CHOLINERGIC DRUGS Parasympathomimetcs Cholinomimetics Assoc Prof I Lambev
 Assoc. Prof. I. Lambev E-mail: itlambev@mail. bg")
CHOLINERGIC DRUGS (Parasympathomimetcs, Cholinomimetics) Assoc. Prof. I. Lambev E-mail: itlambev@mail. bg
 portion of the nervous system can b into two major subdivisions:")
The motor (efferent) portion of the nervous system can b into two major subdivisions: autonomic and somatic. The autonomic nervous system (ANS) is largely indep in that its activities are not under direct conscious contro It is concerned primarily with visceral functions such a cardiac output, blood flow to various organs, and dig which are necessary for life. The somatic division is largely concerned with conscio controlled functions such as movement, respiration, and Nerve impulses elicit responses in smooth, cardi and skeletal muscles, exocrine glands, and postsynaptic neurons by liberating specific chemical neurotransmitters.

By using drugs that mimic or block the actions of c transmitters, we can selectively modify many auto functions. These functions involve a variety of effe tissues, including cardiac muscle, smooth muscle, vascular endothelium, exocrine glands, and presynaptic nerve terminals. Autonomic drugs are useful in many clinical condit
 division and the parasympathetic (craniosacral)")
The ANS has two major portions: the sympathetic (thoracolumbar) division and the parasympathetic (craniosacral) division. Both divisions originate in nuclei within the CNS and give rise to preganglionic efferent fibers that exit from the brain stem or spinal cord and terminate in motor ganglia. The sympathetic preganglionic fibers leave the CNS through the thoracic and lumbar spinal nerves. The parasympathetic preganglionic fibers leave the CNS through the cranial nerves (especially the third, seventh, ninth, and tenth) and the third and fourth sacral spinal roots.
 and storage.")
Parasympathetic nerves regulate processes connected with energy assimilation (food intake, digestion, absorption) and storage. These processes operate when the body is at rest, allowing a increased bronchomotor tone and decreased cardiac activity. Secretion of saliva and intestinal fluids promotes the digestion of foodstuffs; transport of intestinal contents is speeded up because of enhanced peristaltic activity and lowered tone of sphincteric muscles. To empty the urinary bladder (micturition), wall tension is increased by detrusor activation with a concurrent relaxation of sphincter tonus.

Activation of ocular parasympathetic fibers results in narrowing of the pupil and increased curvature of the lens, enabling near objects to be brought into focus (accommodation).

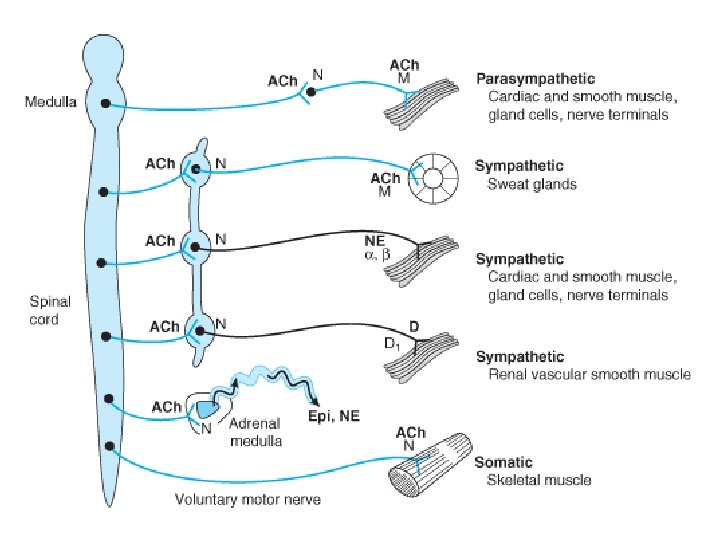
ACh serves as mediator at terminals of all postganglionic parasympathetic fibers, in addition to fulfilling its transmitter role at ganglionic synapses within both the sympathetic and parasympathetic divisions and the motor endplates on striated muscle. However, different types of receptors are presented at these synaptic junctions.

CHOLINERGIC NERVES

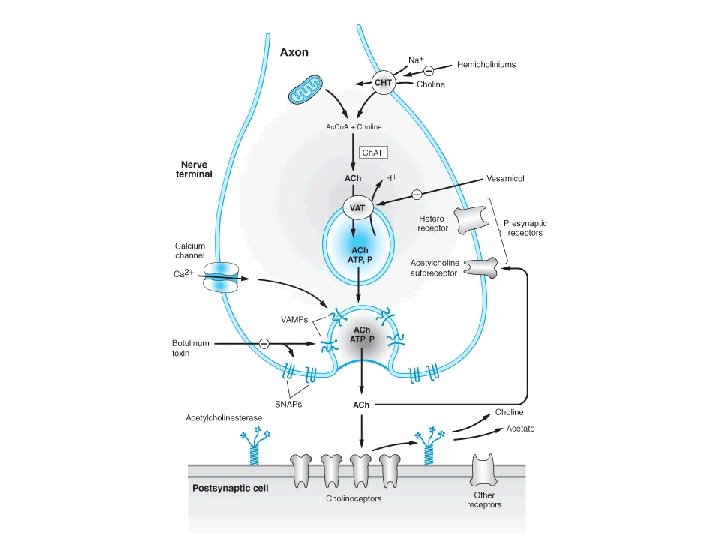
ACh is highly concentrated in synaptic storage vesicles present in the axoplasm of the terminal. ACh is formed from choline and activated acetate acetylcoenzyme A), a reaction catalyzed by the enzyme choline acetyltransferase. The highly polar choline is actively transported into the axoplasm. The specific choline transporter is localized exclusively to membranes of cholinergic axons and terminals.
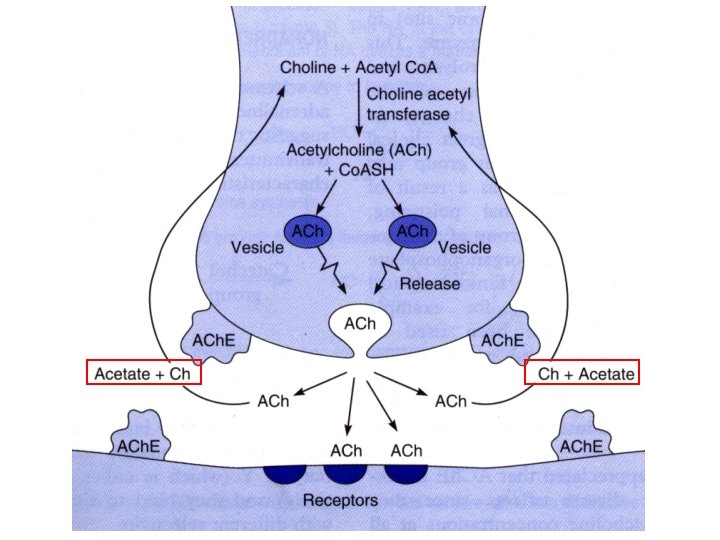

During activation of the nerve membrane, Ca 2+ enters into the axoplasm through voltage-gated channels to activate protein kinases. As a result, vesicles close to the presynaptic membrane and fuse with this membrane. During fusion, vesicles discharge their contents into the synaptic gap. ACh quickly diffuses through the synaptic gap. The molecule of ACh is a little longer than 0. 5 nm. The synaptic gap is as narrow as 30– 40 nm.

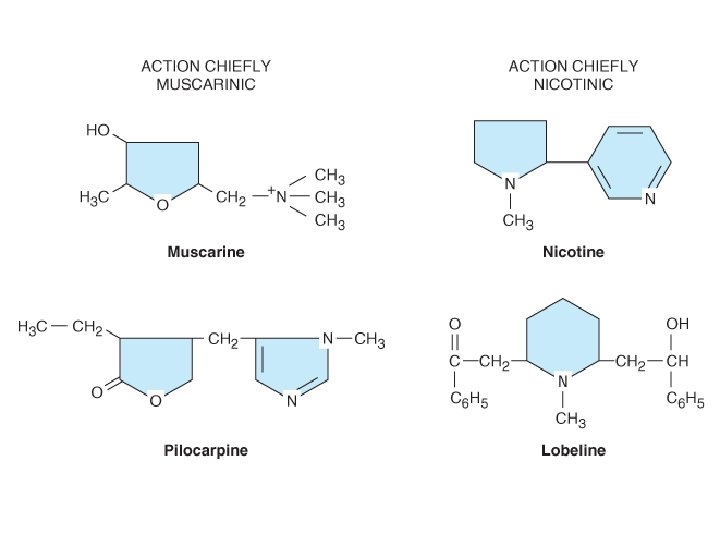
At the postsynaptic effector cell membrane, ACh reacts with its receptors. Because these receptors can also be activated by the alkaloid muscarine, they are referred to as muscarinic (M-) cholinoceptors. In contrast, at ganglionic and motor endplate cholinoceptors, the action of ACh is mimicked by nicotine and they are, therefore, said to be nicotinic (N-) cholinoceptors. Released ACh is rapidly hydrolyzed and inactivated by a specific acetylcholine esterase, present on pre- and postjunctional membranes, or by a less specific serum choline esterase (butyryl choline esterase), a soluble enzyme present in serum and interstitial fluid.

M-cholinoceptors can be classified into subtypes according to their molecular structure, signal transduction, and ligand affinity in the M 1, M 2, M 3 subtypes etc. M 1 -receptors are presented on nerve cells, e. g. , in ganglia, where they mediate a facilitation of impulse transmission from preganglionic axon terminals to ganglion cells. M 2 -receptors mediate acetylcholine effects on the heart. Opening of K+ channels leads to slowing of diastolic depolarization in sinoatrial pacemaker cells and a decrease in heart rate.

M 3 -receptors are found in the glandular epithelia (which respond with activation of phospholipase C and increases secretory activity) and in smooth muscle. In smooth vessels, the relaxant action of ACh on muscle tone is indirect, because it involves stimulation of M 3 -cholinoceptors on endothelial cells that respond by liberating NO. In the CNS, where all subtypes are presented, cholinoceptors serve diverse functions, including regulation of cortical excitability, memory, learning, pain processing, and brain stem motor control.
")
Muscarinic receptor (G protein-linked: 7 subunits)

Presynaptic regulation of transmitter release from noradrenergic and cholinergic nerve terminal

Characteristic of Nicotinic receptors NM-cholinoceptors Location: neuromuscular junction Function: depolarization of muscle end plate and contraction of skeletal muscle NN-cholinoceptors Location: autonomic ganglia Function: depolarization postganglonic membrane (in adrenal medula – catecholamine release)

The NM-receptor is a macroprotein with 5 subunits, which are arrange like rosette surrounding the Na+ channel. The two alpha subunits carry two ACh binding sites with negatively charged groups which combine with the cationic group of ACh and open Na+ channel.

N-receptor: 5 subunits

Acetylcholine receptor stimulants and cholinesterase inhibitors together comprise a large group of drugs that mimic ACh (cholinomimetic agents) Cholinoceptor stimulants are classified by their spectrum of action depending on the type of receptor – muscarinic or nicotinic, that is activated. They are also classified by their mechanism of action because some cholinomimetic drugs bind directly to (and activate) cholinoceptors, while others act indirectly by inhibiting the hydrolysis of endogenous ACh.
 Choline ester (stimulants of M- and N-receptors): Acetylcholine, Carbachol")
I. DIRECT-ACTING CHOLINERGIC DRUGS (1) Choline ester (stimulants of M- and N-receptors): Acetylcholine, Carbachol etc. (2) Alkaloids a) stimulants of M-receptors: Pilocarpine, Cevimeline (dry mouth), Bethanechole, Musacarine, Phalloidin b) stimulants of N-receptors: Nicotine, Cytisine (Tabex®), Lobeline

4+ N Ionization!!! BBB
![Blood pressure [mm Hg] M- и N-effects of ACh A 1 min B C](http://slidetodoc.com/presentation_image_h2/7405d92bc97a9366ec972cedd6737375/image-25.jpg "Blood pressure [mm Hg] M- и N-effects of ACh A 1 min B C")
Blood pressure [mm Hg] M- и N-effects of ACh A 1 min B C D 200 150 100 50 M- M- N- effect Atropine. ACh ACh 2 mg i. v. 50 mcg 5 mg 2 mcg i. v. 50 mcg

Pilocarpus jaborandi • Pilocarpine - in glaucoma
 - sol. 1%, 2%, 4% - in open angle")
Pilocarpine Hydrochloride eye drops (Pilocar®) - sol. 1%, 2%, 4% - in open angle glаucoma Applied to the eye, it penetrates cornea and promptly causes miosis, ciliary muscle contraction, and fall in intraoccular tension (< 22 mm) lasting 4 -8 h. Side effect: painful spasm of accommodation for near. Systemic effects: sweating, salivation Cardiovascular effects: in small doses – fall in BP, but in high doses elicits rise in BP and tachycardia, probably due to ganglionic stimulation (through muscarinic receptors)

Development of angle closure glaucoma and its reversal by miotics A. Mydriasis occurs in an eye with narrow iridocorneal angle and iris makes contact with lens blocking passage of aqueous from posterior to anterior chamber. B. Possible builds up behind iris which bulges forward and closes the iridocorneal angle thus blocking aqueous outflow. C. Miotic makes the iris thin and pupils it away from the lens removing the pupilary block and restoring aqueous drainage.
 and site of action of mydriatics (B) and miotics")
Autonomic control of pupil (A) and site of action of mydriatics (B) and miotics (C)
 Amanita phalloides (phalloid")
Amanita muscaria (muscarine) Amanita phalloides (phalloid
 Nicorette (chewing gum) Nicotinell® TTS")
Cytisine (Tabex® p. o. ) Nicorette (chewing gum) Nicotinell® TTS
 (1) Reversible drugs (more are")
II. INDIRECT-ACTING CHOLINERGIC DRUGS (anticholinesterase drugs: anti. Ch. Es) (1) Reversible drugs (more are carbamates) a) With N 3+ (cross BBB) Alkaloids: Galantamine, Physostigmine Synthetic drugs: Donepezil, Rivastigmine, Tacrine b) With N 4+ (do not cross BBB) Demecarium, Edrophonium (Tensilon®) Neostigmine, Pyridostigmine
 Irreversible anticholinesterase agents (more of them are organophosphates) a) Thiophosphate insecticides Parathion Malathion")
(2) Irreversible anticholinesterase agents (more of them are organophosphates) a) Thiophosphate insecticides Parathion Malathion (Pedilin® – in pediculosis) b) Nerve paralytic gases for chemical warfare Tabun Sarin Soman

Representative "reversible" anticholinesterase agents employe

Anti. Ch. Es inhibit Ch. E and protect ACh from hydrolysis. They produce cholinergic effects and potentiates ACh both in vivo and in vitro. Lipid soluble agents (physostigmine and organophosphates) have more marked muscarinic and CNS effects, stimulates ganglia but action on skeletal muscles is less prominent (NB: the action of Galantamine on skeletal muscles is more strong in comparison with neostigmine).
 produce more marked")
Lipid insoluble anti. Ch. Es (neostigmine and other quaternary ammonium compounds) produce more marked effect on the skeletal muscles (direct action on muscle end-plate NN-cholinoceptors as well). Stimulate ganglia but muscarinic effects are less prominent. They do not penetrate in CNS and have no central effects.

Galantamine is anti. Ch. Es with direct N-action, used in: • Myastenia gravis • Alzheimer’s disease • Poliomyelitis • Postoperative paresis of GIT and bla • As antagonist of competitive myorelaxants with the less side effects than neostigmine Prof. D. Paskov (1914– 1986) Galantamine (Nivalin®)
 is a disease affecting skeletal muscle neuromuscular junctions. An autoimmune process")
Myasthenia gravis (MG) is a disease affecting skeletal muscle neuromuscular junctions. An autoimmune process causes production of antibodies that bind to the a subunits of the nicotinic receptor. This effect causes accelerated degradation of the receptor and blockade of ACh binding to receptors on muscle end plates. Frequent findings are ptosis, diplopia, difficulty in speaking and swallowing, and extremity weakness. Severe disease may affect all the muscles, including those necessary for respiration. The disease resembles the neuromuscular paralysis produced by tubocurarine and similar nondepolarizing neuromuscular blocking drugs. Patients with myasthenia are sensitive to the action of curariform drugs and other drugs that interfere with neuromuscular transmission e. g. , aminoglycoside antibiotics. Anti-Ch. Es are extremely valuable as therapy for myasthenia. Almost all patients are also treated with immunosuppressant drugs and some with thymectomy. Edrophonium is used as a diagnostic test in myasthenia gravis.
 normal and (B) myasthenic neuromuscular junctions. The MG junction has a")
Diagrams of (A) normal and (B) myasthenic neuromuscular junctions. The MG junction has a normal nerve terminal; a reduced number of ACh. Rs and a widened synaptic space.

• In the Alzheimer’s disease in brain tissue there amyloid plaques and neurofibrillarly tangles, as well as loss of cholinergic neurons. • Cholinacetyl trasferase activity in the cortex and hippocampus is reduced from 30% to 70%. • Loss of cholinergic neurons contributes for much of the learning and memory deficit. • The number of M-cholinoceptors is not affected, but the number of N-receptors are reduced.

Thin brain cortex Enlargement ventricles Diminished hypothalamus Alzheimer's disease

Reversible anti-ACh. Es used in: • Glaucoma: pilocarpine, demecarium • Myasthenia gravis: edrophonium, galantamine, neostigmine, physostigmine, pyridostigmine • Alzheimer’ disease: donepezil, galantamine, aminopyridine (Pymadine®), rivastigmine, tacrine • Postoperative paralytic ileus or/and urinary retention: galantamine, neostigmine • Postoperative decurarization: galantamine, neostigmine, pymadine (it releases ACh!) • Belladonna poisoning: physostigmine, neostigmine, galantamine • Cobra bite (cobra venom has a curare like neurotoxin): galantamine, neostigmine

Reactivators of Ch. E, used for treatment of intoxication with organophosphates
- Slides: 44