CHAPTER VIII HOST PARASITE RELATIONSHIP ACKNOWLEDGMENT ADDIS ABABA

CHAPTER VIII HOST PARASITE RELATIONSHIP

ACKNOWLEDGMENT • • ADDIS ABABA UNIVERSITY JIMMA UNIVERSITY HAWASSA UNIVERSITY HARAMAYA UNIVERSITY OF GONDAR AMERICAN SOCIETY OF CLINICAL PATHOLOGY CDC- Ethiopia

Definition: It is a beneficial or harmful relationship between the host and the parasite. Ø On the basis of their life habits, microorganism is classified as saprophytes or parasites. Saprophytes : Mode of life of free-living organisms which obtain their nourishment from soil and water. Saprophytes in general do not require a living host. Parasites: organisms living on or in other higher organisms.

The association may take one of the three forms: 1. Symbiosis: The ability to live in the tissues of the host with mutual benefit. Neither of them are harmed. 2. Commensalism: The ability to live on the external or internal surface of the body with out causing disease. “Eating at the same table” 3. parasitism: one ( the host) is harmed and the other(the parasite ) is benefited. 4. Pathogenicity: The ability of an organism to cause disease. The outcome of the host- parasite relationship depends on a balance between - the virulence of the parasite and - the resistance of the host.

General Concepts Host Susceptibility • Resistance to bacterial infections is enhanced by phagocytic cells and an intact immune system. Initial resistance is due to nonspecific mechanisms. • Specific immunity develops over time. Susceptibility to some infections is higher in the very young and the very old and in immunosuppressed patients.

• Bacterial Infectivity Bacterial infectivity results from a disturbance in the balance between bacterial virulence and host resistance. The "objective" of bacteria is to multiply rather than to cause disease; it is in the best interest of the bacteria not to kill the host.

Host Resistance • Numerous physical and chemical attributes of the host protect against bacterial infection. • These defenses include the antibacterial factors in secretions covering mucosal surfaces and rapid rate of replacement of skin and mucosal epithelial cells. Once the surface of the body is penetrated, bacteria encounter an environment virtually devoid of free iron needed for growth, which requires many of them to scavenge for this essential element.

• Bacteria invading tissues encounter phagocytic cells that recognize them as foreign, and through a complex signaling mechanism involving interleukins, and complement, mediate an inflammatory response in which many lymphoid cells participate.

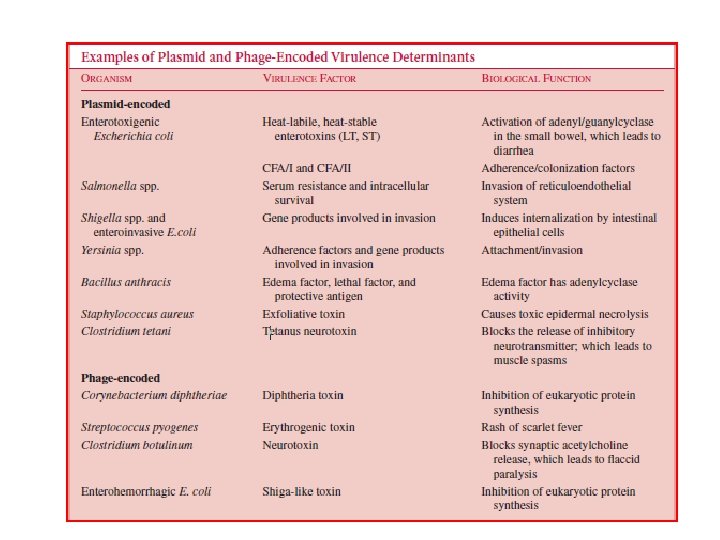
Genetic and Molecular Basis for Virulence • Bacterial virulence factors may be encoded on chromosomal, plasmid, transposon, or temperate bacteriophage DNA; virulence factor genes on transposons or temperate bacteriophage DNA may integrate into the bacterial chromosome.

FIGURE: Mechanisms of acquiring bacterial virulence genes.

Table: Genetic basis for virulence selected bacterial pathogens
, tissue damage results from")
Host-Mediated Pathogenesis • In certain infections (e. g. , tuberculosis), tissue damage results from the toxic mediators released by lymphoid cells rather than from bacterial toxins.

FIGURE: Generalized mechanisms of bacterial pathogenesis: bacteria-induced toxicity or host-mediated damage.
 can grow only")
• Intracellular Growth Some bacteria (e. g. , Rickettsia species) can grow only within eukaryotic cells, whereas others (e. g. , Salmonella species) invade cells but do not require them for growth. Most pathogenic bacteria multiply in tissue fluids and not in host cells. • Virulence Factors Virulence factors help bacteria to (1) invade the host, (2) cause disease, and (3) evade host defenses.

FIGUR: Examples of pathogenic bacteria, indicating their preferred growth phase within the host. (ETEC: enterotoxigenic E coli)

The following are types of virulence factors: • Adherence Factors: Many pathogenic bacteria colonize mucosal sites by using pili (fimbriae) to adhere to cells.

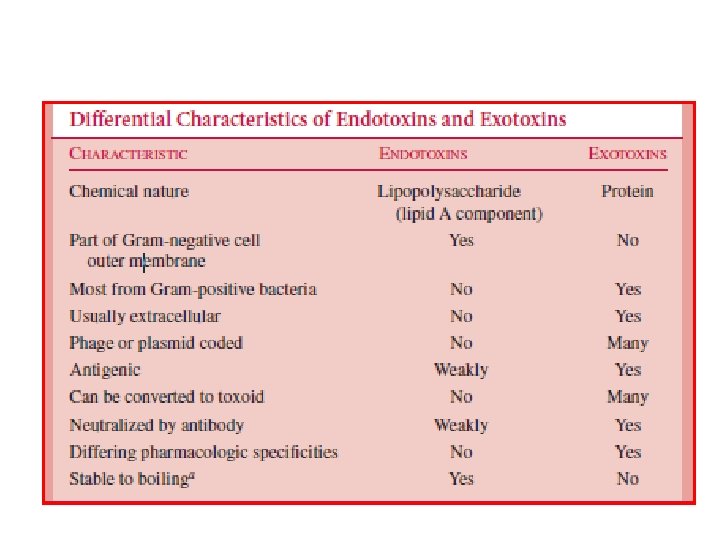
• Invasion Factors: Surface components that allow the bacterium to invade host cells can be encoded on plasmids, but more often are on the chromosome. – Capsules: Many bacteria are surrounded by capsules that protect them from opsonization and phagocytosis. – Endotoxins: The lipopolysaccharide endotoxins on Gram-negative bacteria cause fever, changes in blood pressure, inflammation, lethal shock, and many other toxic events.
 from Gramnegative bacteria.")
FIGURE: Basic structure of endotoxin (lipopolysaccharide) from Gramnegative bacteria.

Table : Multiple biologic activities exhibited by the lipid component of endotoxin

– Exotoxins: Exotoxins include several types of protein toxins and enzymes produced and/or secreted from pathogenic bacteria. Major categories include cytotoxins, neurotoxins, and enterotoxins. – Siderophores: Siderophores are iron-binding factors that allow some bacteria to compete with the host for iron, which is bound to hemoglobin, transferrin, and lactoferrin.

FIGURE: Competition between host cells and bacterial pathogens for iron, illustrating the importance of siderophores. Since free iron is scarce in tissue fluids and blood, bacterial siderophores compete effectively for Fe 3+ bound to lactoferrin and transferrin.

Defense mechanisms of the host There are two defense mechanism of our body 1. Non-specific/ innate/ defence mechanisms 2. Specific / adaptive/ acquired/ 1. Non specific defense mechanisms • Non- specific defense provides the first line protection against potentially pathogenic microorganisms and are not specific to pathogenic species. • Most non-specific defenses are natural and offer protection from the moment of birth. – The non-specific defenses include: – Physical barrier - Inflammatory response – Chemical barrier - Phagocytosis – Normal microflora

I. Physical barrier a. Skin – The outer surface of the skin layer is composed of keratin which is not readily degraded by most microorganisms – Also - prevents attachment. - Impermeable to most pathogens. b. Mucous Membranes c. The whirling of system of bones – Projected to nasal cavities – Essential for trapping of entering microbes d. Fluid flow – Movement of fluids across the surface of body tissues protects the body from accumulation of microorganisms. Example, saliva washes microorganisms in the oral cavity to the stomach. Tears continuously remove microorganisms from the eye.

II. Chemical Barriers • These are secretions of body which have an antimicrobial activity. These include: – Lysozyme – Acidity – Interferon III. Phagocytosis – Phagocytosis is a process of engulfing and destroying an organism or other foreign body and digest with enzyme contained in cytoplasmic (lysosomes) granules of phagocytic cells. – During Phagocytosis, the m/o is engulfed by pseudopodia of phagocytic cell and is

IV. Normal Micro flora Normal microbial flora is microbial population frequently found in association with particular tissue that typically does not cause disease. Will be discussed in the next chapter in detail. V. Compliments : are plasma proteins found in inactive form and activated cascade reaction. They are named from C 1 -C 9

• Role of complements – Opsonization: coating of pathogens and facilitates for Phagocytosis e. g. , C 3 a – Chemoattractants e. g. , C 5 a – -Bacteriallysis (C 8 C 9) • VI. Inflammatory response • Inflammatory response is a non specific immune response to infection or injury and designed to remove cellular debris, localizing invading microorganism and arrest the spread of infection. – Role of inflammation • delivers additional cells of effector molecules to the site of infection • prevent the spread of infection • promote the repair of injured tissue • VII. NK cells / natural killers/ are lymphocytic in origin which kill virus infected cells with put antigenic stimulation

Adaptive • It is occurred if the organism couldn’t overcome the disease usually the innate defense mechanism – Occurred due to or following exposure to foreign substances – Is specific (response to particular pathogen) – It is mediated by lymphocytes (T-cells and B-cells) Accordingly: 1. Humeral immune response 2. Cell mediated immune response 1. Humoral immune response – Is mediated by antibody which are produce b-cells (antigen stimulated cells i. e. plasma cells) – involves five classes of immunoglobins Ig. A, Ig. D, Ig. E, Ig. G, Ig. M Role of antibody – Neutralization – Oppsonization – Complement activation
 cells called T-lymphocyte")
2. Cell mediated: is immunity mediated by sensitized (exposed to antigen) cells called T-lymphocyte and their cyokines with out involvement of antibody. Cytokines are small soluble proteins secreted by cells that can alter the behavior of the cell itself or another. – T cells includes 1. cytotoxic T-cells - destroys infected cells 2. T-helper cells (CD 4 cells) - Th 1 - secret cytokines which activate macrophages for interacellular killing - Th 2 - activates B-cells for exteracellular killing 3. Suppressor T- cells - regulate the function of the above T-cells • Adaptive immunity can be • Passive immunity • Active immunity

1. Passive immunity A. passive natural - occurred due to natural transferred immunoglobulin (Ig. G) B. passive artificial - occurred when Ab and lymphocytes are given to individual which is deficient of them. (i. e. , Ab and lymphocytes of another person) 2. Active immunity A. Active natural (contact with infection) B. active artificial (immunization)

Factors affecting host defence mechanism 1. Nutrition: Malnutrition predisposes to infection. 2. Age: The very old and the very young are particularly liable to infection. 3. Sex: May be attributes to hormonal influence. 4. Impairment of the host immune response –. radiotherapy – Immunosuppressive drugs including steroids –. Malignancy – HIV 5. Race 6. Climate 7. Occupation 8. Drugs 9. Pregnancy •

REFERENCES 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. Mackie and Mc. Cartney, Practical medical microbiology 13 th ed. 1989 Monica Cheesbrough. Medical Laboratory Manual for Tropical Countries, Microbiology, volume II, 2 nd edition. Tropical Health Technology and Butter Worth-Heinemannith, 2006. Geo. F. Brooks, Janet s. Butel, Staphen A. Morse. Jawetz, Malnick and Adelberg's Medical Microbiology. 21 st edition. Appelton & Langh, 1998. T. D. Sleight, M. C. Murphy. Notes on Medical bacteriology, 2 nd edition. Churchill livingstone, Medical division of Longman group UK limited, 1986. Rajesh Bhatia, Rattan Lal Ichhpujmai, Essentials of Medial Microbiology, 1 st edition. Jaypee brothers Medical Publishers Ltd. 1994. Salle(1981). Fundamental principles of bacteriology, Ta. Ta Mc. Graw – Hill publishing Company Ltd, New Dalhi Mackie and Mc. Cartney(1989). Practical medical microbiology 13 th edition. Churchill Livingston Bernand D. Davis, Renanto Dulbecco, Herman N. Eisen and Harold S. Ginsberg(1990). Microbiology 4 th edition. Lipinocott Company. Richard A. Harvey, Pamella C. Champ, Microbiology, Lippincott’s illustrated reviews, 2 nd ed. Benson’s microbiological application, Laboratory manual in general microbiology, 8 th ed. 2001 Sherris, Medical microbiology, an introduction to infectious disease. 4 th ed. 2004. 12. Baron's Medical Microbiology 4 th edition, 2000 13. Jawetz, Melnick, & Adelberg's Medical Microbiology, 24 th Ed, 2007 14. Abilo Tadesse, Meseret Alem, University of Gondar. , Ethiopia Public Health Training Initiative, The Carter Center, Minstry of Health, and the Ethiopia Ministry of Education, 2006
- Slides: 33