Child Health Nursing Partnering with Children Families Jane


































 –")






")



 • A method of administering IV or epidural analgesic using")






- Slides: 53
Child Health Nursing Partnering with Children & Families Jane W. Ball Ruth C. Bindler Chapter 18 Pain Assessment and Management Child Health Nursing: Partnering with Children & Families By Jane W. Ball and Ruth C. Bindler © 2006 Pearson Education, Inc. Pearson Prentice Hall Upper Saddle River, NJ 07458
Acute Pain- the History ! • Before 1970 - no formal research looking at pain management in children • Swafford and Allen, 1968: “pediatric patients seldom need medication for pain relief” • 1974 – 13/25 children received no analgesia after surgery such as nephrectomies, palate repairs and traumatic amputations
Do children feel pain? • Pain fibers present at end of 2 nd trimester • Increased heel sensitivity post heel sticks • Crying increases for days post circumcision • 6 month olds-anticipate and avoid pain
What is Pain? • “Pain is whatever the experiencing person says it is, existing whenever they say it does” (Mc. Caffery and Pasero, 1999)
What is pain? • " Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage. It may be acute or chronic. • Pain is always subjective. Enormous individual differences in response to painful stimuli exist. • (from The Classification of Child and Adolescent Mental Diagnoses in Primary Care: Diagnostic and Statistical Manual for Primary Care (DSMPC) • Child and Adolescent Version, American Academy of Pediatrics, 1996. )
What is Pain? • The pain stimulus is interpreted based on the context or meaning of the pain to the individual, as well as the individual's psychological state, culture, previous experience, and a host of other psychosocial variables.
What is Pain? • As a result, the same noxious stimulus may cause different amounts of pain in different individuals based on personal characteristics. " – (from DSM-PC) Child and Adolescent Version, American Academy of Pediatrics, 1996. )
Let’s review what is Pain • Pain is a signal, – nothing more, – nothing less • ALL PAIN IS REAL • PAIN is PAIN, • Suffering is Optional!
Pathophysiology of Pain • Acute vs Chronic Pain – What is Acute Pain? • brief duration: usually less than 3 months • Identifiable cause / injury / surgery or disease • predictable end • subsides with healing
Pathophysiology of Pain • Acute vs Chronic – What is chronic pain? • Peristent pain lasting longer than 6 months that is generally associated with a prolonged disease process
Pathophysiology of Pain • Nociceptors – Free nerve endings at site of tissue damage – Purpose of nociceptors are to transmit pain impulses along specialized nerve fibers, • the A-delta and C-fibers, to the dorsal horn of the spinal cord • Substantial gelatinosa, aka “gate-keeper” – Regulates transmission of pain and other nerve impulses to the CNS – Located in the dorsal horn of s. c.
Pathophysiology of Pain Jane W. Ball and Ruth C. Bindler Child Health Nursing: Partnering with Children & Families © 2006 by Pearson Education, Inc. Upper Saddle River, New Jersey 07458 All rights reserved.
Pathophysiology of Pain • Brain – Once sensation reaches the brain other factors may influence pain intensity…like what? – Pain signal transmitted through spinal pathways where perception occurs. – Descending tracts can alter perception through the release of inhibitory neurotransmitters
Pathophysiology of Pain • ANS – Activated in response to pain • Tachycardia • Peripheral vasoconstriction • Diaphoresis • Pupil dilation • Increased secretion of catecholamines and adrenocorticoid hormones
Pathophysiology of Pain • Gate Control Theory – Since pain and non-pain impulses are sent along the same pathways, non-pain impulses can compete with pain impulses for transmission
Types of Pain • Nociceptive: stimuli from somatic and visceral structures – somatic: sharp/stinging; superficial dermal or epidermal layers; deep- bones or deeper structures – visceral: abdominal organs, peritoneum and pleura • Neuropathic: stimuli abnormally processed by the nervous system – damage to a nerve - infiltration, compression or infection
Types of Pain • Somatic – Sharp, hot, stinging – Generally well localized – Associated with local and surrounding tenderness
Types of Pain • Visceral – Dull, cramping, colicky, often poorly localized – Tenderness locally or in the area of referred pain – Associated with symptoms such as nausea, sweating and cardiovascular changes
Types of Pain • Neuropathic – Pain descriptors – burning, shooting and stabbing • Dysaesthesia (unpleasant abnormal • sensations) – Hyperalgesia (increase response to a normally painful stimulus) – Allodynia (pain due to a stimulus that does not normally evoke pain eg. light touch)
Physiological consequence of Pain • Affects multiple body systems • (refer to table 18 -1) • Respiratory Changes – Respiratory Alkalosis – Decreased O 2 sats – Retention of secretions
Physiologic Consequences of Pain • Neurological – Increase in HR, blood sugar, cortisol levels, and intracranial pressure (risk for IVH) • Metabolic effects – Increase in fluid and electrolyte losses • Immune System – Increased risk of infection • Gastrointestinal – Impaired functioning
Behavioral Indicators of Pain • Restlessness and agitated or hyper-alert state • Short attention span • Irritability • Facial grimacing, posturing, guarding • Anorexia • Lethargy • Sleep disturbance • Aggression
Assessing Pain in Children • Behavioral Responses and Verbal Descriptions of Pain by Children of Different Developmental Stages • Refer to Table 18 -4 • Children’s Understanding of Pain by Developmental Stages • Refer to Table 18 -3
Myths and Misconceptions around Pain • Active children cannot be in pain • Generally there is a “usual” amount of pain associated with any given procedure • If children are asleep then they are pain free • Giving narcotics to children is addictive and dangerous • Narcotics always depress respiration in children • Infants don’t feel pain • The less analgesia administered to children the better it is for them
Why is Pain Assessment Important? • Provides an avenue for more effective management of pain • Promotes communication between the child, parents and health professionals • Supports evidence based practice • Provides continuity through the hospital • Allows children to indicate the intensity of their pain
Challenges with Assessing Children ! • Lower levels of verbal fluency / nonverbal children • May not verbally communicate presence of pain unless specifically asked • Pain highly individualized • Parents often called upon to provide pain ratings - can be different to patients perspective
Criteria For Selecting A Pain Tool • Established as valid and reliable • Developmentally appropriate • Easily and quickly understood • Liked by patients, families and clinicians • Inexpensive • Appropriate for different languages and culture
The Questt Tool • Question the child • Use pain rating tools • Evaluate behavior and physiological changes • Secure parents involvement • Take the cause of pain into account • Take action and evaluate the results
Pain Assessment Tools • Newborn/ Infant: – CRIES • Developed for use in preterm and ft infants in ICU • Measures crying, O 2 sat, HR, BP, expression and sleeplessness – Neonatal Infant Pain Scale (NIPS) • Evaluates facial expression, cry, breathing, arms, legs and state of arousal – Premature Infant Pain Profile (PIPP) • Gestational age, behavioral state, HR, O 2 sat, brow bulge, eye squeeze, and nasolabial furrow; often used for procedural and post-op pain
CRIES neonatal postoperative Pain Scale • Refer to table 18 -5
NIPS Scale • Refer to table 18 -6 • Recommended for children under 1 year old. • A score of 3 or more= pain
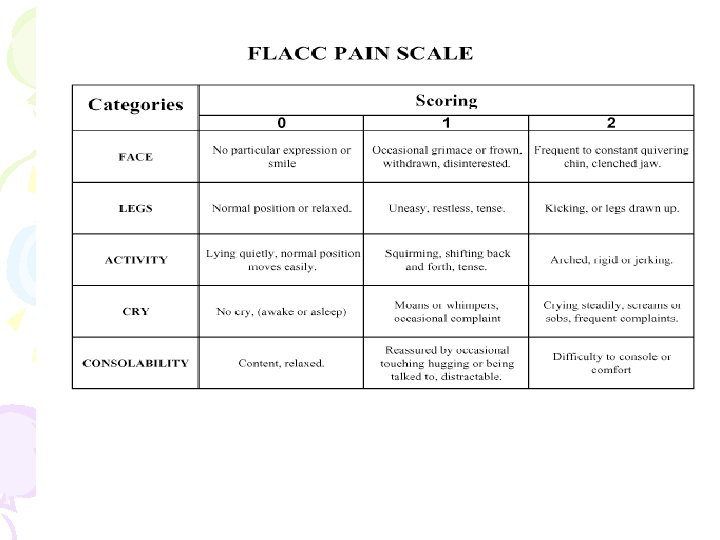
Pain Assessment Tools • Toddler – FLACC – Oucher – Faces pain-rating scale • Preschooler – Oucher – Faces Pain-rating Scale (usually 3 and over) – FLACC • Acronym for face, legs, cry and consolability – Body Outline (3 and over)
Oucher Pain Scale A Jane W. Ball and Ruth C. Bindler Child Health Nursing: Partnering with Children & Families B C © 2006 by Pearson Education, Inc. Upper Saddle River, New Jersey 07458 All rights reserved.
Faces Pain Scale
Pain Assessment Tools • School Age – Numeric Pain Scale (9 yrs- adult) – Oucher – Faces pain-relating scale – Poker chip scale – Work graphic – Visual analogue
Pain Assessment Tools • Adolescent – Numeric Pain Scale – Oucher – Faces Pain-relating scale – Poker chip – Work graphic – Visual analogue – Adolescent pediatric pain tool
Numeric Pain Scale • Numeric Rating Scale – Let’s say 0 means no pain and 10 means the worst pain anyone could have. How much pain do you have? (score 0 -10)
Assessing Readiness for Use of Pain Scales • Refer to Box 18 -3 • Assess a chlid’s language, and understanding of concepts • Children 2 -3 years-old – Understand more or less – No more than 3 choices on pain scale • Only 26% of 5 year olds understand numeric scale – Which number is smaller 4 or 7?
Children with Cognitive Impairment • Assessment of pain difficult • Contribute to inadequate analgesia • Merkel et al (1997) – FLACC scale validated for cognitively impaired children
Case Study • Tom is 10 years old and has severe mucositis after having a BMT. He has a morphine PCA with a background infusion of 1 ml/hr. He is lying very still in bed and is very reluctant to move. His mum does not want him to push the button unless he is really sore, as she has heard that morphine is really addictive. – Who is the best judge of Tom’s pain? – How would you go about assessing Tom’s pain? – What would you tell Tom’s mum if you were his nurse?
Intervention • Pharmacologic and Nonpharmacologic methods of pain control
Pharmacologic Pain Control • Pain Medications include: – Opioids – Nonsteroidal anti-inflammatory drugs (NSAIDs) – Non-narcotic analgesics (acetaminophen)
Pharmacologic Pain Control • Opioids – Ex: morphine, codeine – Often for severe pain – Refer to p 575 for recommended drug dosages and table 18 -8, p 577 for S/Sx of Opioid withdrawal – Naloxone is the reversal agent used for opioid adverse effects (hypotension, respiratory depression)
Pharmacologic Pain Control • NSAIDs and Non-opioid analgesics – Ex of NSAIDS= aspirin, Ibuprofen, Naproxen – Ex of Non-opioid analgesics= acetaminophen • Most commonly used for bone, inflammatory, and connective tissue conditions • NSAIDs and opioids can be used in combo • Remember the differences b/t NSAIDs and acetaminophen! • Refer to p 576 for drug dosages
Nursing Considerations when administering a Pain analgesic • Always document pain level pre and post medication administration • Also document any other nursing interventions and if they were useful
Patient Controlled Analgesia (PCA) • A method of administering IV or epidural analgesic using a computerized pump that is programmed by a healthcare professional and controlled by the child • Children 5 years and older • Children should be able to push the button and understand that this will give them pain relief.
Non-pharmacologic Methods of Pain Control • • • Distraction Hypnosis Imagery Relaxation Comfort measures – Quiet presence – Music massage – Heat/cold – Baths – vibrations
Complimentary Therapies for Pain Control • Refer to p 579 in text • Sucrose solution • Muscle relaxation techniques • Breathing techniques • Electroanalgesia • Biofeedback • Acupucture
Pediatric Considerations in Disaster Preparedness • Impact of disaster – Psychological • General effects • Anxiety • Stress – fear
Pediatric Considerations in Disaster Preparedness • Impact of Disaster – Developmental considerations • Toddler/ preschooler • School age • Adolescent • Responses to Disasters by Children of Different Age Groups – Refer to Table 16 -2 (p 523)
Pediatric Considerations in Disaster Preparedness • Preparedness – Pediatric drugs/ supplies – Advanced planning • Medically fragile in community • Community disaster response systems • Family – Resource package – Anticipatory Guidance
I hope this lecture wasn’t too painful!!