Chemical and Biological Warfare Agents Charles Stewart MD

Chemical and Biological Warfare Agents Charles Stewart MD FACEP

Thinking Out of The Box

Unrestricted warfare “With technological developments being in the process of striving to increase the types of weapons, a breakthrough in our thinking can open up the domain of the weapons kingdom at one stroke. ”

Unrestricted Warfare is a Way of Thinking Out of the Box…

Unrestricted warfare “The new concept of weapons will cause ordinary people and military men alike to be greatly astonished at the fact that commonplace things that are close to them can also become weapons with which to engage in war. We believe that some morning people will awake to discover with surprise that quite a few gentle and kind things have begun to have offensive and lethal characteristics. ”

Unrestricted warfare “It means that all weapons and technology can be superimposed at will, it means that all the boundaries lying between the two worlds of war and non-war, of military and non-military, will be totally destroyed. ”

Unrestricted Warfare Qiao Liang and Wang Xiangsui Beijing: PLA Literature and Arts Publishing House, February 1999

Realism in Theater N N Are we sufficiently prepared for the Right Threats? Some other possible problems ©NIH. –Not invented here ©Media “guidance“ does not actually define a real threat. ©Politicians often “react” and nay not properly plan for real threats ©“Security” may make us less secure ©Simple solutions don’t always solve complex problems.

What Should We Really Plan For? N N N N Explosives Flammable agents Chemical agents Biological Agents Radiological dispersion weapons Nuclear weapons Snipers? All of them are possible threats !

Bombings are still the single most common form of terrorism N N Conventional explosives are easy to get and easy to use. Look for new ways to make and deliver them.

Types of terror attacks? Think Bombs!

Terrorist threat of explosives N Readily available ©Predictable ©Familiar effects ± ± Abundant training available Abundant information available ©No difficulty with delivery

Asymmetric Warfare N Them: © 4 small crews © 100% “ martyrs” N Us: ©More than 4000 direct casualties © 100’s of millions of $$ in damages ©Massive damage to tourism and transportation industries

Law of unintended consequences N Lessons learned ©Big missions can cause big consequences but provoke large responses ©Little missions can cause big consequences with minimal risks ± Anthrax or sniper model attacks ©Does this mean that new incidents will be small in scope with maximum media impact? ± Possibly

Law of unintended consequences N N “Pearl Harbor” syndrome fully activated Secondary losses ©Loss of safe haven ± Afghanistan ± Iraq? ©System degradation ©Financial support degradation

Potential Terrorist Targets N Critical facilities and infrastructure ©Congress ©Presidential staff ©Supreme Court N N N Enclosed spaces Large crowds (high profile events) Facilities of interest to terrorists’ cause

In 2001, They Planned for at Least 3 ?

In 2003, They Chose 3 Targets in Sa

Terrorist threat of snipers N Weapons are readily available in almost all countries ©Predictable ©Effects familiar to EMS ©Absolutely no difficulty with delivery ©High media impact

Terrorist threat of snipers N Look at how two poorly trained and poorly equipped snipers affected 3 states in 2002 © 10 dead, 3 injured ©Think about how two or three teams of well trained snipers would be able to hurt us. ©Has your EMS unit discussed/gamed/planned how to handle this type of terrorism?

Terrorist Threat of Chemical and Biological Agents N Ideal weapons of terrorism ©Easily and cheaply made ©Easily delivered ©Rapidly manufactured ©Technical information not “hot” ©Political effects far beyond local casualties

Terrorist Threat of Incendiary Agents N Readily available ©Predictable ©Familiar effects ± Abundant training available ± Abundant information available ©No difficulty delivering

Terrorist Threat of Nuclear Weapons N Not easily available ©Fairly predictable ©Great difficulty with delivery? ? ©Unfamiliar effects to most EMS ± Abundant training available ± Abundant information available ©Readily detected ? ©Closely controlled

Terrorist Threat of Radiological Weapons N Moderately available ©Fairly predictable ©Unfamiliar effects to most EMS ± ± Abundant training available Abundant information available ©No difficulty with delivery ± Readily detected ± This is the easiest type of terrorism to detect! ©Media hype expected

Radiologic Dispersal Weapons N Great media hype ©Probably a small number of actual casualties ©A quantity of sufficiently radioactive agent to cause real damage must: ± Be set up as a fine particle (ground) ± Transported to the area where it is to be used ± Shielded from detection ©This is not an easy set of tasks

Chemical and biological weapons are simply tools of unrestricted warfare

Terrorist Threat of Chemical Weapons N Moderately available ©Fairly predictable ©Unfamiliar effects to most EMS ? ± Abundant training available ± Abundant information available ± Readily detected ? ? ©No difficulty with delivery

Simplistic solutions? N Decontamination –wash them all down with water? ©Simple, easily implemented solution ©Particularly effective for Sarin

Simplistic solutions? N Neglects fact that hydrolysis is not always effective or beneficial ± Water is not particularly effective for Vx and other oily or thickened Agents? – Thickened Soman was in Russian inventory. ± Vx is hydrolyzed to EA 2192 – Water actually makes VX into a far more toxic and longer lasting substance EA 2192 = Diethyl methylphosphonate, 2 diisopropylaminoethyl mercaptan, ethyl hydrogen methyl-phosphonate, bis(ethylmethylphosphonic)anhydride, bis S- (2 -diisopropylaminoethyl) methylphosphononodithiote.

Simplistic solutions? N Bleach is bad ? ©GRAS – generally recognized as safe! ± Theoretically could consume 4 oz with no ill effects. ± Hundreds of children have done so. ©Bleach is a better decontamination agent than water ± Much more rapid than water ± Known activity against mustard, Soman, and VX-(military evidence in 50’s)

Simplistic solutions? N Water is not particularly effective for mustard ©Europeans found bleach and sodium thiosufate to be more effective N No experience at all with water decontamination of “dusty” agents ©Dusty mustard ©Dusty Soman and Sarin

Decon Shower

Simplistic solutions? N Water will dilute and render safe this substance by lowering the concentration so that no significant downstream damage will occur? ©Sarin – probably -volatile and non persistent ©VX-? ? ? -long lived toxic hydrolysis products ©Soman-? ? ? ©Mustard -? ? ?

Downstream safety ?

Dusty Agents N Combination of a chemical warfare agent with a very finely divided silica or talc powder to make a particulate aerosol N Civilian technology ©Ortho Ant-Stop is an organophosphate in an inert carrier

Dusty mustard N Enhanced penetration of protective equipment ©Goes under MOPP gear ©“May” penetrate Level A PPE ± Insufficient statement N data exists to substantiate this More rapid and enhanced pulmonary effect of mustard on unprotected

Dusty VX –Sarin –Soman N Enhanced penetration of protective equipment ©Goes under MOPP gear ©“May” penetrate Level A PPE* N More rapid and enhanced pulmonary absorption of VX on unprotected ©“May” give a picture more like Sarin* N “May” make Sarin or Soman less volatile* *Insufficient data exists to substantiate this statement

Dusty Agents N Original Solution ©”WHILE EMPHASIZING THAT THERE IS NO EVIDENCE THAT IRAQ HAS DEVELOPED A DUSTY V-AGENT, FATALITIES RANGING FROM 3 TO 38 PERCENT ARE PROJECTED FOR THE SAME CONCENTRATIONS CITED ABOVE FOR TROOPS IN FULL MOPP IF SUCH AN AGENT WERE USED. USE OF THE PONCHO OVER THE MOPP GEAR IS EXPECTED TO REDUCE THESE PROJECTED CASUALTIES TO NEAR ZERO EVEN FOR A DUSTY NERVE AGENT. “

Dusty Agents N N One senses that the prior recommendation was a desperate attempt to offer reassurance and a temporary “solution” for the troops. Certainty, an open flapping poncho would offer no substantial improvement in chemical threat protection

SERPACWA N Better solution took 8 years to develop © Skin Exposure Reduction Paste Against Chemical Warfare Agents © Paste contains a perfluoroalkylpolyether (PFAPE) oil as a base polymer and polytetrafluoroethylene (Teflon polymer) dispersed within the base oil N ATSP soon to come

Simplistic solutions? N Everybody needs to be in Level A-B-C gear for personal protection ©Governmental recommendations? ± OSHA? ± OPP gear is, at best, level C protection – Splash-Resistant over suit – Purified air (Negative Pressure) Protective mask ± Turn-out gear +SCBA = 30 minutes protection? I don’t know the “ Right” answer to this question.

MOPP

Chemical Threats –NIH Problem N What is best cyanide antidote? ©? Lilly cyanide kit? ± Expensive ± Awkward to use ± Dangerous to peds

Chemical Threats –NIH Problem ©Hydroxycobalamin ± Nl. H? ± Vitamin B 12 ± Widely available and quite cheap ± Not FDA approved for this ©Kelocyanor? ± NIH? ± Available ± Pricy? and widely used in Europe

Terrorist Threat of Biowar Agents N We were assured that biological agents were poor weapons of terrorism? ? ©Unpredictable ± Weather ± Lifespan (survivability) ? ± Few good studies on effectiveness ©Stigma ©Difficulty with delivery ? ?

Terrorist Threat of Biowar Agents N We were assured that biological agents were poor weapons of terrorism? ? ©Unpredictable ± Weather ± Lifespan (survivability) ? ± Few good studies on effectiveness ©Stigma ©Difficulty with delivery ? ?

We Were Expecting “ The Big One”. . .

We Got … N Historically most episodes of terrorism are rather small affairs… ©This is a principle of asymmetric warfare… ©Think about the confusion generated by …
 ©Perpetrator")
Why Bioweapons? Other Advantages N N Undetectable by usual means Remote effect (time-lag) ©Perpetrator can leave scene ©Widespread effect before discovery N Flexible ©Covert vs Overt ©Small scale vs large scale ± Small amounts can inspire significant terror

Real Threat…or Fancy Fiction N Delivery will be a problem? ? ?

Real Threat…or Fancy Fiction N Terrorists need more expertise than they’ve got? ? ? Larry Wayne Harris

Real Threat…or Fancy Fiction N You just can’t get these bugs anymore…. ©(we have controls, you know)? ? ? Endemic source of plague in western USA

Real Threat…or Fancy Fiction N High lethality does not mean a large number of deaths? ? ? Remains to be proven.

Biowarfare Agent Sources N N N Home production Laboratory / commercial production Industrial facilities Foreign military sources Medical / university research facilities

History N Romans ©Used dead animals to foul water supply N Mongols ©Catapulted plague victims into Kaffa N English ©Gave smallpox infested blankets to Indians during French-English war in colonies.

History: German Agents in WWI N Dr. Alton Dilger in Washington DC ©Anthrax and Glanders ©About 3500 horses infected ©More people died than from the 2001 anthrax
 produces anthrax and")
History - Terrorist N N N 1915 Dr. A Dilger (German-American) produces anthrax and glanders 1972 ‘Order of the Rising Sun’ prepares 30 kg of typhoid bacteria cultures 1978 Giorgi Markov assassinated with ricin

History - Unit 731 N N 1918 - Unit 731 established in Japan Unit 731 deploys in Manchuria in WWII ± Investigates plague multiple organisms including © 1941 Bubonic plague sprayed in China by Japanese © 1942 Bacterial “bombs” used by Japanese

History - USA Experiments N 1950 -1969 Off coast USA – ©Experiments with Serratia ± US Army and Navy ± for several cities including San Francisco and LA N 1966 Bacillus subtilis via subway route in NYC ± US N Army 1966 Pentagon ‘bombed’ by Chemical Corps

History: A Salad Bar in Oregon N 1984 Rajneesh cult seeds salad bars in Oregon with typhoid to influence an election
 Russia 1979 ©Accidental military")
Anthrax N N Known experience with this agent Sverdlovsk (Ekatrinburg) Russia 1979 ©Accidental military release ©We will talk about this later.

History N N 1983 2 brothers in Northeastern USA produce 1 ounce of pure ricin 1984 Red Army Faction found with botulinum toxin in Paris

History N N 1991 Iraq bioweapons program uncovered during Gulf War 1992 Ken Alibek defects to USA and exposes the Soviet program Ladies and gentlemen… we have a real problem.

History N 2001 Anthrax used via postal delivery methods…. Osma Bin Laden suspected.

History N Sort of puts the lie to anybody who thinks this ain’t gonna happen here …

Asymmetric Warfare N We need to be prepared for the next phase… and we don’t know what that phase is or when it will occur. ©We aren’t ready for a lot of these problems
, coccidioidomycosis (San")
Possible Biologic Agents anthrax, cryptococcosis, escherichia coli, haemophilus influenzae, brucellosis (undulant fever), coccidioidomycosis (San Joaquin Valley or desert fever), psittacosis (parrot fever), yersina pestis (the Black Death of the 14 th Century), tularemia (rabbit fever), malaria, cholera, typhoid, bubonic plague, cobra venom, shellfish toxin, botulinal toxin, saxitoxin, ricin, smallpox, shigella flexneri, s. dysenteriae (Shiga bacillus), salmonella, staphylococcus enterotoxin B, hemorrhagic fever, Venezuelan equine encephalitis, histoplasma capsulatum, pneumonic plague, West Nile fever, Rocky Mountain spotted fever, dengue fever, Rift Valley fever, diptheria, melioidosis, glanders, tuberculosis, infectious hepatitus, encephalitides, blastomycosis, nocardiosis, yellow fever, typhus, tricothecene mycotoxin, aflatoxin, and Q fever. Who knows?

Possible Biologic Agents N The CDC “master list” ©A compromise between ±A limited budget ± Public /media fears ± Agents known to hove been developed as warfare agents ©Does not cover all threats! ±A growing threat ± New and emerging diseases not listed

Detection of Outbreak N N Epidemiologic investigation Syndrome Based ©Inhalation anthrax

BW - Epidemiologic Clues N N N Large epidemic with high illness and death rate Infection non-endemic for region Multiple, simultaneous outbreaks Multi-drug-resistant pathogens Sick or dead animals

BW - Epidemiologic Clues… N N Delivery vehicle or vector found Intelligence of possible event

BW - Epidemiological Information N N Travel history Infectious contacts Employment history Activities over the preceding 3 to 5 days

Aerosol Spread N Ideal aerosol is a homogeneous population of 2 or 3 micron particulates ©This is the best “suspension” of particles for RESPIRATORY spread ©Please note that other sizes may well be infective also. N Maximum human respiratory infection is a particle within 1 to 5 micron size

Aerosol / Infectivity Relationship Infection Severity Particle Size Less Severe 18 -20 15 -18 7 -12 4 -6 (bronchioles) More Severe 1 -5 (alveoli)

Delivery Systems N Airborne

Biological Agents - Types and Characteristics N N Live Agents Biotoxins ©These are more like chemical warfare agents

Possible Live Biowarfare Agents N N N Viruses Rickettsia Bacteria Fungi ? ? Prions ? ? (mad cow disease)

Anthrax

Anthrax N Anthrax is an acute infectious disease of animals caused by Bacillus anthracis. ©Gram positive rods ©Spore forming © May persist in soil for over 50 years!
")
Anthrax N Humans can develop infection from handling contaminated fluids or hides ©(“Woolsorters Disease”)

Anthrax N Spores can be produced in a dry form for biological warfare ©may be stored and ground into particles. ©When inhaled by humans, these particles cause respiratory failure and death within a week.

Anthrax N It is rare to find infected animals in the United States. . N Most United States cases are in Texas, Louisiana, Mississippi, Oklahoma and South Dakota.

Anthrax N Anthrax is most common in underdeveloped agricultural regions N South and Central America N Southern and Eastern Europe N Asia, Africa, N the Caribbean N the Middle East.
 - most common ©inhalation ©gastrointestinal")
Anthrax N 3 forms of Anthrax infection ©cutaneous (skin) - most common ©inhalation ©gastrointestinal

Anthrax - Pathogenesis N Virulent bacteria produce toxins ©edema factor ©lethal factor N Spores are ingested by WBC’s and travel to the regional lymph nodes

Cutaneous Anthrax N Cutaneous ©Vesicle ©Ulcerates with black necrotic center ©Regional lymphadenopathy N Untreated skin infection - 20% mortality if septicemia develops (treated 1%)

Cutaneous Anthrax

Inhalation Anthrax N Initial symptoms like a viral syndrome © 1 to 6 -day incubation period followed by fever, myalgias, cough, and fatigue ©Often get better for short time N Initial improvement is followed by abrupt onset of respiratory distress, shock, and death in 24 to 36 hours

Inhalation Anthrax Chest x-ray shows a widened mediastinum with or without a bloody pleural effusion

Inhalation Anthrax N Inhaled anthrax causes mediastinitis ©Germinated bacteria travel to regional lymph nodes N 50 % of cases have associated hemorrhagic meningitis

Anthrax Meningitis

Intestinal Anthrax N Consumption of contaminated meat ©Inflammation of the intestinal tract ©Nausea, loss of appetite, vomiting, fever ©Abdominal pain, bloody vomit, and diarrhea N Death in 25% to 60% of cases

Anthrax N Biowarfare agent ©Does not spread person to person ©Spores may be spread with multiple types of equipment ©Prophylaxis is possible ©Cheap and easy to produce ©Readily available

Anthrax Transmission N N No documented person-to-person transmission of inhalation anthrax has ever occurred Cutaneous transmission is possible ©Universal precautions required

Inhalation Anthrax - Diagnosis N Nonspecific symptoms ©Fever, headache, malaise N N Substernal chest pain Sudden onset of respiratory distress ©Widened mediastinum on chest x-ray ©Hemorrhagic mediastinitis N Some patients may present with GI or cutaneous anthrax

Inhalation Anthrax - Diagnosis N N Emergency physicians are “first responders” in this disease. This is contrary to usual EMS thinking ©But the “ first response “ for patients with initial complaints of malaise, fever, headache probably won’t occur in the field. N The first Anthrax diagnosis was made by emergency physicians

Anthrax -diagnosis N Nasal swabs ©Poor way to check asymptomatic folks N Gram stain of blood ©Often too late for inhalation disease N ELISA and immunohistology testing may confirm diagnosis but samples must go to reference laboratory for cultures

Anthrax - Prophylaxis N Anthrax vaccine ©Cell free filtrate ©Proven for cutaneous ©Not proven for inhalation or massive exposures. ©Requires 6 injections ©Requires yearly booster

Anthrax - Prophylaxis N Unimmunized persons ©Cipro 500 bid PO ± No reason why another quinolone would not be effective. ©Doxycycline 100 bid PO ©? ? Penicillin ©Continue antibiotics for 4 weeks at a minimum ©Vaccinate!

Anthrax - Therapy N Penicillin ©Resistance is easy to achieve N N N Cipro Chloramphenicol Doxycycline ©Tetracycline N Erythromycin

Anthrax - Pediatric Treatment N Prophylaxis ©Penicillin ©Doxycycline ©? Cipro N IV Therapy ©Penicillin ©? Cipro ©Doxycycline
 Russia 1979 Accidental")
Anthrax N N N Known experience with this agent Sverdlovsk (Ekatrinburg) Russia 1979 Accidental military release

Sverdlovsk = Ekaterinburg

Anthrax - Sverdlovsk N This accident resulted in over 66 deaths downwind. Biological Warfare research, production and storage facility Path of airborne Anthrax – over 20 kilometers downwind

Inhalation Anthrax is a slow infection Exposure 0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 16 18 20 22 24 26 28 30 32 34 1979 Sverdlovsk deaths… per day after exposure Each represents one death 36 38 40 42 43

Current experience N N We still don’t know who did this. The technology could still be reused? ? ?
 pestis ©The Black Death - Bubonic plague ©Flea bite ±")
Plague N Yersinia (Pasturella) pestis ©The Black Death - Bubonic plague ©Flea bite ± Found worldwide ± Prairie dogs in Rocky Mountain areas N Bipolar gram-negative rod

Plague N 3 Presentations ©Bubonic ©Septic ©Respiratory

Plague - bubonic N N Usual natural transmission form Localized abscess at site of infection Regional lymph glands form large abscesses Incubation 2 -10 days

Plague Disease Complex Fever/rigors Inhalational Pharyngitis 2 -3 Sudden days onset Fever, URI syndrome APTT ecchymosis DIC Tender bubo 1 - 10 cm 9% 24 hrs Liver enzymes Fulminant Pneumonia 6% late meningitis Stridor, cyanosis, productive cough, bilateral infiltrates Leukemoid reaction Gram negative rods in sputum Erythema 2 - 10 days Systemic Toxicity Respiratory failure & circulatory collapse

Bubonic Plague N N N Erythema, fever, rigors Bubo formation in regional lymph nodes Bubo aspiration and gram stain is diagnostic

Plague - pneumonic N N N Aerosol transmission Highly lethal Rapid infection (1 -2 days)

Plague - pneumonic N N 2 to 3 day incubation period followed by high fever, myalgias, chills, headache, and cough with bloody sputum Pneumonia and sepsis develop acutely and may be fulminant ©Patients develop dyspnea, stridor, cyanosis, and circulatory collapse

Plague – pneumonic N Patchy infiltrates or consolidation seen on chest x-ray

Plague - septic N Blood-borne spread from other sites to lungs, CNS and other sites ©Highly lethal ©Often has features of pneumonic but slower onset

Acral Gangrene N N Late complication of pneumonic or septicemic plague May occur in the fingers, toes, earlobes, nose, or penis.

Plague - diagnosis N N Clinical suspicion Lymph node aspirate ©Gram stain N N Check sputum and CSF too…. Culture of the aspirate, sputum, CSF, or blood

Plague N N Therapy must be started rapidly! Streptomycin (30 mg/kg/day IM divided BID for 10 days) Doxycycline (100 mg IV BID for 10 days) Chloramphenicol for plague meningitis

Plague - Pediatric Treatment N Prophylaxis ©Doxycycline ©Trimethoprim/Sulfamethoxazole N IV Therapy ©Streptomycin (over 1 year of age) ©Gentamicin ©Chloramphenicol

Plague - prophylaxis N N Vaccine is available… but it won’t protect against aerosol spread… ©Vaccine effective only for bubonic plague Prophylactic doxycycline will ‘probably’ be effective if started prior to exposure. . .

Plague - Prophylaxis N Secondary transmission is possible and likely N Universal and aerosol precautions until ©sputum cultures are negative ©pneumonic plague is excluded

Plague - prophylaxis N Strict isolation is important for plague victims… ©Respiratory isolation is mandatory for the first 48 hours of treatment ©Violent coughing easily spreads infected sputum N Vector control is important to prevent infection of local fleas and rodents.

Plague N N This agent is not an ideal war bug. . . but it is readily available, has limited spread, and is relatively hardy. It would cause substantial casualties. It has the potential of infecting local fleas and rodents as a persistent agent. ©It was used in WWII as a warfare agent

Tularemia N N N Incubation 2 -10 days Oculoglandular Typhoidal Treatment: gentamicin Prophylaxis: vaccine (experimental) or 2 weeks of tetracycline

Smallpox N N Variola virus Extinct? © 2 ‘legal’ repositories known ± US and Russia ± Russia developed military stocks of smallpox ©Monkeypox, cowpox, and ‘chickenpox’ are quite similar ©May lend to genetic manipulation ± Or just selection of a specific variant

Smallpox Last known natural smallpox victim Ali Maalim Somalia 1977

Smallpox - presentation N N N Incubation period 12 -14 days Prodromal period Skin lesions ©Uniform progression of the lesions ©Rash looks like chickenpox lesions only uniform N N Healing in 1 -2 weeks Fatal in 30% of cases (Variola major)

Smallpox …comes in more thon one variant N N N Variola major … 30% mortality Variola minor … 5% mortality Variola “hemorrhagic variant” ©mortality unknown …probably >70% N Variola “flat variant “ ©mortality unknown …probably >50%

Smallpox N N N Diagnosis by clinical examination Electron microscopy Viral culture

Smallpox N N Therapy is supportive Would antiviral drugs…work? ©There are some drugs that appear to have appropriate effect in animal studies, but these are in short supply

Child with Smallpox rash CDC/Cheryl Tryon

Smallpox N Prophylaxis ©Vaccine is available and very effective. ± Jenner ©Vaccinia immune globulin ± Role is unclear ± Used for treatment of vaccina reactions

Smallpox rash close-up CDC/James Hicks, 1973

Smallpox N N All material used in patient care should be burned or autoclaved Considerable potential for person-toperson spread

Smallpox - prophylaxis N N Quarantined all contacts for at least 17 days Infectious until all scabs are healed over

Smallpox N Has already been used in warfare ©British use of smallpox infested blankets for Indians

Last child with Smallpox CDC

Smallpox N Current plan is to encircle an outbreak of small pox wit

Smallpox N Ring system requires ©A group of health care providers who are already immunized. ©Rapid identification of cases ©Isolation of the suspected cases

Smallpox ring system requires N N Contact tracing Massive immunizations Isolated outbreak Effective immunization (prevents disease)

Smallpox N Ring system assumes ©Folks will not refuse vaccination ©Resources are not exhausted ©Quarantine will be observed. © 1: 3 -1: 5 infectivity

What about O’ Hara ? N Any major airport ©Agent release or infected person ©High travel season N Widespread infection ©Infection date may not be known ©Contact tracing difficult ©Look at SARS

Smallpox N Ring system assumes that immunization will be effective b

But… will it be “ blackpox “ N The smallpox variant developed by the Russians was a hemorrhagic smallpox (This type of smallpox is sometimes called” blackpox” because of the massive subcutaneous hemorrhage found in these patients ) N Vozozhdeniye Island in Aral Sea was site of a presumed accidental release in 1971
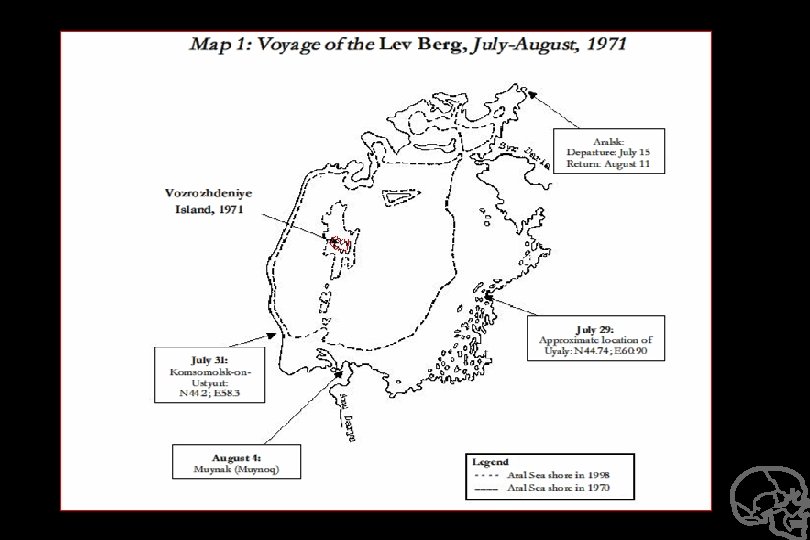

Aralsk smallpox outbreak Patient # Age Sex Date of onset Type of Rash Prior Vacc Dead vs live 1 24 F 8/17 Classic Yes Rec 2 9 M 8/27 Classic Yes Rec 3 23 F 9/10 Hemorrhagic No † 4 36 F 9/10 Classic Yes Rec 5 5. 5 M 9/18 Classic Yes Rec 6 38 M 9/24 Mild Yes Rec 7 0. 8 M 9/26 Hemorrhagic No † 8 60 F 9/26 Mild Yes x 3 Rec 9 33 M 9/28 Mild Yes Rec 10 0. 33 F 10/2 Hemorrhagic No † The Aralsk smallpox epidemic in 1971 was a presumed weapon release from Vozozhdeniye Island in the Aral Sea.

Smallpox –blackpox variant N Ring Strategy would not stop spread of this form of disease ©It was not protective against getting the disease. N Vaccination is protective against death in black pox ©Massive immunization would decrease mortality © 100% mortality in unimmunized. N Note: Data about this variant of smallpox is scanty and may well not be this grim

What about the Toronto model ? N SARS ©Health care system devastated ©Resources exhausted ©EMS shut down N This is for a disease with 10% mortality

Monkeypox Virus

Viral hemorrhagic fever Fever, myalgias, prostration N Target organ is the vascular bed. N ©Conjunctival injection, petechial hemorrhage, and hypotension ©Followed by shock and generalized hemorrhage

Ebola virus N N Viral Hemorrhagic fever No known therapy ©Some antisera may…be effective N No known prophylaxis

VHF N Mortality varies © 50 - 80% Ebola Zaire Abnormal renal and liver function tests - poor prognosis N Disease severity and survival depends on various host factors N

VHF Treatment N Hemodynamic resuscitation and monitoring ©Invasive Swan Gantz catheter as feasible N Careful fluid management ©use of colloid N Vasopressors and cardiotonic drugs

VHF Treatment N N N Cautious sedation and analgesia No anti-platelet drugs or IM injections Coagulation studies and replacement of clotting factors / platelet transfusions

Prevention of VHF N Single room w/ adjoining anteroom as only entrance ©handwashing facility with decontamination solution N Negative air pressure if possible

Prevention of VHF N Strict barrier precautions ©gloves, gown, mask. shoe covers, protective eyeware/faceshield ©consider HEPA respirator for prominent hemorrhage, vomiting, diarrhea, cough N There is no effective vaccine at this time.

Ebola Case Study 1995 N April 5 - Zaire laboratory worker © fever and bloody diarrhea N May 17 - 93 cases - 92% fatality ©most cases were in health care providers N June 25 - 296 cases N When institutional barrier precautions were implemented by WHO/CDC - the infection rate among health care workers dramatically decreased.

Possible biotoxins N N N N Botulinum Clostridia Ricin Saxitoxin Tetrodotoxin Staphylococcal enterotoxin Tricothecene mycotoxins
 Anaerobic spore forming bacterium ©Canned foods ©GI")
Botulinum toxins N N Seven species (A-G) Anaerobic spore forming bacterium ©Canned foods ©GI tract ©Wounds N Aerosol of toxin ©Lethal toxin

Botulinum toxins Clostridum botulinum

Botulinum toxins N Signs and symptoms ©Ptosis ©Diplopia ©Dysphagia ©Dysphonia ©Flaccid paralysis ©Respiratory failure

Botulinum toxins N Diagnosis ©No available rapid laboratory diagnosis ± Assay exists… but is only good for confirmation ± Takes a while to return the results…. ©Suspect if numerous casualties develop bulbar paralysis, muscle weakness, and respiratory failure

Botulinum toxins N Treatment ©Supportive care ± Intubation ± Ventilation ©Trivalent antitoxin (A, B, E) ± Horse serum ± Must be given as soon as possible ©Heptavalent USAMRIID antitoxin ± Investigational horse serum
 ± Investigational product ±")
Botulinum toxins N Prophylaxis ©Toxoid (A, B, C, D, E) ± Investigational product ± 3 x injections with yearly booster ± High risk of exposure

Botulinum toxins N Decontamination ©Was with bleach or soap and water ©Pressure cook all foods ©Toxin does not go through skin

Botulinum N Outbreak control ©Immediate release ± Rapidly decontaminated ©Late contamination ± Boil for 10 minutes

Ok… Why haven’t we seen. . . N Unpredictable ©Collateral damage ©Moral qualms? ? ? N N Personal safety Severe response ©Damage cause ©Out of control ©? ? Deny responsibility

Why haven’t we seen. . N N Higher authority says no. . . Present day tactics are successful Lack of precedent Can’t get credit for the. . .

Delivery Systems – Improv N The ‘experts’ have constantly pointed out that biowarfare can’t be used by “unsophisticated” folks. ©You need a lot of training to effectively use biowarfare ©You need a lot of equipment to make biowarfare agents effective ©Aum Shin tried it and failed (before sarin).

Bioterrorism N Obviously this line of reasoning didn’t stop the current terrorists from using anthrax

Delivery system … crude, but very effective for terrorism… and not very expensive

Delivery Systems - Improv N It depends on just what you want to accomplish… ©English with smallpox and blankets during French & Indian War ©Letter ‘biobombs’ ©Other improv devices

Terrorism is changing N N Increased security about other means Increase in spectacular and/or high casualty events ©NYC and Pentagon N N Increase in state sponsorship Increase in religious sponsorship ©`Everybody who doesn’t worship my way deserves to die!”

And biotechnology is changing. . . N N Dual use technology is burgeoning Gene sequences are becoming public knowledge Increased availability of information Private hire of former Soviet scientists

Foreign Outlook on the US is changing N N N The “last” superpower Jealousy of our freedom and lifestyle The great Satan ©Imposing ‘Our’ view and religions ©A fickle bully ©A place where ± TV makes the decisions and is constantly present ± The soft and decadent live in the US

The Changing Role of the US ©Decrease in international stability leads to increase use of US forces as police ©Retribution / Retaliation cycle of current ‘wars’ in Afghanistan and Iraq

In Topoff II, we trained at 2 major places…

Topoff II N Pre-arranged ©Date and location known ©Compressed time format N N N Limited scope Limited # of patients No significant disruption of normal medical services

What if every yellow spot were a biological release. .

Please remember N Sophisticated planning of simultaneous attacks on multiple targets ©Detailed knowledge of system weaknesses ©Understand employ media to best effect N N Use of unusual “tools” to achieve high casualties and shock effect Self-sacrifice (martyr) can be expected

Who? N N Undefined constituency and/or vague objectives Prior pattern of high casualty incidents ©Sophisticated planning of simultaneous attacks on multiple targets N N N Demonstration of sophistication Willing to take risks ? ? State sponsorship

OBL?

Who else N N OBL or a successor? Palestine ©PLF-GC ©Abu Nidal N N Saddam or a successor ? United States Aryan Nations ©Neo-Nazi groups? N N N Japanese Red Army Hizbollah Sikh

Who will reap the whirlwind? ? ?
- Slides: 186