Chronic diarrhea and malabsorption syndromes By Dr Tamara


Chronic diarrhea and malabsorption syndromes By Dr. Tamara Kufoof MD, pediatrician, MRCPCH Part 1, 2 Full time lecturer, mu’tah university Year 2017/2018 ﺭﺍﺋﺪ ﻋﻠﻲ : ﺗﺒﻴﻴﺾ ﺍﻟﻄﺎﻟﺐ

Definition � Chronic diarrhea: Diarrhea illness persisted more than 14 days, although others use a cutoff of 4 weeks. � Persistent diarrhea is an episode of diarrhea of infectious etiology, which develops acutely but continues for more than 14 days

Etiology of chronic diarrhea Classification according to these two vital factors: 1 - Age. 2 - Intraluminal vs mucosal factors.

Chronic diarrhea in infants Common causes: � Cow’s milk protein allergy. � Secondary disaccaridase deficiency � Infections as giardiasis and HIV. � Cystic fibrosis.

Rare causes Acrodermatitis enteropathica. Primary immune defects. Lymphangiectasia. Eosinophilic gastroenteritis. Intractable diarrhea syndrome. Abetalipoproteinemia. Shwachman syndrome. Bacterial overgrowth. Other rare causes.
 �")
Chronic diarrhea in older children Common causes � Chronic nonspecific diarrhea (toddler’s diarrhea) � Coeliac disease. � Secondary disaccaridase deficiency. � Infections as giardiasis and HIV. � CF

Rare causes Immune deficiency. Eosinophilic enteritis. Secretory tumors.

Chronic diarrhea in adolescents Common causes � IBS. � Giardiasis. � IBD � Lactose intolerance � Laxative abuse ( anorexia nervosa ). � celiac Rare causes � Secretory tumors. � Addison disease.
.")
Cont. carbohydrate intolerance Secondary lactose intolerance � � � Usually post-infectious ( rota virus). Bloating, abdominal discomfort and flatulence that occur from 1 hour to a few hours after ingestion of milk or dairy products may signify lactose intolerance. Stool characteristics: Loose, watery, acidic stool often with excessive flatus and associated with urgency that occurs a few hours after the ingestion of lactose-containing substances is typical.

Cont. carbohydrate intolerance Investigations: � � Reducing substances in the stool is positive and the stool is acidic with PH <5. 5. Breath hydrogen test : - Carbohydrate malabsorption results in bacterial fermentation of the unabsorbed sugar. Thus, carbohydrate malabsorption can be determined by measuring the exhaled hydrogen concentration after a carbohydrate load is administered. Management: Lactose free diet and LF milk

Cow’s milk protein allergy � usually starts in the first year when children are given cow milk products. � Symptoms : mild to severe � Typical symptoms are Vomiting, diarrhea, colic and constipation may occur. � Other rare presentations are wheezes, cough, atopic eczema and behavioral changes like irritability, crying and milk refusal. � A challenge with milk free times may have a good indicators. However, histopathological examination is a diagnostic test.
 � It")
Toddlers diarrhea � Called : chronic non specific diarrhea of childhood (CNSD) � It is a common problem. � 1 -3 Years � a benign condition. � Usually, the children have no failure to thrive and they present in a good nutritional state. Abdominal pain may be present in a minority. � The stool is often brown and watery, and contain mucus with undigested food particles. The parents are likely to report a short mouth to anus transit time. Mainly carbohydrates

Cont. Toddlers diarrhea Golden rules � In developed countries toddler diarrhea is the most frequent cause of chronic diarrhea in 1– 5 year old children � Toddler history diarrhea has a typical dietary and clinical hydrogen tests have no place in the diagnostic process � Breath � Rx: . Reassurance, . Normalization of feeding patterns according to the “four Fs”: Fat, Fiber, Fluid, and Fruit juices. Mainly due to carbohydrates

Post enteritis syndrome Persistent diarrhea after gastroenteritis is caused by: 1. Continuing infection. 2. Further infection. 3. Carbohydrate intolerance. 4. Post infection malabsorption syndrome. � Usually subsides, but severe cases may persist to longer periods. � Dx: Stool analysis and stool culture. � Rx: Treatment of the cause.
 � Fecal – oral route � Ingested cysts � Should suspect")
G. lamblia (Giardiasis) � Fecal – oral route � Ingested cysts � Should suspect in children with more than 5 days diarrhea � The diarrhea is voluminous and odoriferous but seldom contains blood

cont. Giardia trophozoite can infest healthy children chronically, but usually this is a clinical problem in debilitated or Immunodeficient children (selective Ig. A deficiency are particularly susceptible to persistent giardiasis )

Cont. � Causes a protracted but usually self-limiting diarrhea in well-nourished, immunocompetent children � Most people who have acute giardiasis become asymptomatic within 6 weeks of onset � Few otherwise healthy children develop prolonged diarrhea with weight loss of 10% to 15%, FTT, and stunting for 2 years or more � Rare Presentations(diarrhea is absent) : Anasarca

Diagnosis 1. 2. Antigen testing of stool Finding the organism on proximal intestinal biopsy Clinicians should have a high index of suspicion for giardiasis in children who have: � persistent diarrhea if the � child attends child care � drinks well water � lives near or visits lakes or streams � has lived in or visited underdeveloped regions

Treatment � Rx Metronidazole in a dose of 15 mg/kg for 10 days is the current treatment � Asymptomatic children generally are not treated

Cystic fibrosis � AR disorder. � Most patients have respiratory symptoms as recurrent pneumonia, and adenoid. � Those patients have pancreatic insufficiency which lead to diarrhea with greasy stool. � Failure to thrive. � Genetic diagnosis and sweat chloride test are the main investgations.

Acrodermatitis enteropathica AR disorder, Presentation � with peri-oral rash, chronic diarrhea, recurrent infection and napkin rash resistant to treatment. � Usually starts at the time of weaning. � Tent red hair and alopecia. � Diagnosis � Serum zinc and alkaline phosphatase concentrations are low � the signs and symptoms resolve after oral or parenteral zinc therapy Management Zinc supplements


Inflammatory bowel disease � � � Crohn’s disease and ulcerative colitis. 20% of cases presents under 20 years old. It has intestinal and extra intestinal manifestations.
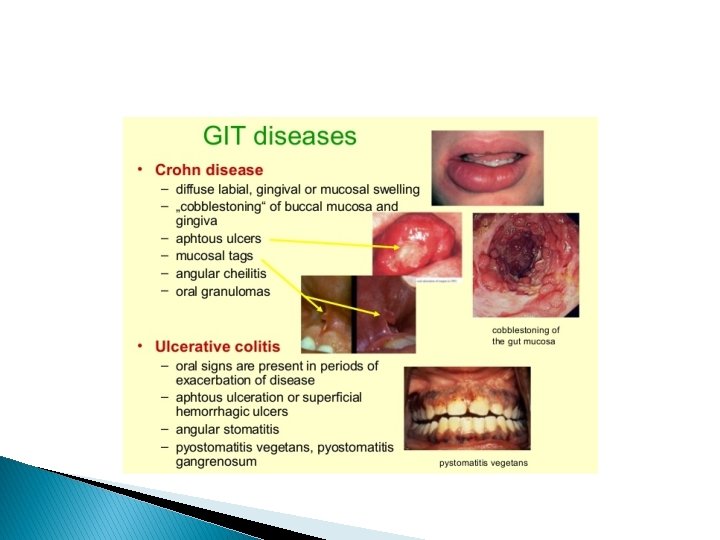
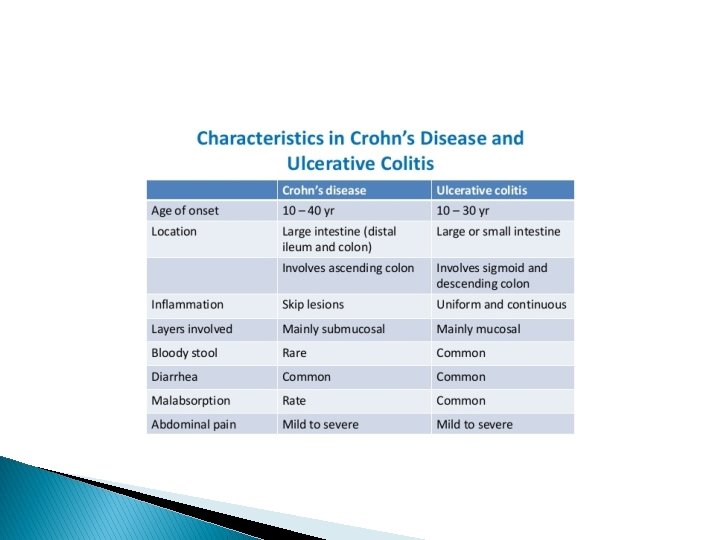

Cont. IBD Clinical picture � Diarrhea � Abdominal pain � Growth deceleration � Weight loss � Anorexia. � Colonic Crohn disease may be clinically indistinguishable from ulcerative colitis (UC), with manifestations that include the following: • Bloody mucopurulent diarrhea • Cramping abdominal pain • Urgency to defecate

� 1. 2. 3. 4. Perianal involvement in Crohn disease may produce the following: Simple skin tags, fissures, abscesses, and fistulae Painful defecation Bright-red rectal bleeding Perirectal pain, erythema, or discharge

Cont. IBD Investigations: � CBC… anemia. � ESR and CRP…. . Elevated. � Hypoalbuminaemia. � � A single-contrast upper GI radiologic series with small-bowel follow-through (SBFT). Colonoscopy, bx

Endoscopy � � � Colonoscopy with several colonic and terminal ileal biopsies is considered a standard diagnostic procedure. Upper endoscopy, or esophagogastroduodenoscopy (EGD), should be part of the first-line investigation. Video capsule endoscopy is increasingly being used to evaluate for small-bowel Crohn disease in children.

Irritable bowel syndrome � � � chronic or recurrent abdominal pain, altered bowel habits, and bloating, with the absence of structural or biochemical abnormalities to explain these symptoms. part of a broader group of disorders known as functional GI disorders. It is the most common GI diagnosis among gastroenterology practices in the United States and is one of the top 10 reasons for visits to primary care physicians.


Take care The following clinical features should alert the physician to the possibility of a disorder other than irritable bowel syndrome (red flags) � Frequent awakening by symptoms � Steady progressive course � Fever � Weight loss � Arthritis � Rectal bleeding � Persistent vomiting.

Evaluation of patients with chronic diarrhea Initially: � Hx and PE � CBC, KFT, Electrolytes, ESR � Stool workup: Ax, Cx, PH, reducing substances, fat � Stool for clostridium difficile toxin � Stool antigen for Giardia lamblia
: � Sweat chloride, � celiac work up,")
Second phase (guided by Hx and PE): � Sweat chloride, � celiac work up, � quantitative stool for fat (72 hrs collection of stool) � Alpha-one antitrypsin (in stool): for protein loosing enteropathy(PLE) 3 rd phase � Endoscopy (U&L), Biopsy � Barium studies

- Slides: 37