Childhood Anxiety Disorders Anxiety mood state characterized by

Childhood Anxiety Disorders

Anxiety: mood state characterized by strong, negative emotion and bodily symptoms in which an individual apprehensively anticipates future danger or misfortune Fear: immediate alarm reaction to current danger Anxiety disorder: excessive and debilitating anxiety with negative emotion and fear

FIGHT AND FLIGHT RESPONSE

ANXIETY CYCLE

Developmental Considerations Anxiety is an adaptive emotion that readies children both physically and psychologically to cope with danger Infancy: loud noises, being startled, strangers Toddlerhood: dark, separation School-Age: injury, natural disasters Adolescence: competency-based concerns, health of self and others

Developmental Considerations DSM-IV qualifiers for children Anxiety may be expressed by crying, tantrums, freezing, or clinging Unlike adults, children are not required to acknowledge that fears are unreasonable or excessive Difficulties in recognizing symptoms Internalizing symptoms less observable Internalizing symptoms less aversive Children may lack verbal skills to communicate concerns

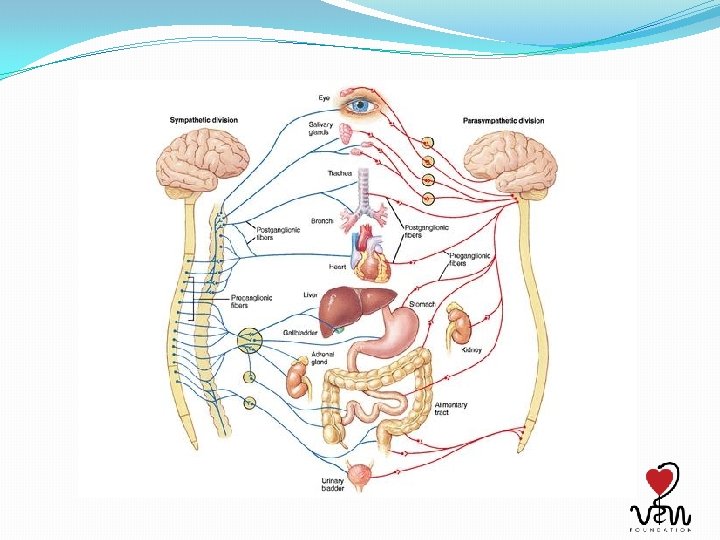
Anxiety: 3 Interrelated Systems �Cognitive �Anxious thoughts develop in response to cognitive distortions in the attention, interpretation, and memory components of information processing �Physical �Brain sends messages to sympathetic nervous system: fight or flight response �Symptoms are excessive in intensity or duration �Behavioral �Action (or inaction) that individuals take to prevent exposure to feared stimuli or to reduce anxiety associated

Case Example �“Charlie, now 11 years old , is entering 6 th grade in a middle school. Each September since kindergarten the start of school has always been a struggle for him. This year his distress escalated with the added demand of starting in a new school, and by November he missed twenty-six days of school. His academic work has suffered, and his teachers have sent his assignments home. Charlie insists that he can't complete them without his mother's presence. He worries that something

Separation Anxiety Disorder DSM Criteria: 3+ symptoms � Excessive distress when separation from attachment figure is anticipated � Excessive worry about losing or possible harm to figure � Excessive worry that an event will lead to separation � Reluctance or refusal to go to school because of separation fear �Excessive fear or reluctance to be alone �Reluctance or refusal to go to sleep without being near attachment figure �Nightmares involving theme of separation �Complaints of physical symptoms when separation occurs/is anticipated

SAD: Clinical Presentation Demand parental attention Clinging Sleep with parents

Prevalence, Age of Onset, Family Characteristics �Prevalence rate of 2 - 4% �SAD accounts for 1/2 of all children and adolescents referred for treatment of anxiety disorders �Occurs as early as preschool age �No gender differences �Often occurs in response to some major stressor

Case Example “Corinne's mother tried everything she could think of to get her 14 -year-old daughter to join an after-school club or accept invitations to parties at classmates' homes. Corinne insisted that she would rather stay home and read; she didn't think she fit in with her friends any more and didn't know what to say to them. When she did venture out with a cousin, it took her hours to do her makeup because she didn't think she looked quite right. ”

Social Phobia DSM Criteria �Marked and persistent fear of one or more social or performance situations in which child is exposed to unfamiliar people or possible scrutiny by others �The child fears he/she will act in a way that will be humiliating or embarrassing �Exposure to situation provokes considerable anxiety �Feared situations are avoided or else endured with intense anxiety

Social Phobia: Clinical Features A child with social phobia is one who displays phobic responses to one or more social situations: Speaking, eating, or drinking in front of others Initiating or maintaining conversations Speaking to adult authority figures Other situations that may elicit concerns over being embarrassed/humiliated

Social Phobia: Clinical Features In young children, the anxiety may be reflected in signs of distress such as crying, throwing temper tantrums, or becoming mute and clinging to parents In older children, it may be expressed less dramatically in terms of trembling hands, a shaky voice or other obvious signs of anxiety

Social Phobia: Clinical Features �Children with social phobias also experience anticipatory anxiety well before actually confronting these situation �Unfortunate cycle �Anticipate awkwardness/poor performance �Increased anxiety �Actual awkwardness/poor performance �Can interfere with the child's ability to function in a wide range of areas

Social Phobia: Associated Features Children with social phobias can also show a range of associated features: Being overly sensitive to criticism Having low levels of self-esteem Having inadequate social skills School performance may be impaired due to test anxiety and failure to participate in classroom activities Social anxieties can result in school refusal

Social Phobia: Prevalence Relatively rare in the general child population Prevalence estimates of around 1 -3% are suggested by cross-sectional research No gender differences Last, et al. (1992) has suggested that among children referred to an anxiety disorders clinic, 20% met DSM criteria for a diagnosis of social phobia Thus, social phobia does not seem to be uncommon among children displaying anxiety related problems

Case Example Donna presented to therapy because she reported that she was unable to concentrate at home, at school, and with friends. She indicated that she had difficulty falling asleep at night because her mind was “constantly racing” with thoughts and concerns about anything and everything. She described feeling constantly tense and uptight, noting significant difficulty in just being able to enjoy a relaxing activity, like reading or watching TV.

Generalized Anxiety Disorder Excessive anxiety, unrealistic worries, and fearfulness, not related to a specific object or situation Child finds it difficult to control worry Plus one of the following symptoms Restlessness or feeling keyed up/on edge Being easily fatigued Difficulty concentrating or mind going blank Irritability Muscle tension Sleep disturbance

Generalized Anxiety Disorder “What if? ” statements Marked degree of subjective distress and excessive worry about a things including: the appropriateness of past behavior possible injury or illnesses (to themselves or others), the possibility of major calamitous events their ability to live up to expectations their competencies in various areas being accepted by others other things related to concerns about the future

GAD: Clinical Characteristics Children tend to be perfectionistic, worrying about what others will think of them or their performance Engage in excessive approval seeking and frequent solicitations of reassurance Anxiety level contributes to physical symptoms: headaches, dizziness, shortness of breath, upset stomach and problems in sleeping, which may also become a source of concern and worry Some children also develop "nervous habits" such as nail biting, and hair pulling
, in a review of epidemiological studies, suggests prevalence estimates of")
GAD Prevalence Strauss (1994), in a review of epidemiological studies, suggests prevalence estimates of 3% to 5% with younger children (< 11 years) Prevalence rates for adolescents across studies ranged from 4% - 7% GAD is somewhat more frequently seen in adolescents No significant gender differences

Case Example The mother of 5 -year-old Louisa, says "I go through a routine every night with Louisa. She always makes the same requests when I put her to bed; don't let the bed go up in the sky. Don't let the moon break the house. Don't let any alligators, cows, or snakes into the house. Scott, age 4, is afraid of the banging of the radiator in his room, the wail of a siren, the noise of thunder. Serena, age 5, and her mother look under her bed every night to make sure there are no witches hiding there.
,")
Childhood Fears and Phobias Childhood fears are quite common Lapouse and Monk (l 959), in a classic survey of 6 to 12 year‑old children, found that some 43% had 7+ fears Childhood fears range from those related to very specific and concrete objects (e. g. , animals and strangers) to those which are more abstract (e. g. , monsters, war, death). Some fears seem to be age or stage specific, occurring frequently at certain ages

Childhood Fears: Developmental Considerations Fear of strangers at age 6 to 9 months Fear of separation at age 1 to 2 years Fear of the dark at around age 4 Many fears resolve with time and do not require treatment Some fears are more problematic and the term “phobia” is a more appropriate descriptor of the child's condition.

Specific Phobia DSM Criteria �Marked and persistent fear that is excessive and unreasonable, cued by the presence or anticipation of a specific object or situation �Exposure to the phobic stimulus almost invariably provokes an immediate anxiety response �Duration of 6 months �Types: � Animal (e. g. , snakes) � Natural environment (e. g. , storms) � Blood-injection-injury � Situational (e. g. , bridges, elevators, flying) � Other (e. g. , loud sounds, choking)
 have defined a phobia as a")
Childhood Phobias Miller, Barrett and Hampe (l 974) have defined a phobia as a specific type of fear that is: out of proportion to the demands of the situation cannot be explained or reasoned away is beyond voluntary control leads to avoidance of the feared situation persists over an extended period of time is not adaptive is not age or stage specific

Childhood Phobias: Prevalence Little investigation of the prevalence of these problems in children 2 - 4% in the general child population Rates on the order of 4% are found for adolescents Rates as high as 6 - 7% are found in clinical populations

Case Example “Jesse, l 0 years old, cleans his teeth so frequently that he uses a box of toothpicks each week and his gums bleed profusely. Each day he uses a half box of Q-tips to clean his ears and a roll of toilet paper when he goes to the toilet. When he does his homework, Jesse can spend an hour on the same page, erasing and rewriting words because he's sure he didn't get them right. ”

Case Example “Ashley, l 6, reports that each time she leaves a classroom, passes the principal's office or leaves school, she has to imagine the number 12 on a clock and say the words "good luck" to herself. She reports that she can't stop thinking about the words "good luck. " If she tries to stop herself from thinking about these words, she becomes very anxious and worries that she'll have a heart attack. In the classroom, she is often frozen in her seat, unable to respond. She worries that any decision she makes will result in something dreadful happening to her parents. Before going to sleep, she closes the bedroom door four times, turns the lights on and off four times and looks out the window and under her bed twelve times. ”

Obsessive-Compulsive Disorder DSM Criteria DSM IV Criteria A. Either obsessions or compulsions: Obsessions as defined by (1), (2), (3), and(4): 1. Recurrent and persistent thoughts, impulses, or images that are experienced, at some time during the disturbance, as intrusive and inappropriate and that cause marked anxiety or distress 2. The thoughts, impulses, or images are not simply excessive worries about real-life problems 3. The person attempts to ignore or suppress such thoughts, impulses, or images, or to neutralize them with some other thought or action 4. The person recognizes that the obsessional thoughts, impulses, or images are a product of his or her own mind (not imposed from without as in thought insertion)
 and (2): Obsessive-Compulsive Disorder Criteria 1. Repetitive behaviors (e.")
Compulsions as defined by (1) and (2): Obsessive-Compulsive Disorder Criteria 1. Repetitive behaviors (e. g. , DSM hand washing, ordering, checking) or mental acts (e. g. , praying, counting, repeating words silently) that the person feels driven to perform in response to an obsession, or according to rules that must be applied rigidly 2. The behaviors or mental acts are aimed at preventing or reducing distress or preventing some dreaded event or situation; however, these behaviors or mental acts either are not connected in a realistic way with what they are designed to neutralize or prevent or are clearly excessive

B. At some point during the course of the disorder, Obsessive-Compulsive Disorder Criteria the person has recognized that the. DSM obsessions or compulsions are excessive or unreasonable. Note: This does not apply to children. C. The obsessions or compulsions cause marked distress, are time consuming (take more than 1 hour a day), or significantly interfere with the person’s normal routine, occupational (or academic) functioning, or usual social activities or relationships. D. If another Axis I disorder is present, the content of the obsessions or compulsions is not restricted to it. E. The disturbance is not due to the direct physiological effects of a substance (e. g. , a drug of abuse, a medication) or a general medical condition

Common Obsessions and Compulsions �Obsessions �Contamination �Harm to self or others �Need for symmetry/order �Religious or moral concerns �Sexual or aggressive �Lucky or unlucky numbers Compulsions Cleaning Checking, counting, repeating Ordering, straightening Praying, confessing, reassurance seeking Touching, tapping, or rubbing Hoarding

OCD: Prevalence and Course Prevalence 1 -4% of children and adolescents Ratio of boys to girls is 2: 1 in childhood; equalizes in adolescence 80% of all cases have childhood onset Course Age of onset Males years 6 - 15 years (peak 10); Females 20 - 29 Onset typically gradual, some acute Chronic waxing and waning of symptoms Stress exacerbates symptoms Estimated that 15% display progressive deterioration in social & occupational functioning

Case Example �Dylan, 4 years old, presented to treatment because his parents were concerned with his behavior following a incident in which he was attacked by a dog. According to his parents, Dylan would use his toys to reproduce the incident in play. Additionally, Dylan avoided going anywhere near his neighbor’s house (where the dog attack occurred) and became noticeably startled and very distressed when hearing dog barking. For the past several weeks, he had experienced several nightmares in

�A. Exposure Post-traumatic Stress Disorder Criteria �Person exposed to a event that DSM involved threat of harm/death to self or other �Person’s response involved intense fear, helplessness, or horror �B. Traumatic event is re-experienced (1+) �Recurrent and intrusive recollections (play) �Recurrent and distressing dreams �Acting or feeling as if event were recurring (reenactment) �Intense distress at exposure to internal or external cues that resemble an aspect of the event �Physiological reactivity on exposure to cues

PTSD DSM Criteria �C. Persistent avoidance of stimuli associated with trauma and numbing of general responsiveness (3+) �Efforts to avoid thoughts/feelings about event �Efforts to avoid activities, places, people related to event �Inability to recall an important aspect of trauma �Markedly diminished interest or participation �Feeling of detachment from others �Restricted range of affect
 Difficulty falling or staying")
PTSD DSM Criteria D. Persistent symptoms of increased arousal (2+) Difficulty falling or staying asleep Irritability or outbursts of anger Difficulty concentrating Hypervigilance Exaggerated startle response E. Duration of symptoms > 1 month

Associated Characteristics of Anxiety Disorders �Cognitive disturbances �Interference with academic performance �Attentional biases (toward threat) �Cognitive biases (negative spin on ambiguous situations) �Physical symptoms �Sleep �Aches/pains �Social and emotional deficits �Interference �Low self-esteem �Loneliness

Etiology �Anxiety arises from a complex interaction of specific characteristics related to the child (e. g. , biological, psychological, and genetic factors) and his or her environment (e. g. , conditioning, observational learning, family relations, traumatic events) �Focus on four most recognized models �Biological �Behavioral �Cognitive �Ecological

Etiology Biological Genetic Influences Biological vulnerability to inherit a fearful disposition Genetic influences account for 1/3 of variance Neurobiological factors Within the limbic system, the behavioral inhibition system is overactive Increased tendency to become over-reactive and withdraw in response to novel stimulation Irritable, shy, cautious, and quiet temperament

Etiology Biology, continued Neurochemical factors Abnormal function of serotonin, norepinephrine, dopamine, and GABA

Etiology Behavioral Mowrer’s Two Stage Model of Conditioning Acquisition of fear through classical conditioning An individual associates a threatening stimulus with a nonthreatening stimulus, so that the latter by itself triggers anxiety Maintenance of fear through operant conditioning Negative reinforcement is manifested by avoidance and/or escape learning Consequently, without opportunities for new learning provided by exposure, the fear/anxiety does not extinguish

Etiology Behavioral, continued Observational learning Children learn about anxiety-provoking situations by observing others experience such situations or by acquiring information through activities like reading or watching the news on television

Etiology �Cognitive �Attentional biases toward threat-related information � Selectively attend to information that may be potentially threatening �Distorted judgments of risk � Negative spin on ambiguous/non-threatening situations � Lead them to select avoidant solutions �Selective memory processing � Tendency to remember anxiety-provoking cues/experiences �Perfectionistic beliefs �Inflated sense of responsibility

Etiology Ecological Bidirectional relationships among child, family, and other environmental contributions to anxiety Child temperamental characteristics (i. e. , behavioral inhibition) X insecure parentchild attachment X anxious and controlling parenting styles Parental modeling of fear responses Community violence

Assessment Diagnostic Interviews Anxiety Disorders Interview Schedule for DSM-IV Schedule for Affective Disorders and Schizophrenia for School-Age Children Clinician-administered Comprehensive Time-consuming and labor-intensive
 Multidimensional")
Assessment Rating Scales Screen for Child Anxiety Related Emotional Disorders - Revised (SCARED) Multidimensional Anxiety Scale for Children Fear Survey Schedule for Children – Revised Also, disorder-specific measures Quick and easy to administer Standardized with good psychometric properties Can be used as screening devices *not to diagnose
 Behavioral avoidance to phobic stimulus")
Assessment Observation Social-evaluative tasks (e. g. , classroom presentation) Behavioral avoidance to phobic stimulus Parent-child interaction Self-monitoring procedures Quantify and describe symptoms

Treatment Behavioral and Cognitive-Behavioral Treatments have received most empirical support Pharmacotherapy has recently received promising support Selective Serotonin Reuptake Inhibitors (SSRIs) Psychodynamic and Family therapies have not received much empirical support

Treatment �Treatments should target the 3 interrelated symptoms �Physical symptoms � Rapid heart beat � Muscle tension � Insomnia �Cognitive symptoms � Distorted perceptions of threat �Behavioral symptoms � Avoidance � Escape

Behavioral Therapy Exposure Therapy Systematic Desensitization Relaxation Exercises Contingency Management Strategies Modeling

Exposure �Create fear hierarchy �List of fearful events, rated on 0 -100 scale from least to most anxietyprovoking �Example: Fear of snakes � Talk about snakes 3 � See pictures of snakes 5 � Watch movies of snakes 6 � Touch a rubber snake 8 � Go to pet store and hold snake 10 �Gradual exposure: Child confronts fear

Exposure with Response Prevention Obsessive-compulsive disorder In addition to exposures, the child is asked to refrain from engaging in compulsive rituals Example Touches floor of public bathroom (exposure) Does not engage in handwashing (response prevention) Proposed therapeutic mechanism of exposure Break the conditioned fear response Consequently, acquire new, less threatening (and more adaptive), fear representations

Systematic Desensitization � 3 Steps �Teach child to relax �Construct fear hierarchy �Present anxiety-provoking stimuli sequentially as child remains relaxed �Proposed therapeutic mechanism �Break the conditioned fear response, because relaxation is incompatible with fear response �Which is better? ? ?

Relaxation Deep breathing Imagery Progressive Muscle Relaxation Proposed therapeutic mechanism Increased control over sympathetic nervous system Decreased physiological symptoms

Reinforced Practice: in vivo exposure with a feared situation or object and rewards (e. g. praise, tokens, toys, hugs, etc. ) for approaching and confronting a feared situation or object

Modeling Filmed modeling Live modeling Participant modeling

Cognitive-Behavioral Therapy In addition to behavioral strategies… Teaches children to understand how thoughts contribute to anxiety And how to modify distorted thoughts to decrease symptoms FEELINGS THOUGHTS BEHAVIOR

Cognitive-Behavioral Therapy �Components �Psychoeducation about nature of symptoms �Skill building � Cognitive restructuring � Positive self-talk � Problem solving � Approach-oriented coping � Relaxation strategies �Exposure �Role play �Contingency reinforcement: rewards

Coping Cat: CBT for Anxiety �Developed by Phil Kendall at Temple University �It is based on basic Cognitive Behavioral Principles �Treatment typically takes place across 16 sessions where the child is taught: �how to recognize their physical reactions and anxious feelings when confronted with anxiety related stimuli �to become aware of anxiety-related cognitions �to develop a coping plan for dealing with anxiety that involves positive self statements and problem solving skills

Coping Cat �The child is also taught to evaluate their coping responses and apply self-reinforcement for adaptive coping behaviors �Children are encouraged to engage in both imaginal and in vivo exposure to anxiety related stimuli, while using the skills they have been taught �In-session and out-of-session activities are used to give children opportunities to use skills �Therapists also reinforce the successful use of coping skills

Anxiety Disorders �Anxiety disorders are the most common mental health disorders �Many anxiety disorders start in childhood and if untreated, they may persist into adulthood �Children may have more than one kind of anxiety disorder �Up to 6% of children and youth have an anxiety disorder severe enough to need treatment
 tendency to anxiety")
get anxiety disorders? Often. Why theredo is children a family (genetic) tendency to anxiety Children who live with too much stress can become anxious Stress can be in family, school or neighborhood Anxious parents can model anxious behaviour for children

Kinds of Childhood Anxiety Disorders Separation anxiety Social phobia Generalized anxiety disorder Selective mutism Obsessive Compulsive Disorder Panic Disorder Phobias Post Traumatic Stress Disorder
 �They may worry that")
Separation Anxiety Disorder �Child is afraid of leaving their parent(s) �They may worry that something bad will happen to the parent or to someone they love or to themselves �May refuse to go to school �May have stomachaches, headaches, or throw up if they fear separation �May refuse to go to playdates at other people’s houses �Diagnosed if it causes problems at school or socially and has been going on at least 4 weeks

Generalized Anxiety Disorder Children with this kind of anxiety may: Have lots of worries and fears Have problems sleeping because of worries Have trouble concentrating Get tired easily or have tension headaches Be tense or restless Be perfectionist Have an anxious desire for approval

Obsessive-Compulsive Disorder �OCD often begins in early childhood or adolescence. Children with this kind of anxiety may: �Have frequent uncontrollable thoughts (obsessions) �Usually they don’t like these thoughts, or they may think they don’t make sense �Perform certain behaviours or rituals to try and prevent something bad from happening (or to get rid of thoughts) �Examples are: handwashing a lot if there is a fear of germs; checking that doors are locked; special touching rituals

Panic Disorder �Happens less often with younger children �People with this kind of anxiety have panic attacks �Feel very scared �Heart pounding, hard to breathe �May feel shaky, dizzy, or sick �May feel like they are going crazy or something really awful is going to happen �Sometimes they avoid school or want to stay in the house �Frequent panic attacks = panic disorder

Selective Mutism Children may not talk to anyone who is not close to them, such as immediate family They may look down, withdraw, turn red if required to talk Often they whisper if they do speak in a situation where they are anxious Up to 2% of school age children may have these symptoms Some kids outgrow it; some go on to have social phobia

Social Anxiety/Social Phobia Happens more in teens than in young children Fear and worry about social situations Going to school Speaking in class Social events including recess and lunch Shy, self-conscious Easily embarrassed These kids tend to be sensitive to criticism and find it hard to be assertive

Post Traumatic Stress Disorder �Symptoms start after a physical or emotional trauma or very frightening event �Can be marked by several of �Behavioural changes �Repetitive play �Zoning out, numbing of feelings �Jumpiness and watchfulness of surroundings �Nightmares and sleep problems �“Flashbacks” Not very common in young children
 �Frequent")
Anxiety disorders - What to watch for: �Avoidance of school (refuses to go) �Frequent stomachaches or headaches in the morning before school �Avoidance of activities �Easily upset – distress out of proportion �You spend a lot of time comforting your child and/or urging her/him to participate in regular activities �You feel that your family functioning is being disrupted by your child's fears and worries, or meltdowns

What parents can do: �Be patient, calm and reassuring �Be positive about their ability to manage the situation (with support) �Help your child succeed by doing “small steps” �Reward and praise your child’s efforts as well as successes �Be a model for your child – manage your own anxieties �Help your child “avoidance” with planned gradual exposure to things they fear �Teach your child positive self-talk

What parents can do: �Teach your child basic relaxation strategies such as belly breathing and muscle relaxation �Teach your child to visualize or imagine a pleasant, relaxing “happy place” �Keep stress low at home. Avoid parental conflict when the children are present. Be calm and positive as much as possible. �Deal with external situations that require adult intervention, such as bullying �Healthy living: enough sleep, regular routines, balanced diet, exercise �Take time to have fun and relax with your child

Don’t: Criticize or yell at your child Tease or make fun of your child for anxiety Ignore the problem or wait for the child to get over it Tell the child to “toughen up” Pressure your child to do more than s/he can do Have unrealistic expectations Make it easy for your child to avoid anything that scares them

Tell parents: �If the child is having significant problems with school, missing a lot of school, or having other problems functioning, you should talk to your doctor �Anxiety disorders can be treated! �The most common treatment is cognitive behavior therapy (CBT) in groups or individually �In CBT children learn relaxation and stress management plus �Gradual exposure to things that make them anxious, to decrease the fear �Coping strategies to reduce anxiety CBT is first choice, but medication may be needed in severe situations

SAD Behavioral components: Cognitive components: Extra targets: School refusal

Social Phobia Behavioral components: Cognitive components: Extra targets: Social Skills Training

Generalized Anxiety Disorder Behavioral components Cognitive components Extra targets: Reassurance seeking

Specific Phobia Behavioral components Mostly transient conditions

OCD Behavioral components: Cognitive components: Extra Targets: Medications SSRIs: Luvox, Paxil, Prozac, and Zoloft Majority of children on medication improve, but may relapse and need further treatment.

PTSD � Trauma-focused CBT 1. psychoeducation and parenting skills 2. relaxation 3. affective modulation: identifying and coping with negative emotions 4. cognitive strategies 5. trauma narrative 6. in vivo mastery of trauma reminders 7. conjoint child-parent sessions 8. enhancing future safety and

That is all! Any Questions
- Slides: 87