Chapter two Synovial Fluid Analysis Acknowledgements Addisa Ababa

Chapter two Synovial Fluid Analysis

Acknowledgements • • Addisa Ababa University Jimma University Hawassa University Haramaya University of Gondar American Society for Clinical Pathology Center for Disease Control and Prevention-Ethiopia

LEARNING OBJECTIVES Upon completion of this chapter, the reader will be able to: 1 Describe the formation and function of synovial fluid. 2 Relate laboratory test results to the four common classifications of joint disorders. 3 State the five most diagnostic tests performed on synovial fluid. 4 Determine the appropriate collection tubes for requested laboratory tests on synovial fluid. 5 Describe the appearance of synovial fluid in normal and abnormal states. 6 Discuss the normal and abnormal cellular composition

Learning Objectives 7 List and describe six crystals found in synovial fluid. 8 Explain the differentiation of monosodium urate and calcium pyrophosphate crystals using polarized and compensated polarized light. 9 State the clinical significance of glucose and lactate tests on synovial fluid. 10 List four genera of bacteria most frequently found in synovial fluid. 11 Describe the relationship of serologic testing of serum to joint disorders.

Chapter outline Introduction to Synovial Fluid Analysis Routine laboratory assay Collection of sample Gross examination (color, clarity) Total and differential leukocyte counts Gram's stain and bacterial culture (aerobic and anaerobic) • Crystal examination with polarizing microscope • • •

Synovial Fluid Definition: • Synovium refers to the tissue lining synovial tendon sheaths, bursae, and diarthrodial joints except for the articular surface. • Synovial fluid (synovia, SF) is an imperfect ultrafiltrate of blood plasma combined with hyaluronic acid produced by the synovial cells.

Synovial Fluid cont’d q Small ions and molecules (e. g. , Na+, K+, glucose, urea, etc. ) readily pass into the joint space and are, therefore, similar in concentration to plasma, while large molecules are absent or present in trace amounts

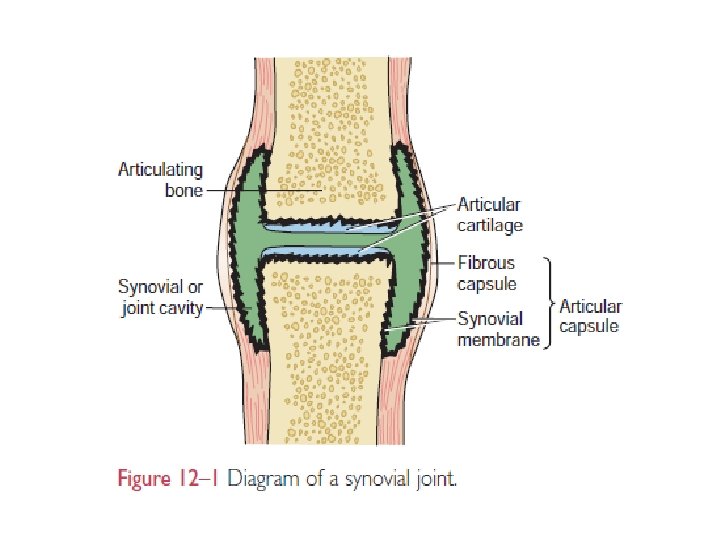
Physiology Synovial fluid, often referred to as “joint fluid, ” is a viscous liquid found in the cavities of the movable joints (diarthroses) or synovial joints. The bones in the synovial joints are lined with smooth Articular cartilage and separated by a cavity containing the synovial fluid. The synovial membrane contains specialized cells called synoviocytes. The smooth articular cartilage and synovial fluid reduce friction between the bones during joint movement. In addition provides nutrients to the articular cartilage

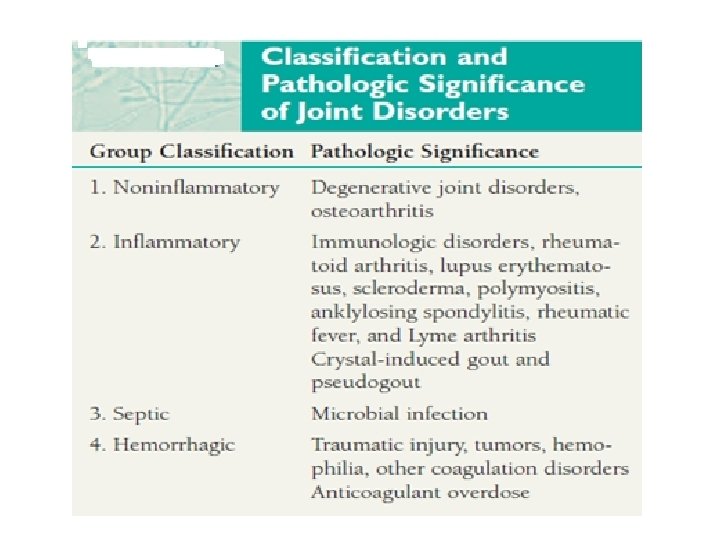
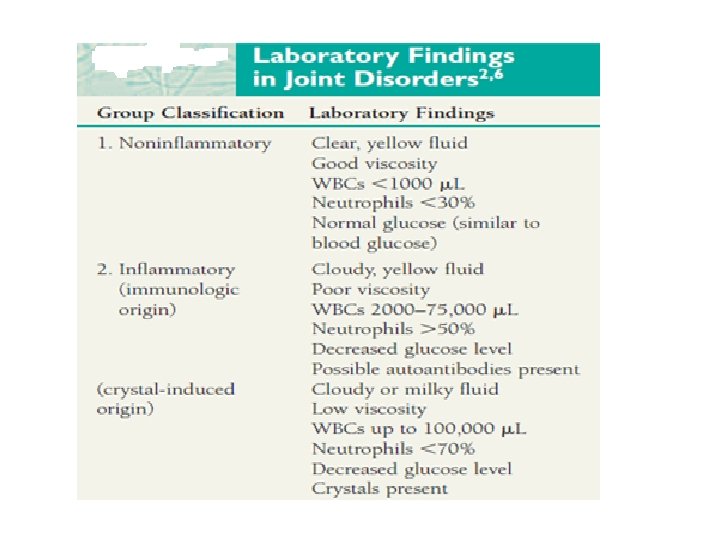
Classification of Synovial Fluid *Examination of the synovial fluid is essential to distinguish infectious from noninfectious arthritis Non inflammatory effusions (Group I) • Typically have leukocyte counts less than 3000/μL, with a minority of neutrophils. . • Non inflammatory response* • Non inflammatory effusions**
 • have leukocyte counts 3000 - 75 000, with neutrophils")
Inflammatory effusions (Group II) • have leukocyte counts 3000 - 75 000, with neutrophils accounting for over 50%. • Examples of this reaction group: – Rheumatoid arthritis – systemic lupus erythematosus (SLE) – Reiter's syndrome – rheumatic fever – acute crystal-induced arthritis – arthritis associated with inflammatory bowel disease – psoriatic arthritis – fat droplet synovitis
 effusions (Group III) • typically have leukocyte counts greater than 50, 000,")
Purulent (infectious) effusions (Group III) • typically have leukocyte counts greater than 50, 000, of which 90% or more are neutrophils. • Bacterial, fungal, and tuberculous joint infections constitute this group.
 • WBC count between 50– 10, 000 WBC/ m. L,")
Hemorrhagic effusions (Group IV) • WBC count between 50– 10, 000 WBC/ m. L, with < 50% neutrophils • RBCs may be present • may be seen in association with: – traumatic arthritis – pigmented villonodular synovitis – synovial hemangioma – neuropathic osteoarthropathy – joint prostheses – hematologic disorders (hemophilia, thrombocytopenia, anticoagulant therapy, sickle cell disease or trait, myeloproliferative syndrome).

Synovial Fluid Findings by Disease Category Finding Normal Group I Noninflammatory Group II Inflammatory Group III Infectious Group IV Hemorrhagic Clarity Transparent/ opaque Opaque Color Clear to pale yellow Xanthochromic to white/bloody White Red-brown or xanthochromic WBCs/m. L 0– 150 < 3000– 75 000 50 000– 200 000 50– 10 000 PMNs (%) < 25 < 30 > 50 > 90 < 50 RBCs No No No Yes Glucose (blood/SF difference mg/d. L) 0– 10 (0– 0. 56 mmol/L) 0– 40 (0– 2. 2 mmol/L) 20– 100 (1. 11– 5. 5 mmol/L) 0– 20 (0– 1. 11 mmol/L)

Cont’d
 should be confined to patients with an")
Specimen Collection • Joint fluid aspiration (arthrocentesis) should be confined to patients with an undiagnosed effusion • It should be performed by an experienced operator using good sterile technique. • Large joints (knee) normally contain< 4. 0 m. L of synovia – small sample size is common unless effusion is present.
 Total and differential")
Synovial Fluid Analysis Routine tests • • Gross examination (color, clarity) Total and differential leukocyte counts Gram's stain and bacterial culture (aerobic and anaerobic) Crystal examination with polarizing microscope Useful tests in certain circumstances • • Fungal and acid-fast stains and cultures PCR for bacterial and mycobacterial DNA Serum–synovial fluid glucose differential Lactate and other organic acids Complement Enzymes Uric acid

Recommended Tests • Major importance to differentiate crystal-induced joint disease from infectious arthritis. • When either disease is suspected perform: – Arthrocentesis – systematic examination of the synovial fluid • Examination diagnostic if performed correctly • In other joint diseases a specific diagnosis may not be possible Note: Fluid examination is important if only to rule out infectious arthritis, which is a critical diagnosis to make as a joint may be irreversibly damaged within 48 hours if not properly treated

Gross Examination of Synovial Fluid 1. Color • Should be evaluated in a clear glass tube against a white background. • Interpretation: – Normal SF is colorless but is often pale yellow. – Non inflammatory and inflammatory disorders are usually straw- to yellow-colored (xanthochromia). – Septic fluid may be yellow, brown, or green

Gross Examination of Synovial Fluid 2. Traumatic tap • produces an uneven distribution of blood during arthrocentesis or streaking in the syringe • pale yellow xanthochromia is difficult to distinguish from normal, a red-brown color following centrifugation is good evidence of pathologic hemarthrosis.

Gross Examination of Synovial Fluid 3. Clarity • relates to number and type of particles within the synovia. • Normal SF is transparent (newsprint is easily read through the tube) • Translucent fluid obscures details, – black and white areas can be distinguished – opaque fluid completely obscures the background. • Increased turbidity is less often due to concentrations of fibrin, free-floating ‘rice bodies’

Microscopic Examination Total Cell Count • Should be done within 1 hour following arthrocentesis to avoid degenerative cell loss. • Cell counts are usually performed in a standard hemocytometer and Automated cell counters

Microscopic Examination, cont’d… • A wet-prep slide count of 0 -2 WBCs /HPF (averaged over 10 fields) predicts less than 1300 WBCs by cell count • Leukocyte counts > 10 000/μL, and often > 50 000/μL, are characteristic of: o crystal-induced arthritis(e. g. , gout, pseudogout) o chronic inflammatory arthritis (e. g. , rheumatoid arthritis o systemic lupus erythematosus o ankylosing spondylitis, and others) o septic arthritis

Microscopic Examination, cont’d… q Leukocyte counts over 50 000/μL require dilution, which should be done with saline, not acetic acid, to avoid mucin clot formation and cell clumping. q Highly viscous synovial fluid should be incubated with hyaluronidase before counting, especially if automated counters are used. q Osteoarthritis, osteochondritis dissicans, trauma, and synovioma usually have total WBC counts less than 10 000/μL.

Microscopic Examination, cont’d… • The upper reference level for SF leukocytes is 150 -200/μL. • Elevated cell counts are used to help divide findings into different disease categories, but are nonspecific for any particular disease because of extensive overlap

Microscopic Examination, cont’d… Notes: • Erythrocytes should be routinely counted unless it is an obvious traumatic tap. • If a large number of red cells interferes with the leukocyte count, they may be lysed by dilution with 0. 3 normal saline or 1% saponin in saline • If there is the appearance of the fluid as bloody, count it because it indicates some infectious diseases.

Differential Leukocyte Count. • Cytospin preparations are preferred over smears from centrifuged SF because the cell morphology is significantly better. • Treatment with hyaluronidase may be necessary to produce thin smears in viscous specimens. • Neutrophils normally account for about 20% of SF leukocytes. • Neutrophils generally exceed 50% in urate gout, pseudogout, and rheumatoid arthritis (RA); they most often exceed 75% in acute bacterial arthritis.

Differential Leukocyte Count. q These cells frequently exhibit degenerative changes and may contain bacteria, crystals, lipid droplets, vacuoles, or dark blue to black granular inclusions (ragocytes, RA cells) which are similar to toxic granulation occasionally seen in peripheral blood smears. q The presence of ragocytes in patients with RA may indicate a poorer outcome.
 cells commonly present in patients with lupus")
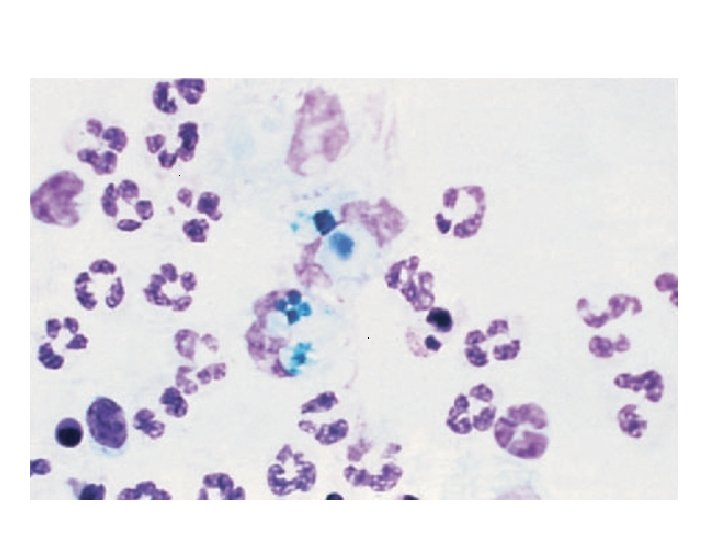
Differential Leukocyte Count. • LE (lupus erythematosus) cells commonly present in patients with lupus arthritis, are most often neutrophils which have phagocytosed the nuclei of degenerating cells ( Fig. 28 -10 ). (see next slide) • However, LE cells are not pathognomonic for systemic lupus erythrematosus since they have also been identified in the synovial fluid of RA patients

LE cell in the synovial fluid from a patient with systemic lupus erythematosus

Differential Leukocyte Count. Lymphocytes • normally constituting about 15% of the SF cells, are prominent in early RA and other collagen disorders, and chronic infections. • Reactive forms, including immunoblasts, are also occasionally present. Monocytes and macrophages • most common cells present in normal SF, accounting for approximately 65% of the cell count. • Reiter's cells, originally believed to be specific for Reiter's syndrome, are macrophages containing degenerating neutrophils

Differential Leukocyte Count. Eosinophilia • over 2% of the leukocyte count, has been reported in rheumatoid arthritis, rheumatic fever, metastatic carcinoma, Lyme disease, parasitic infections, chronic urticaria, angioedema, following arthrography (allergic reaction to dye), and irradiation

Crystal Identification Microscopic examination of synovial fluid for the presence of crystals is an important diagnostic test in the evaluation Of arthritis. Crystal formation in a joint frequently results in an acute, painful inflammation. It can also become a chronic condition. Causes of crystal formation include metabolic disorders and decreased renal excretion that produce elevated blood levels of crystallizing chemicals, degeneration of Cartilage and bone, and injection of medications, such as corticosteroids into a joint.

Types of Crystals • The primary crystals in synovial fluid are • monosodium urate (uric acid) (MSU) found in cases of gout and • Calcium pyrophosphate (CPPD) seen with pseudogout. • Hydroxyapatite (basic calcium phosphate) associated with calcified cartilage degeneration, • Increased serum uric acid resulting from impaired metabolism of purines; increased consumption of highpurine-content foods, alcohol, chemotherapy treatment of leukemias; and decreased renal excretion of uric acid are the most frequent causes of gout.

Crystal Examination. • Crystals formed from crystallization of solutes like gout due to accumulation of urate crystals • Crystals in synovial fluid lead to acute inflammation with increased WBC counts and a neutrophils-predominant infiltrate. Crystal identification, especially if intracellularly in neutrophils or macrophages, is pathognomonic for a crystal-induced arthritis

Crystal Examination cont’d… Gout : the process of crystal deposition in articular tissue. • most common types of endogenous crystals responsible for gouty arthritis are monosodium urate monohydrate (urate gout), calcium pyrophosphate dihydrate (pyrophosphate gout, chondrocalcinosis, or ‘pseudogout’), apatite and other basic calcium phosphates (BCP; apatite gout), calcium oxalate (oxalate gout), and lipids (lipid gout).

Crystal Examination cont’d… • Initial examination should be performed on a wet preparation using polarized light. • Phase-contrast microscopy enhances crystal detection. • Most crystals are scanned with a 10× objective • evaluated with at least a 40× objective, concentrating especially on cellular areas. • Complete examination requires 100× oil immersion, however, because apparently negative fluids on scanning may contain a large population of small crystals.
 crystals appear as needle-shaped rods 5 -20")
Crystal Examination cont’d… � Monosodium urate (MSU) crystals appear as needle-shaped rods 5 -20 μm long, but may be only 1– 2 μm in length or, rarely, appear as rounded spherolites. � They are strongly birefringent ( Fig. 28 -12 ): yellow when oriented parallel to the compensator, blue with perpendicular orientation (negative birefringence or elongation) ( Fig. 28 -13 ). � Quality Control: �A control slide of MSU crystals should always be used for comparison. �Alternatively, betamethasone, a steroid that appears as a strongly negative birefringent rod, can be used to prepare a reference slide for the polarizing microscope
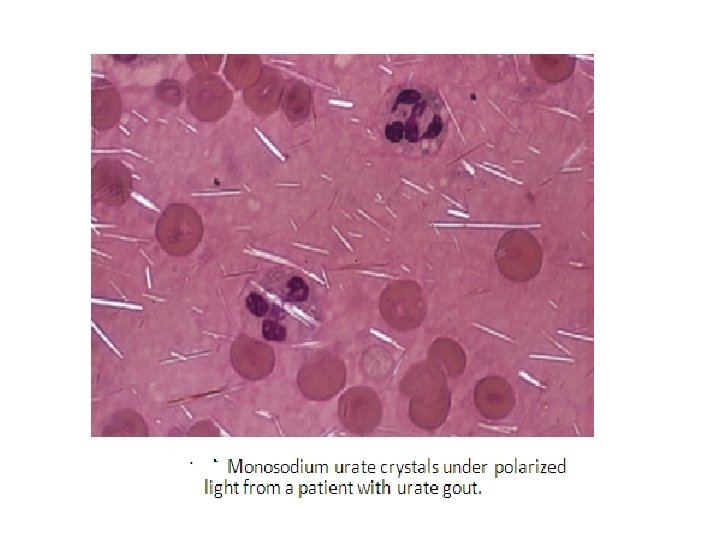

� Figure 28 -13 Monosodium urate crystals in synovial fluid. Compensated polarized light.
 crystals are found in a group")
Crystal Examination cont’d… • Calcium pyrophosphate dihydrate (CPPD) crystals are found in a group of conditions collectively known as CPPD crystal deposition disease.

limitations Interfering factors in crystal identification: � Glove powder �introduced during joint surgery appears as round, strongly birefringent particles 5 -30 μm in diameter with a Maltese cross appearance when polarized � Other crystals or particulates �monoclonal immunoglobulin crystals or cryoglobulins, �Charcot–Leyden crystals �amyloid, cartilage, and prosthetic fragments �collagen fibrils and fibrin strands �hematoidin crystals from prior hemorrhage �crystals from certain anticoagulants �nail polish �dust particles

Chemical Analysis • Because synovial fluid is chemically an ultra filtrate of plasma, chemistry test values are approximately the same as serum values. • The most frequently requested test is the glucose determination, as markedly decreased values are indicative of inflammatory or septic disorders. • offers only supportive information to the routine tests. • High viscosity may be remedied by dilution with normal saline, sonication, or hyaluronidase treatment

Reference Ranges for SF Constituents Total protein 1– 3 g/d. L 6– 8 g/d. L Albumin 55– 70% 50– 65% Alpha-1 -globulin 6– 8% 3– 5% Alpha-2 -globulin 5– 7% 7– 13% Beta-globulin 8– 10% 8– 14% Gamma-globulin 10– 14% 12– 22% Hyaluronic acid 0. 3– 0. 4 g/d. L Glucose 70– 110 mg/d. L Uric acid 2– 8 mg/d. L Lactate 9– 29 mg/d. L

Chemical analysis Glucose. – Proper interpretation of SF glucose values requires comparison with serum levels, – ideally preceded by a fast of 8 hours to allow glucose to equilibrate across the synovial membrane. – The serum–synovia differential is less than 10 mg/d. L in normal and many non inflammatory conditions. – In septic arthritis, this difference ranges from 20 -60 mg/d. L, but overlaps significantly with other inflammatory conditions, thereby limiting its clinical usefulness.

Chemical Analysis cont’d… • Protein. – Reference interval is 1. 0 -3. 0 g/d. L. – With increasing inflammation, larger proteins (e. g. , fibrinogen) enter the synovial space. – Spontaneous clot formation may be detected in nonanticoagulated specimen tubes (fibrin clot test – Measurement of SF protein is very nonspecific – The total protein level is not generally useful in patient diagnosis, treatment, or outcome.

Chemical Analysis cont’d… • Enzymes. – enzymes have been studied in SF, – lactate dehydrogenase, – aspartate aminotransferase, – adenosine deaminase, – acid and alkaline phosphatase, – and lysozyme among others – currently not clinically relevant, the measurement of various hydrolases may have significant predictive value in joint prognosis, especially RA.

Chemical Analysis cont’d… • Organic Acids. – SF lactic acid levels are usually increased in patients with septic arthritis. – Levels >30 mg/d. L are commonly associated with septic arthritis due to Gram-positive cocci and Gram-negative bacilli. – Using gas–liquid chromatography, the presence of other organic acids not normally present in SF may be very helpful in differentiating septic from non septic arthritis

Chemical Analysis cont’d… • Uric Acid. – SF uric acid levels generally parallel serum levels in gout and noninflammatory arthropathies. – Exception is inflammatory joint disorders other than gout, where SF urate levels may be significantly lower than in the paired serum. • Lipids – normal synovial fluid contains extremely low concentrations of lipids – quantification of lipids currently has no clinical value in joint fluid analysis except in cases where cholesterol crystals may resemble MSU or CPPD
 is found in synovia of about")
Immunologic studies Immunologic Studies – Rheumatoid factor (RF) is found in synovia of about 60% of RA patients, usually at a titer equal to or slightly lower than the serum titer. – Antinuclear antibodies (ANA) are found in the SF of about 70% of patients with SLE and 20% of patients with RA. – Neither is specific enough for practical use. SF complement levels, normally about 10% of serum levels, increase to 4070% of serum activity with inflammation, proportional to the increase of protein exudation.

Microbiological Examination • Immediate transportation of joint fluid are extremely important in the rapid identification of an infectious agent • Septic arthritis may be acute or chronic • Gram stain and culture should be performed as part of the routine synovial fluid evaluation. • Gram stain sensitivity varies from about 75% for staphylococcal infections, 50% for most Gram-negative organisms, to < 25% for gonococcal (GC) infections.

Microbiological Examination cont’d… • Culture sensitivity : – 75 -95% for non gonococcal joint infections in patients who have not received antibiotics. – For patients with gonorrhea, the sensitivity is only 10 -50%. • PCR with universal primers to detect bacterial DNA for the more fastidious, uncultivable pathogens like: – Borrelia burgdorferi – Chlamydia s – Mycoplasma sp.

Microbiological Examination cont’d… � Arthritis develops in approximately 60% of patients with Lyme disease resulting from exposure to ticks infected with Borrelia burgdorferi. � In patients with outdoor occupations, synovial fluid/tissue should be examined for fungal pathogens by KOH/calcofluor white stain � and cultured on selective fungal media. For example � a patient with a recent travel history to Arizona may present with a monoarticular arthritis secondary to Coccidioides immitis. �Patients with a chronic arthritis and risk factors for Mycobacterium tuberculosis or nontuberculous infections should undergo a synovial biopsy.

Microbiological Examination cont’d… • Ziehl–Neelsen or Kinyoun stains for acid-fast organisms have a sensitivity of about 20%. • Cultures for M. tuberculosis are positive in about 80% of proven cases. . • Synovial biopsy is recommended for suspected tuberculous arthritis to provide a more rapid diagnosis.

Synovial Testing Limitations • It is critical that tests be performed accurately to make specific diagnostic information. – Major problem in the laboratory examination of synovial fluid is there is no consensus as to what constitutes a ‘routine’ analysis’ – Quality performance is not consistent, due to the fact that the average laboratory examines only one to two synovial fluids each month

STUDY QUESTIONS 1. Explain the functions of synovial fluid 2. The primary function of synoviocytes is to: 3. Explain the testes Which is frequently performed 4. Explain normal synovial fluid macroscopically 5. List some of frequent crystales found in synovial fluid

References: • Urinalysis and body fluids / Susan King Strasinger, 5 th ed. 2008 • District laboratory practice in tropical countries. 2 nd ed. Part I. Monica • • Cheesbrough, 2005 Text book of urinalysis and body fluids. Doris LR, Ann EN, 1983 Urinalysis and body fluids: A color text and atlas. Karen MR, Jean JL. 1995 Clinical chemistry: Principles, procedures, correlation. 3 rd ed. Michael L. Bishop et al. 1996 Tietz Text book of clinical chemistry. 3 rd ed. Carl AB, Edward RA, 1999 Clinical chemistry: Theory, analysis, correlation 4 th ed. Lawrence AK. 2003 ASCP Document Urinalysis lecture note. Mistire W. , Dawite Y. 60
- Slides: 60