Childhood Obesity Dr Mouna Dakar Obesity is the

Childhood Obesity Dr. Mouna Dakar

Obesity is the most prevalent nutritional disorder among children and adolescents in the United States. Approximately 21 -24% of American children and adolescents are overweight, and another 16 -18% is obese.
 children")
These findings indicate that the prevalence of overweight (BMI ≥ 85 th percentile) children and adolescents in the US has increased by 50 -60% in a single generation. and the prevalence of obesity has doubled.

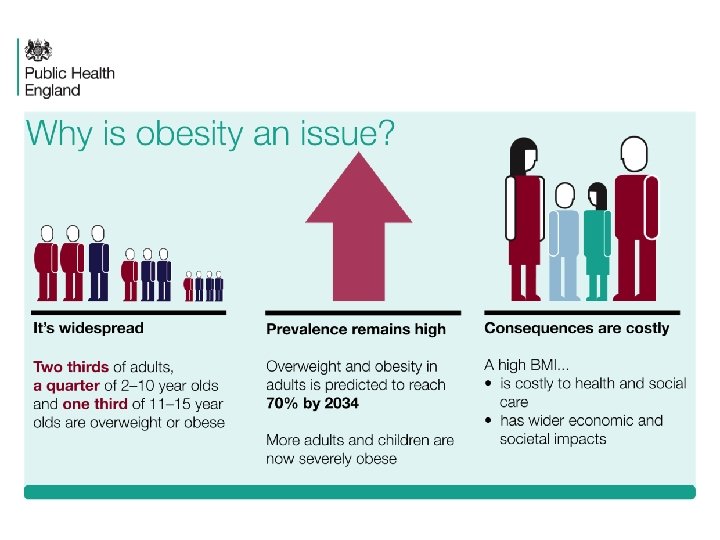
• An estimated 300 million people around the world are obese as defined by a body mass index (BMI) of 30 or more • At least 155 million school-age children worldwide are overweight or obese

Prevalence of obesity among children National Child Measurement Programme 2013/14 Around one in ten children in Reception is obese (boys 9. 9%, girls 9. 0%) Around one in five children in Year 6 is obese (boys 20. 8%, girls 17. 3%) Child obesity: BMI ≥ 95 th centile of the UK 90 growth reference 5 Patterns and trends in child obesity

BMI status of children by age National Child Measurement Programme 2013/14 This analysis uses the 2 nd, 85 th and 95 th centiles of the British 1990 growth reference (UK 90) for BMI to classify children as underweight, healthy weight, overweight and obese. These thresholds are the most frequently used for population monitoring within England. 6 Patterns and trends in child obesity

Prevalence of obesity by school year, sex, and year of measurement National Child Measurement Programme 2006/07 to 2013/14 7 Patterns and trends in child obesity Child obesity: BMI ≥ 95 th centile of the UK 90 growth reference 95% confidence intervals are displayed on the chart
 indicates that the prevalence of obesity")
The National Health and Nutrition Examination Survey (NHANES) indicates that the prevalence of obesity is increasing in all pediatric age groups, in both sexes.

Obesity in children is a complex disorder. Its prevalence has increased so significantly in recent years that many consider it a major health concern of the developed world.

Many factors, including genetics, environment, metabolism, lifestyle, and eating habits, are believed to play a role in the development of obesity.

Background: Factors Contributing to Childhood Obesity Many factors interact to contribute to obesogenic environments and affect children’s weight. These include: Genetic and individual factors Home influences The school environment Factors in the local community Wang Y, Wu Y, Wilson RF, et al. AHRQ Comparative Effectiveness Review No. 115. Available at www. effectivehealthcare. ahrq. gov/child-obesity-prevention. cfm.

However, more than 90% of cases are idiopathic; less than 10% are associated with hormonal or genetic causes.

Genetic syndromes associated with childhood obesity include the following: Prader-Willi syndrome Pseudohypoparathyroidism Laurence-Moon-Biedl syndrome (Bardet-Biedl) syndrome Down syndrome Turner syndrome

Genetics of childhood obesity • Genetic – – • • higher concordance between monozygotic than dizygotic twins high concordance in body fat in monozygotic twins raised apart Genetics do not explain rapid increase in obesity rates High rates of parental obesity - probably due to genetics and shared environment

Hormonal disorders associated with childhood obesity include the following: Growth hormone deficiency Growth hormone resistance Hypothyroidism Glucocorticoid excess (Cushing syndrome) Precocious puberty Polycystic ovary syndrome (PCOS) Prolactin-secreting tumors

Medications that may cause weight gain in children and adolescents include the following: Cortisol and other glucocorticoids Sulfonylureas Tricyclic antidepressants (TCAs) Monoamine oxidase inhibitors (MAOIs), such as phenelzine Insulin (in excessive doses)

Georgia add campaign

Background: Health Consequences of Childhood Obesity Overweight children and adolescents are at greater risk for health problems when compared with their normal-weight peers and are more likely to become obese adults. Obese children and adolescents are more likely to have serious illnesses such as type 2 diabetes, hypertension, high cholesterol, stroke, heart disease, nonalcoholic fatty liver disease, certain types of cancer, and arthritis. Other reported health consequences of childhood obesity include eating disorders and mental health issues such as depression and low self-esteem Centers for Disease Control and Prevention. Available at www. cdc. gov/obesity/childhood/index. html. Reilly JJ, Kelly J. Int J Obes (Lond). 2011 Jul; 35(7): 891 -8. PMID: 20975725. Wang Y, Wu Y, Wilson RF, et al. AHRQ Comparative Effectiveness Review No. 115. Available at www. effectivehealthcare. ahrq. gov/child-obesity-prevention. cfm.
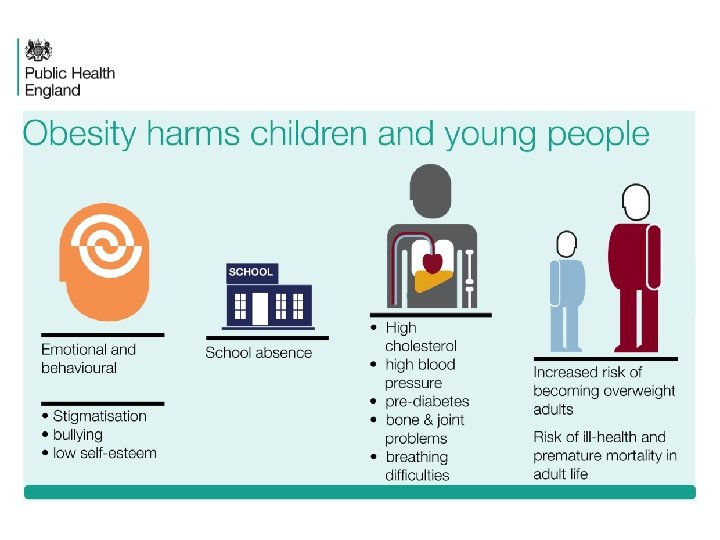

Complications Metabolic • Hyperlipidaemia • Hypertension • Insulin resistance and abnormal glucose tolerance • Poor pulmonary function • Asthma • Advanced growth and early maturity • Hepatic steatosis and cholelithiasis, • Low grade systemic inflammation, • Sleep apnoea, • Polycystic ovary disease • Orthopaedic complications eg SUFE, flat feet Psychosocial • • isolation, stigmatisation, bullying psychological problems eg depression

History and Physical Examination

Short stature or a reduced rate of linear growth in a child with obesity suggests the possibility of growth hormone deficiency, hypothyroidism, cortisol excess, pseudohypoparathyroidism, or a genetic syndrome such as Prader-Willi syndrome.

A history of dry skin, constipation, intolerance to cold, or fatigability suggests hypothyroidism.

Polyuria and polydipsia may be noted if the adolescent with obesity develops overt diabetes.
 (eg, infection, trauma, hemorrhage,")
A history of damage to the central nervous system (CNS) (eg, infection, trauma, hemorrhage, radiation therapy, seizures) suggests hypothalamic obesity with or without pituitary growth hormone deficiency or pituitary hypothyroidism.

A history of morning headaches, vomiting, visual disturbances, and excessive urination or drinking also suggests that the obesity may be caused by a tumor or mass in the hypothalamus.

Selective accumulation of fat in the neck, trunk, and purple striae suggest an excess of cortisol, particularly if the rate of linear growth has declined.

excessive facial hair, acne, and irregular periods in a teenage girl suggest that the weight gain may be caused by cortisol excess or polycystic ovary syndrome (PCOS).

Diagnosis of obesity in children • • • Obesity in adults defined by BMI level associated with short and long term disease and mortality risk Childhood obesity acute complications are uncommon and longer term risks are harder to track No uniformly accepted diagnosis but most refer to BMI >95 th centile (overweight is >85 th), using age and sex specific centiles BMI 95 th centile approximates BMI of 30 by age 19 BMI centile charts in med tech or online (CDC)

www. cdc. gov/growthcharts

Other measure of obesity or adiposity • BMI SDS – Is the number of standard deviations from the mean – BMI SDS of 2 is equivalent to the 95 th centile – Good to track over time • Waist circumference • Waist to hip ratio • Percentage body fat – Bioelectrical impedance – Skin fold thickness

Approach Considerations

The following laboratory studies may also be indicated in patients with obesity: Fasting lipid panel for detection of dyslipidemia Thyroid function tests Adrenal function tests, when indicated, to assess the possibility of Cushing syndrome Growth hormone secretion and function tests, when indicated Assessment of reproductive hormones (including prolactin), when indicated Serum calcium, phosphorus, and parathyroid hormone levels to evaluate for suspected pseudohypoparathyroidism

To identify high-risk patients, Maffeis et al reported that obese children and adolescents with a fasting plasma glucose value greater than or equal to 86 mg/d. L are most likely to manifest impaired glucose tolerance.

37 ©M. Miqdady, M. D. 18 -May-21

Management 38 For overweight children small reduction in calories allows gradual decline in BMI For obese children & adolescents weight loss of 0. 5 -1 kg/week is the goal. Special diets like protein rich diet not recommended

Education points to address Do not eat while talking on the phone or watching TV Avoid appetizer and dessert in restaurants Eat a healthy snack before going to a holiday party so you will feel full

Your Eating Habits Small, frequent meals at regularly scheduled times Regularly scheduled snacks of fruit or vegetables Do not skip meals No foods are off limits however in order to encourage success moderation is the key

The “Toxic Environment” • supersized High-Calorie Food is… – Highly palatable – Inexpensive – Heavily advertised – Near-ubiquitous Brownell KD & Horgen KB. Food Fight. New York: Mc. Graw-Hill; 2003.

Cutting Back On Calories But Feeling Full Add vegetables to as many things as possible Eat several servings of fruits daily Avoid processed & fried foods, red meat, ghee butter, cream & chocolates Some fat is needed to provide essential nutrients to the body; use veg. oils like olive & sunflower, but avoid saturated fats. Watch foods labeled “fat-free” or “lowfat”; you may consume more calories

In 1980, about 50 percent of high school seniors reported eating green vegetables “nearly every day or more. ” By 2003, that figure had dropped to about 30 percent. (YES Occasional Papers. Paper 3. Ann Arbor, Mich. : Institute for Social Research, May 2003) From the statistical sourcebook “A Nation at Risk: Obesity in the United States. ” To order, call 1 -800 -AHA-USA 1 or email inquiries@heart. org
 at restaurants as they do during")
Children eat nearly twice as many calories (770) at restaurants as they do during a meal at home (420). From the statistical sourcebook “A Nation at Risk: Obesity in the United States. ” To order, call 1 -800 -AHA-USA 1 or email inquiries@heart. org

Exercise vs. Lifestyle Physical Activity Exercise Lifestyle Physical Activity

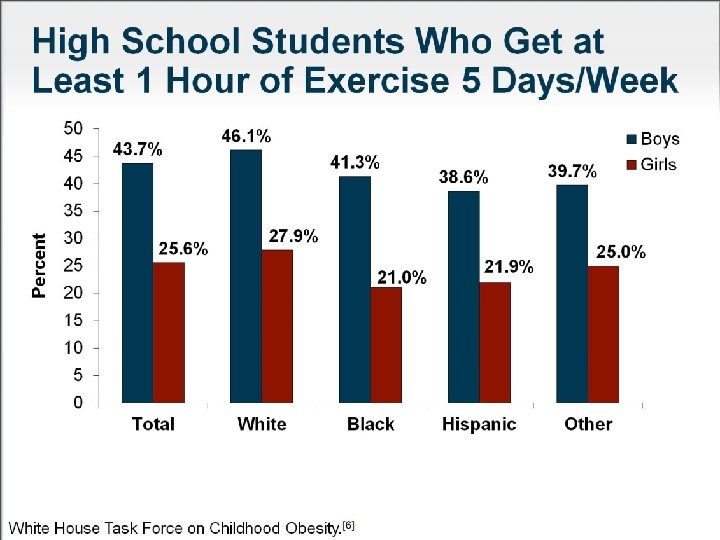
Physical activity among children Health Survey for England 2012 Around two in ten children aged 5 -15 years meet the government recommendations* for physical activity (boys 21%, girls 16%) *Child recommendations for physical activity in CMO report 2011 – one hour moderate activity per day HSE reports at least 60 minutes of moderate to vigorous activity on all seven days in the last week 46 Patterns and trends in child physical activity

Surgical Intervention

Various bariatric surgical procedures have been used in adults and some adolescents (in most centers, patients ≥ 15 y) with a body mass index (BMI) of more than 40 kg/m 2 or weight exceeding 100% of ideal body weight (IBW).

Prevention

In 2010, the American Heart Association issued guidelines for the primary prevention. A few of the recommendations were as follows:

Diet and nutrition: A diet that is low in sodium and high in potassium is recommended to reduce blood pressure; diets that promote the consumption of fruits, vegetables, and low-fat dairy products

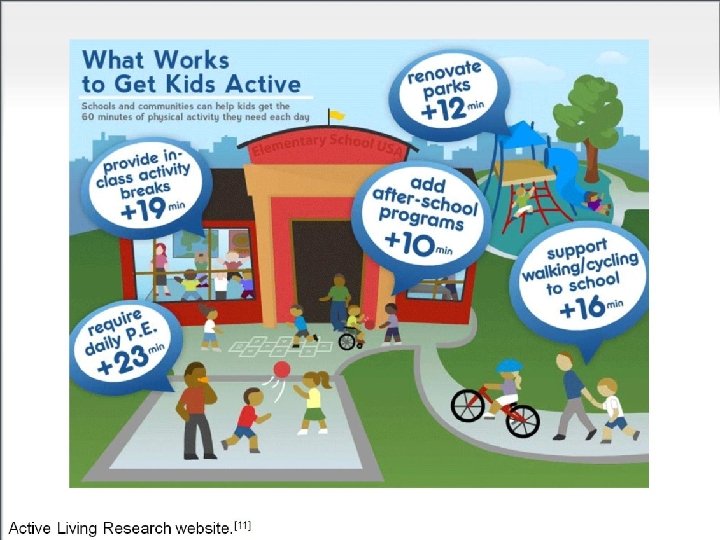
Physical inactivity: Increasing physical activity is associated with a reduction in the risk of obesity. the goal is to engage in at least 30 minutes of moderate intensity activity on a daily basis

Thanks for your attention View Notes
- Slides: 57