primary care Focus on CKD G 3 a/b. A 1/2 n This is what we mostly see and what WE should be managing

AGE

Age In people aged over 70 years, an e. GFR in the range 45– 59 ml/min/1. 73 m 2, if stable over time and without any other evidence of kidney damage, is unlikely to be associated with CKD-related complications. (NICE)

Monitoring How often do I check labs? Which labs? What about imaging?

Monitoring NKF n CKD 3 yearly CBC PTH and Phosphorus at least once Nice n n Obtain baseline cbc in all pts with GFR less than 45, and treat and monitor based upon results Don’t order calcium, PTH, and vitamin in pts with GFR above 30, but do test if less than 30. Frequency of testing is based upon results.

proteinuria All people with diabetes, and people without diabetes with a GFR less than 60 ml/min/1. 73 m 2, should have their urinary albumin/protein excretion quantified. The first abnormal result should be confirmed on an early morning sample (if not previously obtained). (NICE)

Proteinuria NKF

Quiz Kahoot 5, 6, 7
 1. 4. 1 Offer a renal ultrasound")
Renal Ultrasound Indications for renal ultrasound (NICE) 1. 4. 1 Offer a renal ultrasound to all people with CKD who: n n n have progressive CKD have visible or persistent invisible hematuria have symptoms of urinary tract obstruction have a family history of polycystic kidney disease and are aged over 20 have stage 4 or 5 CKD are considered by a nephrologist to require a renal biopsy. NKF (Most pts with CKD): to evaluate for kidney shape, size, symmetry and evidence of obstruction

Treatment CKD 3 often carries minor complications that can and should usually be managed by us
 n n keep the systolic blood pressure below 140 mm.")
Blood pressure control (NICE) n n keep the systolic blood pressure below 140 mm. Hg (target range 120– 139 mm. Hg) and the diastolic blood pressure below 90 mm. Hg. In people with CKD and diabetes, and also in people with an ACR of 70 mg/mmol or more, aim to keep the systolic blood pressure below 130 mm. Hg (target range 120– 129 mm. Hg) and the diastolic blood pressure below 80 mm. Hg.
 We recommend that in both diabetic and non-diabetic adults with CKD")
Blood pressure (NKF) We recommend that in both diabetic and non-diabetic adults with CKD and urine albumin excretion <30 mg/ 24 hours (or equivalent*) whose office BP is consistently >140 mm Hg systolic or >90 mm Hg diastolic be treated with BP-lowering drugs to maintain a BP that is consistently <140 mm Hg systolic and <90 mm Hg diastolic. (1 B) We suggest that in both diabetic and non-diabetic adults with CKD and with urine albumin excretion of >30 mg/24 hours (or equivalent*) whose office BP is consistently >130 mm Hg systolic or >80 mm Hg diastolic be treated with BP-lowering drugs to maintain a BP that is consistently <130 mm Hg systolic and <80 mm Hg diastolic. (2 D) We suggest that an ARB or ACE-I be used in diabetic adults with CKD and urine albumin excretion 30– 300 mg/ 24 hours (or equivalent*). (2 D) We recommend that an ARB or ACE-I be used in both diabetic and nondiabetic adults with CKD and urine albumin excretion >300 mg/24 hours (or equivalent*). (1 B)
 DM and ACR more than 2. 5 mg/mmol (men) or more than")
ACEI/ARB (NICE) DM and ACR more than 2. 5 mg/mmol (men) or more than 3. 5 mg/mmol (women) irrespective of the presence of hypertension or CKD stage. non-diabetic people with CKD and hypertension and ACR 30 mg/mmol or more Offer ACE inhibitors/ARBs to non-diabetic people with CKD and ACR 70 mg/mmol or more irrespective of the presence of hypertension or cardiovascular disease n (Cochrane 2011 insufficient evidence to support acei in non diabetic ckd ) Titrate to maximal tolerated dose before adding another agent No evidence that treating diabetes with no proteinuria is needed

ACEI Cochrane 2011 no evidence to support ACEI/ARB in ckd 3 w/o diabetes. Kahoot 8, 9, 10

Worse on an ACEI? If there is a fall in e. GFR or rise in plasma creatinine after starting or increasing the dose of ACE inhibitor/ARB, but it is less than 25% (e. GFR) or 30% (serum creatinine) of baseline, the test should be repeated in a further 1– 2 weeks. If the change in e. GFR is 25% or more or the change in plasma creatinine is 30% or more: look for other causes (nsaids, dehydration, etc. ) if none found decrease/stop ACEI
 have been shown")
ACEI vs. ARB IN DCKD: only ACEI (at maximum tolerable doses) have been shown in well done placebo controlled trials to lower all cause mortality. (Cochrane 2006) Ontarget 2008 in Jama (ACEI plus ARB) n n n Older than 55, with atherosclerosis or DM with end-organ damage Ramipril 10 mg or telmisartan 80 mg or both (8, 000 in each arm) Evaluated every 6 months for 56 months ~12% in each arm died Combination arm was 0. 33% more likely to need acute dialysis NNH 565 pts for 56 months for 1 case of acute dialysis, however no benefit seen to combination therapy so don’t do it.

Stopping ACEI/ARB 2009 in Nephrology and Dialysis journal a observational study was published. 12 months before and after study was published. discontinuation of ACEi/ARB: CKD 4/5 61. 5% of patients had more than a 25% increase in e. GFR, whilst 36. 5% had an increase exceeding 50%. There was a significant decline in the e. GFR slope − 0. 39 ± 0. 07 in the 12 months preceding discontinuation. Mean arterial blood pressure (MAP) increased from 90 ± 1. 8 mm. Hg to 94 ± 1. 3 mm. Hg (p = 0. 02), however ≥ 50% of patients remained within target. Overall proteinuria was not affected (PCR before = 77 ± 20 and after = 121. 6 ± 33. 6 mg/mmol). No guidance from NICE or NKF, but makes sense to me given what we know about ARF
 of")
Diabetes We recommend a target hemoglobin A 1 c (Hb. A 1 c) of <7. 0% (53 mmol/mol) to prevent or delay progression of the microvascular complications of diabetes, including diabetic kidney disease. (NKF) Kahoot 11, 12, 13

Statins NICE: Treat all with CKD 3 or higher with atorvastatin 20 mg NKF: treat them as you would other patients Cochrane review 2014 n n n 50 studies Primary prevention Decrease cardiovascular disease and death by 20%, no effect on ckd progression and stroke.

Bones n n In people with GFR <45 ml/min/1. 73 m 2 (GFR categories G 3 b. G 5), we suggest maintaining serum phosphate concentrations in the normal range according to local laboratory reference values. (2 C) NICE: don’t check phosphorous pth vitamin d routinely if GFR above 30 We suggest not to prescribe bisphonate treatment in people with GFR <30 ml/min/1. 73 m 2 (GFR categories G 4 -G 5) without a strong clinical rationale. (2 B) NICE: Offer bisphonates if indicated for the prevention and NICE: treatment of osteoporosis in people with a GFR of 30 ml/min/1. 73 m 2 or more (GFR category G 1, G 2 or G 3).

Bones Continued We suggest not to perform bone mineral density testing routinely in those with e. GFR <45 ml/min/1. 73 m 2 (GFR categories G 3 b-G 5), as information may be misleading or unhelpful. (2 B) n In my opinion this only applies to those with renal osteodystrophy
 Treat only if low vitamin D")
Vitamin D Replace if less than 30 (NKF) Treat only if low vitamin D and use sterols if low and less than 30 GFR (NICE)

Low Protein Diet Cochrane review 2009 n 10 studies out of 40 included n 2, 000 pts 1, 000 in each arm n 168 renal deaths in high protein n 113 renal deaths in low protein n NNT 2 -56 patients for one year to prevent one death. n No comment on other mortality or exactly what low protein means around 0. 3 -0. 6 g/kg/d Nice recommends against low protein 0. 6 -0. 8 k/kg/day We suggest lowering protein intake to 0. 8 g/kg/day in adults with diabetes (2 C) or without diabetes (2 B) and GFR <30 ml/min/ 1. 73 m 2 (GFR categories G 4 -G 5), with appropriate education.

Sodium Bicarbonate July 16 2009 in the Journal of the American Society of Nephrology. n n 134 adult patients with stage 4 CKD and serum bicarbonate levels of 16 to 20 μmol/L. Randomized to 600 mg sodium bicarb tid or standard treatment. Bicarb was titrated up to keep serum HCO 3 level > 23 mmol/L Decline in Cr. CL decreased 5. 93 in placebo and 1. 88 in rx P<. 0001). Four patients in the bicarbonate group developed ESRD requiring dialysis (6. 5%) compared with 22 patients in the control group (33%; RR, 0. 13; 95% CI, 0. 04 – 0. 40; P <. 001).

Sodium Bicarbonate NKF: We suggest that in people with CKD and serum bicarbonate concentrations <22 mmol/l treatment with oral bicarbonate supplementation be given to maintain serum bicarbonate within the normal range, unless contraindicated. NICE: Consider oral sodium bicarbonate NICE: supplementation for people with both: n GFR less then 30 AND bicarb less then 20.

erythropoietin Randomized, controlled study comparing a hematocrit target of 42% with that of 30% among patients with heart disease who were undergoing hemodialysis, the former group had higher rates of nonfatal myocardial infarction and death, but not significantly so NEJM 1998 open-label, randomized trial, CKD, not on dialysis, treated with epo for 18 months, 1, 400 total patients: The use of a target hemoglobin level of 13. 5 g per deciliter (as compared with 11. 3 g per deciliter) was associated with increased risk and no incremental improvement in the quality of life : NEJM 2006 NICE: goal 10 -12 NKA: don’t use above 11. 5

Questions

Sources http: //www. kidney. org/Professionals/Kdoqi/guidelines_ckd/toc. htm Cochrane Database Essential evidence plus Mann JF, Schmieder RE, Mc. Queen M, et al. , for the ONTARGET investigators. Renal outcomes with telmisartan, ramipril, or both, in people at high vascular risk (the ONTARGET study): a multicentre, randomised, double-blind, controlled trial. Lancet 2008; 372(9638): 547 -553. J Am Soc Nephrol. 2009 Sep; 20(9): 2075 -84. Epub 2009 Jul 16 BMJ 2008 Mar 22: 336 (7645): 645 N Engl J Med 356: 956, March 1, 2007 Besarab A, Bolton WK, Browne JK, et al. The effects of normal as compared with low hematocrit values in patients with cardiac disease who are receiving hemodialysis and epoetin. N Engl J Med 1998; 339: 584 -590 Singh AK, Szczech L, Tang KL, et al. Correction of anemia with epoetin alfa in chronic kidney disease. N Engl J Med 2006; 355: 2085 -2098 Nephrol Dial Transplant. 2009 Oct 10 Palmer SC, Hayen A, Macaskill P, et al. Serum levels of phosphorus, parathyroid hormone, and calcium and risk of death and cardiovascular disease in individuals with chronic kidney disease. A systematic review and meta-analysis. JAMA 2011; 305(11): 1119 -1127.

Sources Navaneethan SD, Pansini F, Perkovic V, Manno C, Pellegrini F, Johnson DW, Craig JC, Strippoli GF. HMG Co. A reductase inhibitors (statins) for people with chronic kidney disease not requiring dialysis. Cochrane Database Syst Rev 2009; (2): CD 007784. http: //www. kdigo. org/clinical_practice_guidelines/pdf/CKD/KDIGO_2 012_CKD_GL. pdf https: //pathways. nice. org. uk/pathways/chr onic-kidney-disease#content=viewnode%3 Anodes-recommendations-forclinical-laboratories
- Slides: 43