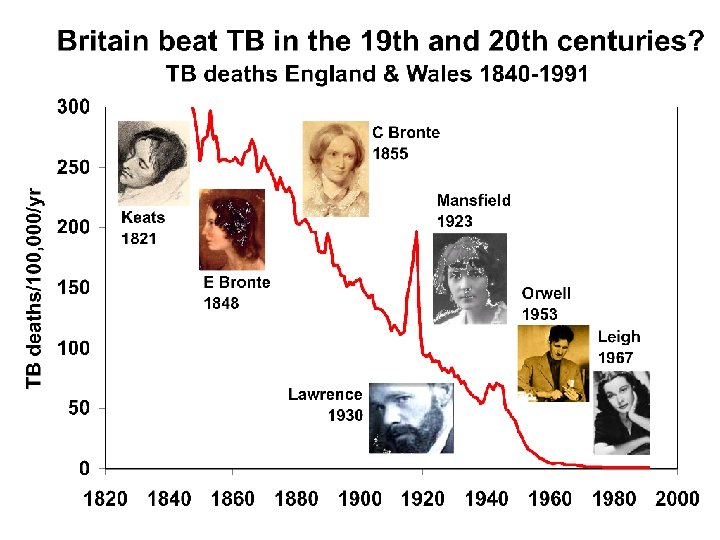
CHRISTOPHER DYE Drugs superbugs and Drugs superbugs and

CHRISTOPHER DYE Drugs, super-bugs and…

Drugs, superbugs and… What is an antibiotic? Why do bugs turn into superbugs? Superbugs: the clean-up New antibiotics: science or economics? CHRISTOPHER DYE What is a superbug?

What is a superbug?

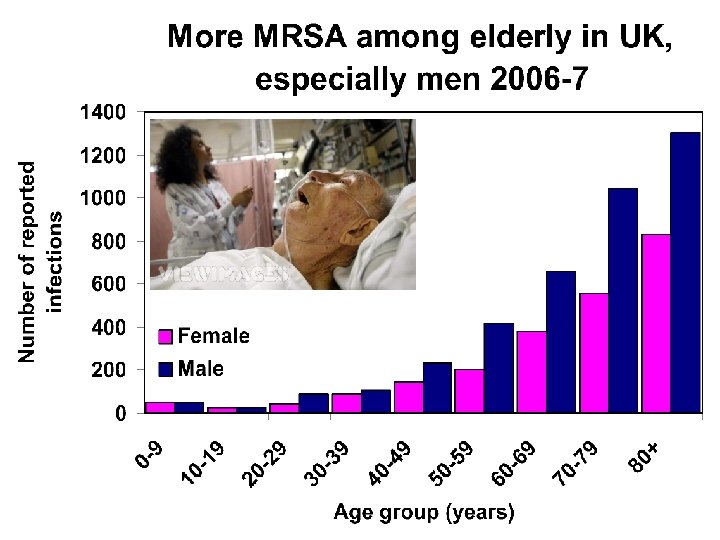
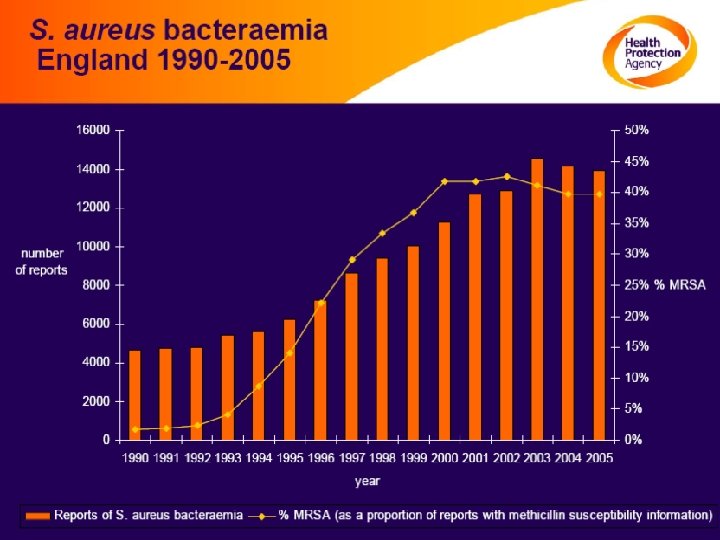
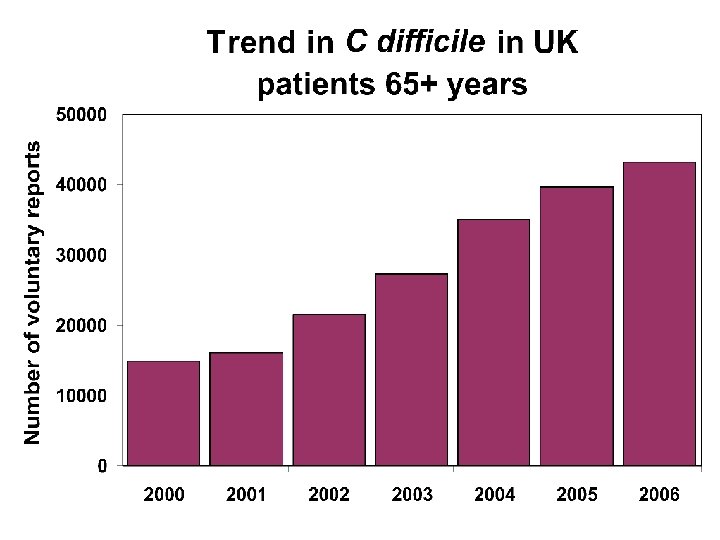
Superbugs, Super at what? Virulent, drug resistant, hospitals, rich countries MRSA methicillin resistant Staphylococcus aureus (UK 7000 cases falling) GRE Glycopeptide resistant Enterococcus (mostly vancomycin, 1000 cases rising) Virulent, hospitals Clostridium difficile (50, 000 cases rising, slowing) Virulent, drug resistant, community, poor countries Resistant Streptococcus pneumonia (100 s rising? ) MDR tuberculosis (40 rising? Isoniazid in London)

Not Ebola, Marburg, rabies, flu, HIV…

MRSA: Methicillin resistant Staphylococus aureus
 United States 2005 (and soon UK? ) In hospital")
MRSA: coming out (of hospital) United States 2005 (and soon UK? ) In hospital In community (after health care) In community (not after health care) 58% 27% 14% Of ≈ 100, 000 invasive MRSA infections Of ≈ 20, 000 deaths (1 in 5, > HIV/AIDS)

VRE: vancomycin resistant Enterococci Urine infections Heart infections Blood poisoning Wound infection

Clostridium difficile Diarrhoea Colitis Fever Abdominal cramp Abnormal heart rhythm
DR Streptococcus pneumoniae Middle ear infection Sinusitis Bronchitis Pneumonia Meningitis")
(M)DR Streptococcus pneumoniae Middle ear infection Sinusitis Bronchitis Pneumonia Meningitis

Out of hospitals… MDR Mycobacterium tuberculosis Lung destruction Bloody cough Spine/bone deformity Meningitis

MDR-TB among previously treated TB patients < 6% 6 – 20 % 20 – 40% > 40 % No estimate
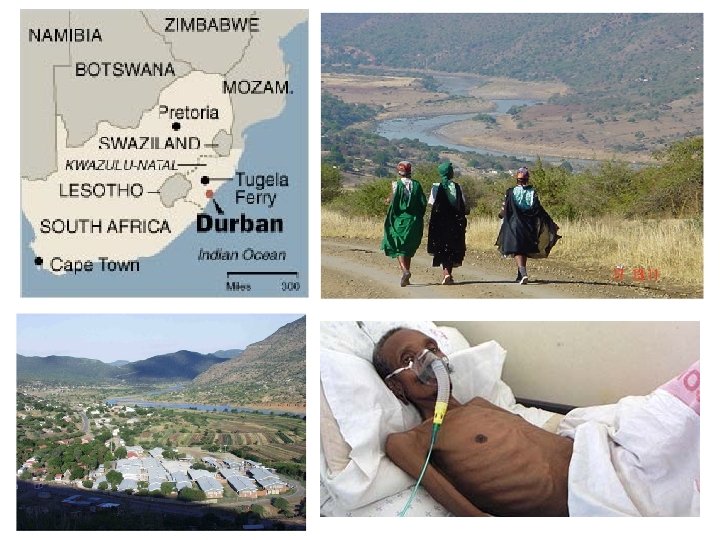

Proportion surviving Rapid death of TB XDR patients at Tugela Ferry: 52/53 died, half within 16 days Days since sputum collected

The travels and travails of Andrew Speaker

What is an antibiotic?
 collaborator of Louis Pasteur … life could be used to")
"Antibiosis" Paul Vuillemin (1889) collaborator of Louis Pasteur … life could be used to destroy life…. . Bacteriocides Bacteriostatics
: Penicillium did not become contaminated with bacteria Pasteur (1822")
"Antibiosis" before Fleming Roberts (1874): Penicillium did not become contaminated with bacteria Pasteur (1822 -95) and Joubert (1834 -1910): mould-contaminated cultures stopped the growth of the anthrax Lister (1871): urine contaminated with mould did not allow the growth of bacteria Duchesne (1897): substance that stopped bacterial growth, penicillin mould Acid (lactic) producing bacteria: to treat diphtheria, meningitis, cystitis and open wounds Fungus-like bacteria (Actinomycetes): dissolves cell walls of other bacteria and fungi; used to treat TB and others; origin of streptomycin Skin bacteria: protect against pathogenic bacteria and fungi (ringworm) Beer yeast: long-used antibiotic effects

Penicillin: the first antibiotic Fleming Chain Florey 1928/41
 The search for a")
"Hunting a beast through endless forests" (Kafka d. TB 1924) The search for a TB cure

Today's antibiotics CLASS Aminoglycosides Ansamycins Cephalosporins Glycopeptides Macrolides Penicillins Polypeptides Quinolones Sulfonamides Tetracyclines Others SOME EXAMPLES Streptomycin Geldanamycin Cefadroxil Vancomycin Erythromycin Penicillin Bacitracin Ciprofloxacin Mafenide Tetracycline Chloramphenicol, Isoniazid Metronidazole, Pyrazinamide

How antibiotics work… and then don't work Interfering with. . . • Making DNA/RNA rifampicin, chloroquine • Making proteins tetracycline, chloramphenicol • Cell membranes polyenes, polymyxin • Enzymes sulphamethoxazole • Cell walls penicillin, vancomycin

Total antibiotic dependency • 80 million prescriptions of antibiotics for human use each year • 12, 500 tons each year • 50% humans, 50% animals • 1 million tons consumed by humans and animals in past 50 years
 super bugs?")
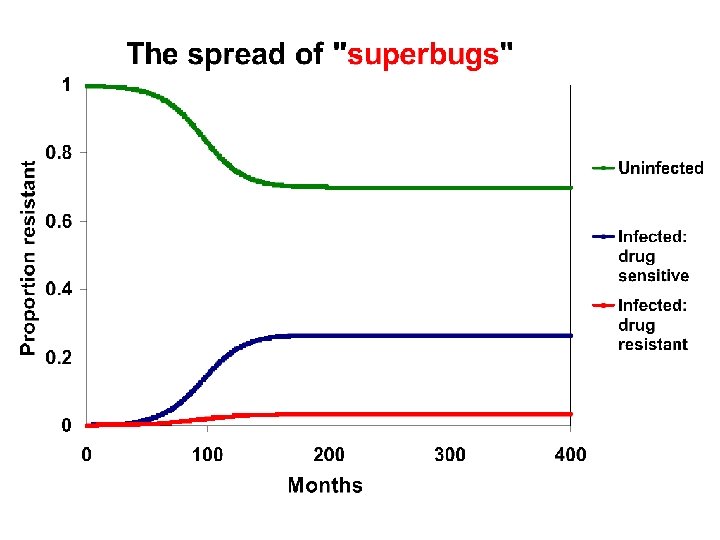
Why do bugs turn into (drug resistant) super bugs?

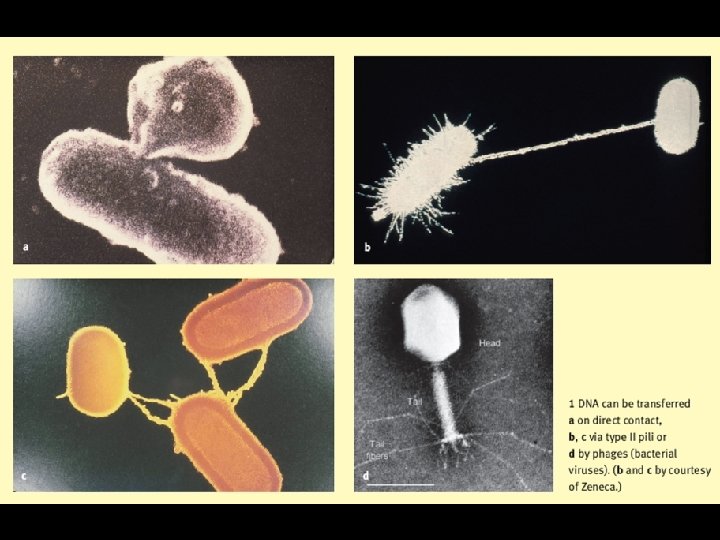
"The genetic lending library of evil…" Mutation Conjugation Transduction Transformation

Down in the pathospere resistance profiling of soil bacteria D'Costa et al 2006

Resistance: complex genetics but a simple selection process

Superbugs: not so super Rifampin-resistant mutants of TB from lab are less fit Gagneux, Science 2006

Superbugs: overcoming the handicap Rifampin-resistant mutants from patients are not less fit Gagneux, Science 2006

Evolution in action: promoting resistance with sub-therapeutic doses 1. Self-medication 2. Patients forget to take medication, interrupt treatment, cannot afford full course 3. Belief in new medications over old 4. Preferred injections of broad-spectrum drugs 5. Physicians pressured to prescribe antimicrobials 6. Pharmaceuticals marketed directly to public 7. Antibiotics poorly formulated, counterfeit, expired 8. Hospitals with highly susceptible patients, intensive antimicrobial use, cross-infection 9. Failure of simple infection controls e. g. handwashing 10. Veterinary prophylaxis or growth promotion, Salmonella and Campylobacter through food to humans

The arms race in Wonderland: at the court of the Red Queen to Alice: “Now, here, you see, it takes all the running you can do, to keep in the same place. If you want to get somewhere else, you must run at least twice as fast as that!”

Loss of resistance is slow Quickly in, slowly out Minimal fitness handicap Plasmids contain several resistance genes Resistant strains persist at low levels Finland: restricted macrolide use Erythromycin resistance in group A streptococci in Finland cut from 20% to 10% in 2 years

Superbugs: the clean-up

"Record numbers of Britons are flying abroad for medical treatment to escape…the rising threat of hospital superbugs. . "

"We shall fight them with bleaches… whatever the cost may be" "A ward at a time, walls, ceilings, fittings and ventilation shafts" "Every hospital will be disinfected and scrubbed clean over the next year"
 Handwashing Limiting invasive devices Environmental cleaning Judicious antibiotic use Surveillance")
Superbugs in captivity (hospitals) Handwashing Limiting invasive devices Environmental cleaning Judicious antibiotic use Surveillance ----- hospital

Assuming superbugs are less fit… In general Combination therapy In the community (>80% most respiratory) Restrict antibiotics for: coughs, colds, sore throats (unless strep), otitis media, sinusitis (or < 3 days) In hospital Minimize presumptive treatment, discontinue treatment asap, withhold key antibiotics In animals Minimize use sub-therapeutic dosing

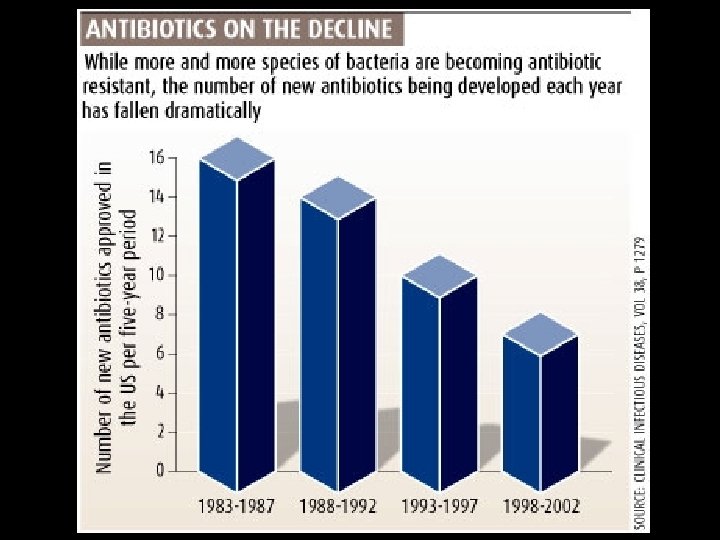
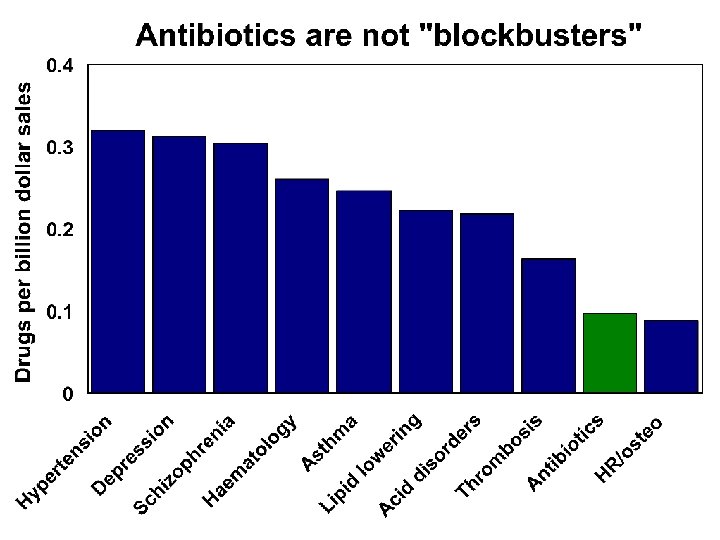
New antibiotics: hard science or hard sell?

Only 2 new classes of antibacterials since 1970 s Decade introduced Class of antibacterial 1930 s 1940 s 1950 s 1960 s sulphonamides penicillins, aminoglycosides chloramphenicol, tetracyclines macrolides, glycopeptides streptogramins, quinolones lincosamides trimethoprim 1970 s 1980 s 1990 s 2000 s oxazolidinones, lipopeptides Other licensed drugs since 1970 s in same classes

big pharma, bad karma? THE 2006 BITTER PILL AWARDS: While You Were Sleeping Award Overmarketing insomnia medications “Got Cholesterol? ” Award Overpromoting brand-name statins Driven to Distraction Award For hawking an Attention Deficit drug

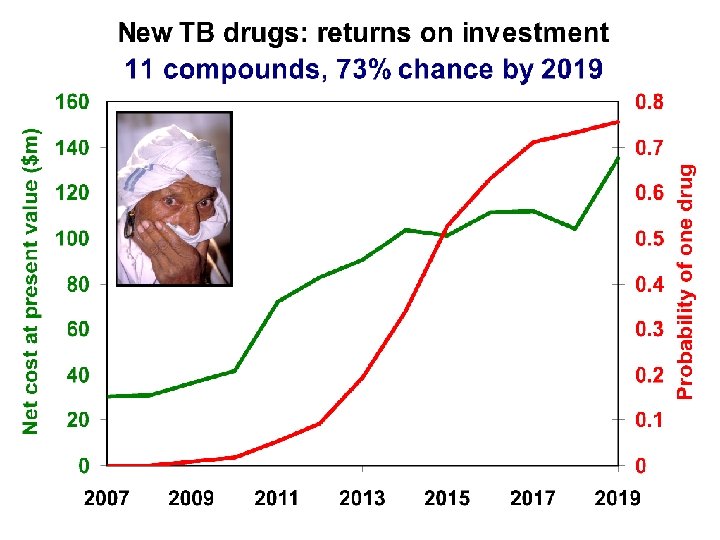
Who will make new drugs? Mostly Pharma but… Escalating costs Net present value Strict license standards Post-market surveillance Resistance Generics (short patents) Narrow spectrum Variable licensure High purchase price Low unmet need Short treatment time
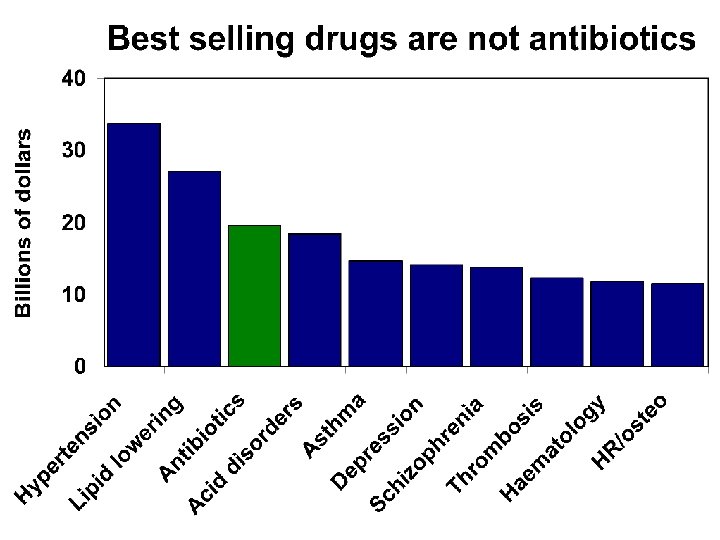

#1 Lipitor lowers cholesterol $11 billion #2 Nexium Heartburn Fastest sales growth
 Tax incentives for")
From "market failure" to market success Legislation Intellectual property (extended exclusivity) Tax incentives for R&D Guaranteed market Regulation Simplify regulation and clinical trials Financing Promote translational research and trials: bench to bedside Cash prizes (instead of patents) Surveillance Present and future drug needs

End of the antibiotic era? 1. 2. 3. 4. Adjustable balance between resistance and susceptibility… Resistance genes are inevitable, but their spread is preventable Resistance is reversible, though slowly Economic and regulatory levers to make and distribute new antibiotics have growing political commitment Other solutions: prevention, vaccines
- Slides: 56