Chest Trauma The Basics Stefan Da Silva CCFPEM
 2009")
Chest Trauma The Basics Stefan Da Silva CCFP(EM) 2009

• Outline • Discuss identification and management of life-threatening chest trauma • Discuss identification and management of potentially lethal chest trauma • Pearls

6 Immediate life-threatening chest trauma injuries • Airway obstruction • Open pneumothorax • Tension pneumothorax • Flail chest • Massive hemothorax • Cardiac tamponade

Management options • Diagnosis: – CLINICAL!! – CXR – EDE – CT chest • Interventions: • • Intubation Chest tube insertion Pericardiocentesis +/- thoracotomy

CXR • Up to 38% of injuries present on CT will be missed on initial CXR • Additional injuries found on CT will require treatment in up to 24% of pts

Physical exam? • • • CXR is better than auscultation. CT better than CXR If stable get imaging. If unstable then tx • eg. pt hypotensive and dying. Chen SC, et al. Accuracy of auscultation in the detection of hemopneumothorax. Eur J Surg. 1998.

Tension pneumothorax • “one-way” valve through hole in lung or chest wall pleura • Air in pleural space causes compression of affected lung, then compression of mediastinum and eventually shift of midline structures • Causes hypoxia, decreased venous return, and finally hypotension

Tension pneumo • Signs/symptoms • Restlessness, CP, SOB • Tachypnea, tachycardia, hypoxia, hypotension • Absent breath sounds, neck vein distension, shift of trachea to contralateral side, hyperresonance to percussion
, midclavicular")
Needle decompression • Landmark: 2 nd intercostal space (superior to 3 rd rib), midclavicular line; or else nipple-line anterior axillary line • Equipment: 16 or 18 G needle (really, that’s all…) • Will need chest tube as definitive management

Open pneumothorax • • • “sucking chest wound” Large defect in chest wall that allows air to pass in and out with each breath Lose chest wall integrity so unable to create intrapleural negative pressure If hole is 2/3 diameter of trachea, air will enter thru chest wall instead of trachea with inspiration S/s: obvious chest wall defect, air heard flowing from wound

Mgmt • Sterile occlusive dressing • Tape on 3 sides over wound • Allows air to escape with exhalation • Do NOT tape all 4 sides as may convert to tension pneumo (BAD!) • Will need definitive chest tube (away from site of defect)

Flail chest • 3+ consecutive ribs fractured in 2 places • Creates floating segment in chest wall • S/s: hypoxia, poor A/E, paradoxical chest movement, bony crepitus

Flail chest • 4 reasons for hypoxia in flail chest? • Underlying lung injury • Pain restricts deep breathing • Paradoxical chest wall movement causes poor A/E • Atelectasis and V/Q mismatching

Mgmt • Oxygen • Intubate and ventilate prn • Pain control
 in pericardial sac which interferes with atrial filling")
Cardiac tamponade • Fluid accumulation (blood) in pericardial sac which interferes with atrial filling and cardiac activity • S/s: Becks triad (hypotension, distended neck veins, muffled heart sounds), pulsus paradoxus • Diagnosed aided with U/S
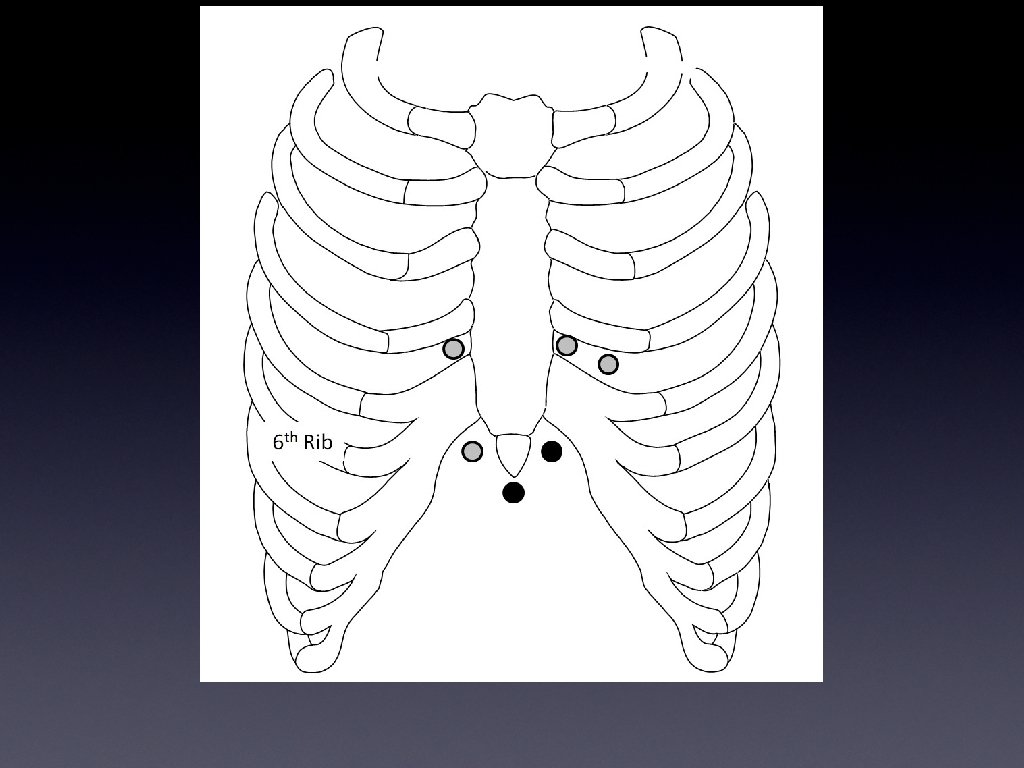

Pericardiocentesis • Removing only 15 -20 cc fluid may improve status • Can do either direct under u/s guidance or indirect (blind)
")
Massive hemothorax • Mortality rate almost doubles if due to blunt trauma (near 40%) • Bear in mind, CXR is an inadequate way to diagnose volume of hemothorax —CT far better; so treat clinical picture, not XR picture!

• • • Indications for thoracotomy Initial chest tube output >20 cc/kg Ongoing bleeding >7 cc/kg/h Increasing hemothorax seen on CXR Continued hypotension despite resuscitation (with no other causes found) Decompensation after initial response to resuscitation penetrating wounds to thorax with loss of vitals signs.

Survival after ED thoracotomy • Signs of life in hospital— 11. 5% • Signs of life in field— 8. 9% • Blunt trauma— 1. 4% • Penetrating trauma— 8. 8% • Gunshot— 4. 3% • Stab— 16. 8% Rhee, et al. Survival after ED thoracotomy: review of published data from the past 25 years. J Am Coll Surg 2000.

Why not ? • Risk of occupational exposures to ED staff • Significant time/personnel investment for dismal outcomes • No surgical backup • ie. you open the chest, fix the wound, resuscitate but no surgeon. . . ? ? ?

Rules • Indications • • • Penetrating thoracic trauma with initial signs of life in field PEA SBP <50 after fluid resus • Contraindications – No qualified surgeon present – Blunt trauma? ? – Dead. . .

Thoracotomy goals • • Pericardiotomy and release of tamponade Repair of cardiac wounds Open cardiac massage Control of major thoracic vessel hemorrhage Cross-clamp aorta Control of bronchovenous fistulas Aspiration of air from RV/LV Internal defib
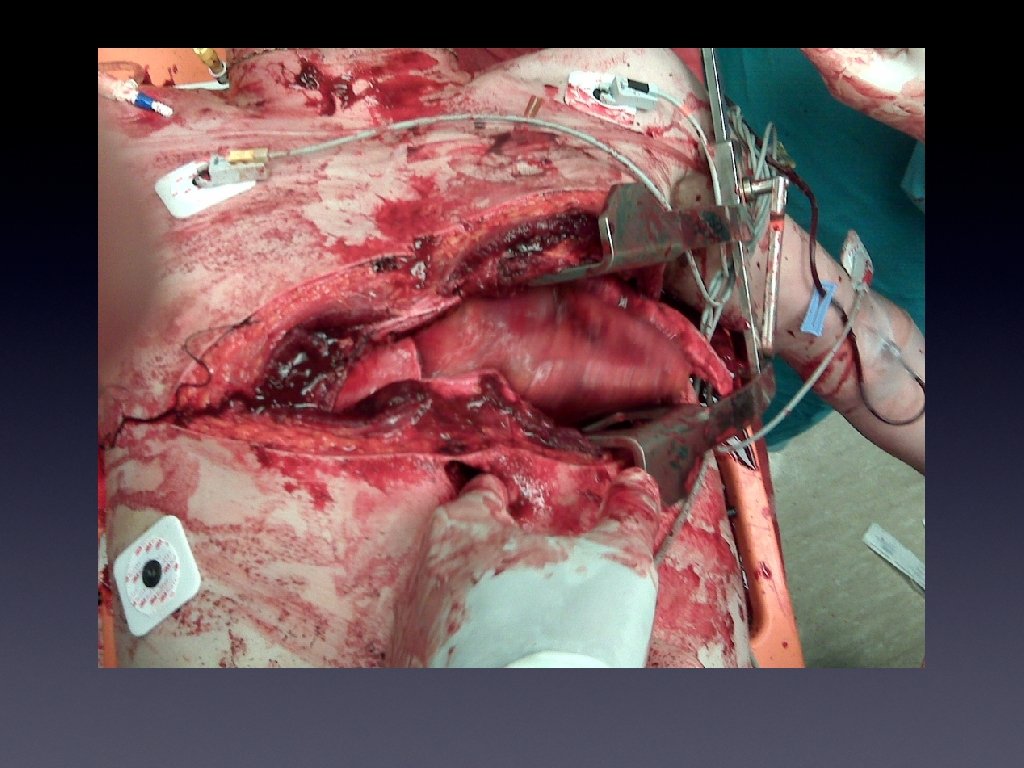

Procedure • • • Intubate—ketamine and roc Prep—quick!! L arm above head, towel under shoulder Incision—cut skin from sternum to post axillary line Open ribs—incise above rib, use scissors to cut intercostals Rib spreader—handle lateral and down Retract left lung Pericardiotomy, deliver heart, repair wounds (staples, sutures, foley) Cross-clamp aorta Control major vessel bleeding Open cardiac massage OR, OR, OR, …

EMR. Thoracic trauma. 2001.

Potentially lethal injuries • • • Simple pneumo Hemothorax Pulm contusion Tracheobronchial tree injury? ? ? Diaphragmatic injury • Aortic disruption • Blunt cardiac injury • Wounds traversing mediastinum

• • • Tracheobronchial injuries Mortality 30% (1/2 of these pts die within first hour) May occur with either penetrating or blunt trauma Sudden deceleration pulls lungs away from mediastinum, causing traction on trachea at the carina ? glottis closed at time of impact causes sudden increase in intrabronchial pressure and rupture of tracheobronchial tree 80% occur within 2. 5 cm of carina

Tracheobronchial injuries • CXR findings: • Bayonet sign (end of ruptured bronchus seen as tapering air-filled structure) • Fallen lung sign (lung torn from bronchus and falls into lower chest) • Massive subq emphysema • Pneumomediastinum

Tracheobronchial injuries • Caution when intubating!!! • Preferably, should be intubated using fiberoptic techniques in OR • Extratracheal placement may occur and result in inability to oxygenate or ventilate, worsen pneumomediastinum

Occult Pneumothorax • Pneumothorax not seen on initial CXR • Suspect in multi-system trauma or significant mechanism • If you suspect it. . . get the CT scan.

Occult Pneumothorax Thanks Heather…

Pulmonary contusion • • • May have no outward signs of trauma Likely due to lung laceration causing alveolar hemorrhage and atelectasis Should appear on CXR within 6 h Maximal hemorrhage will have occurred by 6 hrs Patchy or diffuse air space disease Most common pulmonary injury in adults and peds

Differentiating • Pulmonary contusion • • • Occurs within 4 h Segmental/lobar, asymmetric Lasts 48 h • ARDS – Onset after 24 -48 h – Diffuse, symmetric – Lasts a variable amount of time

Mgmt ? • Supportive: • Cautious IV fluids • Pain relief • No role for antibiotics • No shown benefit with steroids • Aid ventilation: • Bi. PAP • Intubation

Esophageal perforation • Much more common in penetrating trauma • Think of it if you see tracheal injuries or rd th 3 /4 else injuries to T-vertebrae (as they are closely associated) • CXR will show mediastinal air, pleural effusion, pneumothorax, widened mediastinum, air-fluid level in mediastinum

Mgmt • • • Gastrograffin swallow better than barium swallow (diagnose in 62% of cases) Endoscopy more sensitive, but much higher risks of worsening the perforation Surgical exploration, obviously, if other associated injuries IV abx, NGT, immediate surgical consult Without surgical mgmt, mortality is ~50% (mediastinitis)

Diaphragmatic injury • Blunt injury: • • • Left hemidiaphragm more commonly injured (up to 80% of cases) Right hemidiaphragm far less common; and if very small perforation, may not require surgical repair Penetrating injury: • More likely equal distribution between right and left (possibly more left sided injuries as there are more right-sided attackers involved with stab wounds!)

Blunt cardiac injury • • Spectrum of disease that runs from asymptomatic myocardial bruise to myocardial rupture (and often, death) 6 categories: • • BCI with free wall rupture BCI with septal rupture BCI with coronary artery injury BCI with cardiac failure BCI with complex arrhythmias BCI with minor EKG/cardiac enzyme abnormalities Incidence in blunt trauma pts is 20% (again, can be anywhere on the spectrum)

Mechanisms • Direct precordial impact • Crush injury between sternum and spine • Deceleration or torsion causing tear at fixed points (ex: between RA and vena cava) • Hydraulic effect resulting in increasing intracardiac pressure and rupture • Blast injury

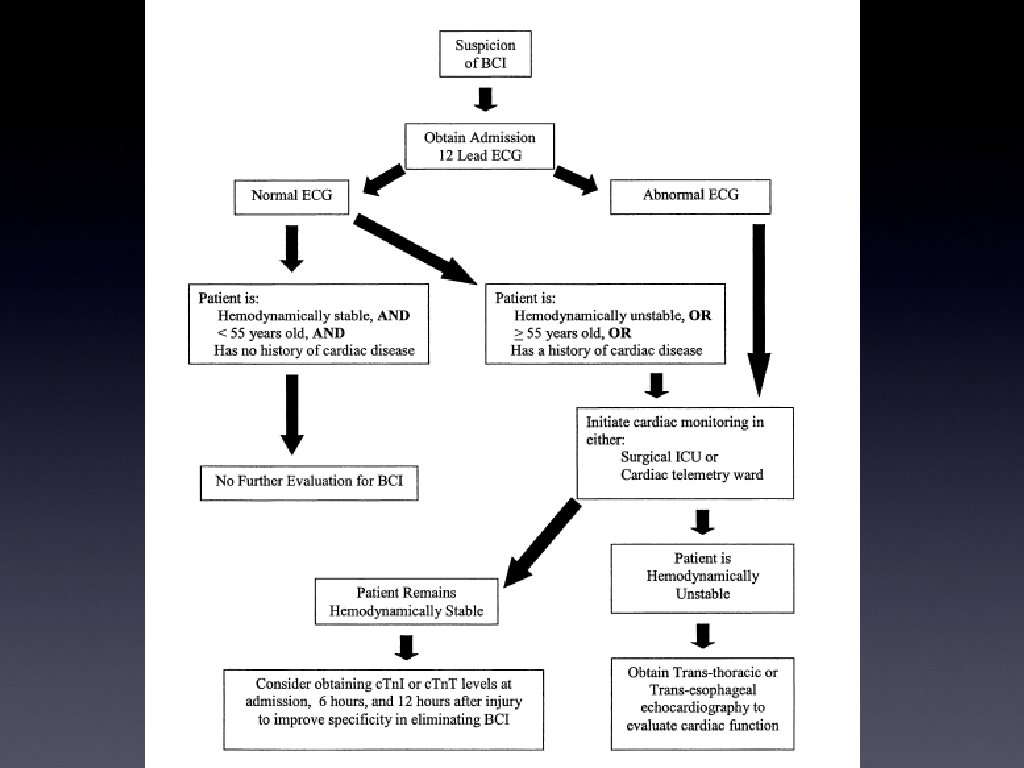
EKG ? • Currently, EKG is reference for BCI and predictor of cardiac complications • Must have no previous cardiac hx • Previously normal EKG • May see dysrhythmias, conduction abnormalities, ST changes

Troponins • • No-BCI complications occurred in presence of normal EKG and normal serial Tn. T However, 6 pts with BCI had abnormal EKG, but a normal Tn. T value Concluded that no role for Tn. T if pt has normal EKG ? Tachycardia?

Aortic disruption • Common mechanism—rapid deceleration • Of those that survive first hour, 90% will die within 4 months • CXR as screening tool

Mechanisms • • • Accounts for up to 15% of MVC deaths Chest strikes steering wheel decelerating forces thru chest vascular compression between thoracic vertebrae and sternum severe intraluminal hypertension Area most susceptible to injury is transition point where transverse arch fixed by arch great vessels, to descending aorta fixed by ligamentum arteriosum and intercostal arteries

Injuries • • Blunt: Focal intimal disruption Partial rupture involving intima and media Transection involving full-thickness aorta • • • Partial Circumferential RARE! • Pentrating: Pseudoanuersyms

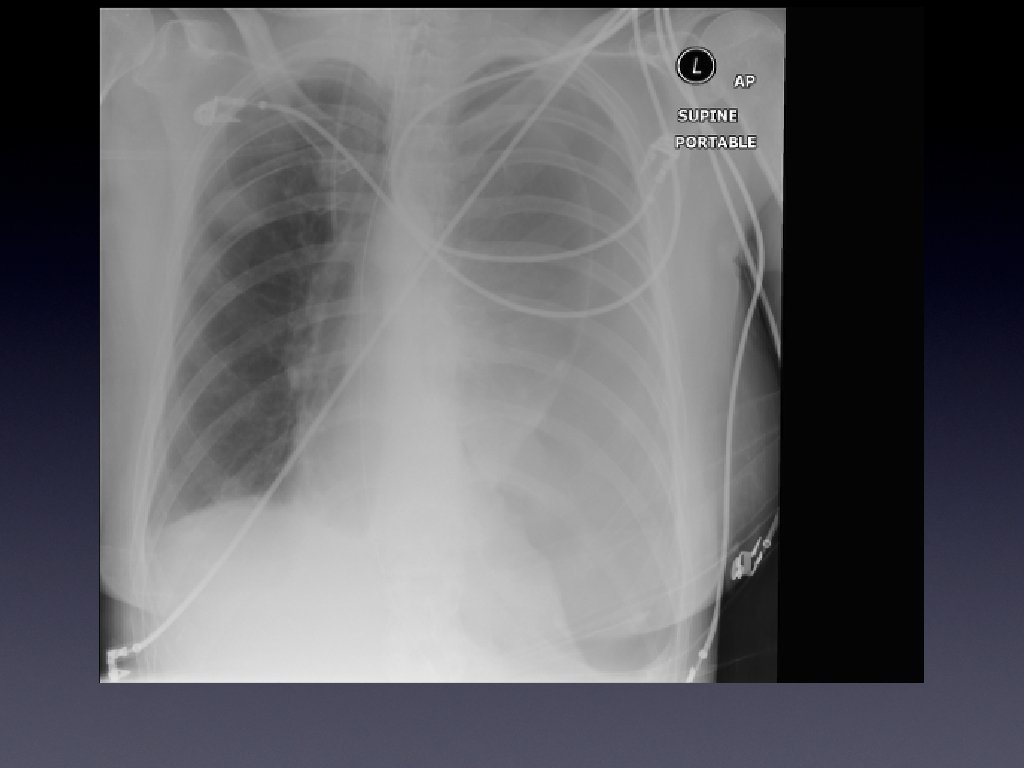
Aortic disruption • CXR findings: • • Widened mediastinum Depressed L mainstem bronchus Deviation of NG tube Lateral displacement of trachea L apical pleural cap Loss of paravertebral pleural stripe Obscured aortic knob Widened paratracheal stripe

Widened mediastinum • >8 cm on supine AP film OR • >7. 5 cm at aortic knob OR • Ratio of mediastinal width to chest width of 0. 38 cm OR • Subjective interpretation of widening

Fractures • • Rib #’s: Make sure there is not a flail chest or pneumo/hemothorax involved! 1 st /2 nd rib #: • • Suspect other injuries… Arteriography if 1 st/2 nd rib # AND: multiple thoracic injuries assoc, distal vascular insuffic, widened mediastinum, large hemothorax, intercostal art injury, brachial plexus injury, significant displacement of #

Fractures • Sternal #—assoc pulmonary, cardiac injuries in up to 6% cases (difficult to diagnose without lat CXR or CT) • Scapular #--in one study up to 43% were missed on initial CXR (but were visible…just not looked for!)

Sternoclavicular Disolcation • Emergent reduction of sternoclavicular dislocation • Towel clamp applied to medial end of affected clavicle and direct pulling force to reduce sternoclavicular joint

Pearls • Treat the patient not the tests • Mechanism, mechanism • Situational vitals • The two A’s: Airway and Access • Find the bullet!! • Recreate the scene and anticipate trajectory.
- Slides: 53