Chapter 6 The Pyramidal System Spastic Paralysis g


 lateral medial (MI) precentral gyrus and anterior paracentral lobule")






 tract: cerebral crus basilar pons medullary pyramidal decussation ~10% of fibers descend")

 corticospinal tract - (bilaterally) innervates the medial lower motor")







 tract: Fig. 16 -6 c arises in the “face region” (ventral part")


 are influenced by corticobulbar")

 Fig. 16 -6 b area")
 speed force direction Fig. 5 -1")

")
 paralysis (absence of volitional movement) (especially of skilled")


 reflex: Fig. 5 -13 tendon tension golgi tendon organ activation Ib")
 exaggerated patellar reflex Fig. 6 -7")






 pontine RF + extensors - flexors")

: contralateral upper motor neuron deficits & ipsilateral cranial nerve")
 Weber syndrome (alternating oculomotor hemiplegia, superior alternating hemiplegia)")
 contralateral spastic hemiplegia")
 contralateral spastic hemiplegia")

 Hemisection of spinal cord at C 8/T 1:")



- Slides: 51
Chapter 6 The Pyramidal System: Spastic Paralysis
g n i nn pla Fig. 5 -1 ec x e brainstem corticobulbar tract spinal cord pyramidal (corticospinal) tract n o uti
(MI) lateral medial (MI) precentral gyrus and anterior paracentral lobule
Pyramidal System upper lim b lower limb face Fig. 6 -1 face
upper lim b lower limb face corona radiata internal capsule CN III CN VI Fig. 6 -1 CN XII and medullary pyramid
corona radiata
corticobulbar tract corticospinal tract
posterior limb of internal capsule
Components of the internal capsule: Fig. 16 -5
Corticospinal (pyramidal) tract: cerebral crus basilar pons medullary pyramidal decussation ~10% of fibers descend in the anterior funiculus Fig. 6 -2 ~90% of fibers descend in the dorsal part of the lateral funiculus
most fibers decussate in the ventral white commissure Lower motor neuron Lateral corticospinal tract - innervates the lower motor neurons that supply the limbs (extends the entire length of spinal cord)
ventral white commissure Anterior (ventral) corticospinal tract - (bilaterally) innervates the medial lower motor neurons that supply the paraxial muscles (extends only into the cervical segments)
Fig. 6 -3
ventral corticospinal tract Fig. 6 -3
rostral midbrain
mid pons
caudal pons
pyramidal tract fibers parasagittal cut
caudal medulla rostral medulla
Corticobulbar (corticonuclear) tract: Fig. 16 -6 c arises in the “face region” (ventral part of precentral gyrus)
corona radiata internal capsule CN’s: V VII IX X XI XII nuclei innervating the external ocular muscles are not under the direct influence of the cerebral cortex
Motor nuclei of CN III, IV, and VI are influenced by the cortical and brainstem gaze centers (ch. 10) left frontal eye field Fig. 10 -2
Muscles that act in unison: (mastication, deglutition, phonation, lingual movements) are influenced by corticobulbar tract fibers from both hemispheres. Fig. 6 -4
Facial paralysis: Only the contralateral lower facial muscles are paralyzed after a unilateral lesion of the corticobulbar tract above the pons. UMN type LMN type
Movements are conceived in the frontal lobe (prefrontal cortex) Fig. 16 -6 b area 4 receives input from the premotor cortex, SII, and motor thalamus
MI (area 4) speed force direction Fig. 5 -1
Pyramidal tract: extends entire length of the CNS susceptible at any level to: vascular accidents trauma tumors demyelinating diseases (MS, ALS)
Lenticulostriate arteries (most common site of spontaneous hemorrhage in patients with chronic hypertension)
Upper motor neuron syndrome: (spastic paralysis) paralysis (absence of volitional movement) (especially of skilled movements) increased muscle tone (particularly antigravity muscles) clasp-knife response may be present exaggerated myotatic reflexes (decreased muscle spindle threshold) clonus may be present extensor plantar response Babinski sign slight atrophy symptoms are in the contralateral limbs and contralateral lower facial muscles
Right spastic hemiplegia: paralysis accompanied by increased muscle tone & increased resistance to passive stretch in the antigravity muscles capsular stroke on the left Fig. 6 -5
clasp-knife response: Fig. 6 -6
Inverse myotatic (lengthening) reflex: Fig. 5 -13 tendon tension golgi tendon organ activation Ib impulses excitation of interneurons inhibition of lower motor neurons relaxation of muscle
Hyperactive myotatic reflexes: (especially in quadriceps and biceps) exaggerated patellar reflex Fig. 6 -7
clonus Fig. 6 -8
stroking the lateral aspect of the sole with a hard, blunt object Fig. 6 -9 seen when the corticospinal system is normal
a withdrawal reflex normally suppressed directly by the cerebral cortex (this extension is normal in infants before the corticospinal tract is fully myelinated) Fig. 6 -9 in the adult it is associated with corticospinal tract damage
A - axial B - shoulder C - arm D - forearm E - hand Fig. 7 -1 movements in proximal limbs recover somewhat with time, but rapid individual finger movements never return
Fig. 5 -1
red nucleus reticular formation vestibular nuclei
higher centers red nucleus + flexors (upper limb) pontine RF + extensors - flexors + medullary RF - extensors + flexors vestibular nuclei + extensors
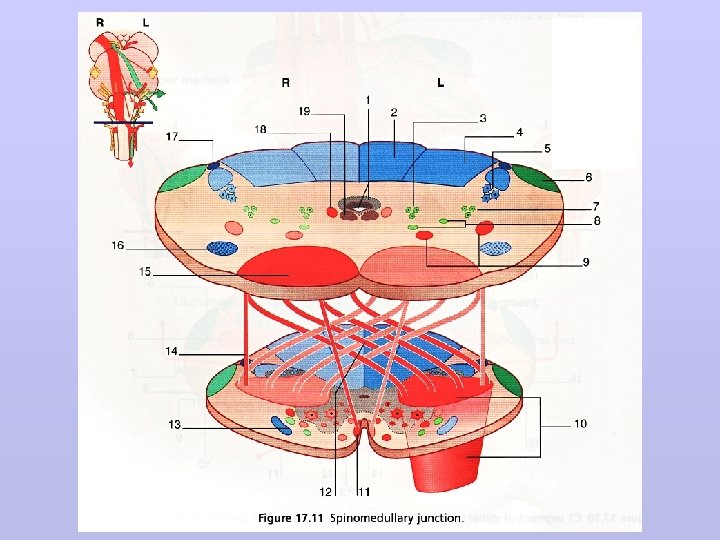
Note the proximity of the pyramidal tract to the intramedullary rootlets of CN’s IIl, VI and XII CN III CN VI Fig. 6 -1 CN XII
Alternating hemiplegias (aka. crossed paralyses): contralateral upper motor neuron deficits & ipsilateral cranial nerve (lower motor neuron) deficits
Damage in the cerebral crus (midbrain) Weber syndrome (alternating oculomotor hemiplegia, superior alternating hemiplegia) contralateral spastic hemiplegia plus ipsilateral ophthalmoplegia, mydriasis, ptosis
Damage in the basilar pons alternating abducens hemiplegia (middle alternating hemiplegia) contralateral spastic hemiplegia plus ipsilateral esotropia, paralysis of abduction
Damage in the medullary pyramid alternating hypoglossal hemiplegia (inferior alternating hemiplegia) contralateral spastic hemiplegia plus ipsilateral paralysis of tongue muscles
Combined UMN and LMN lesions also occur in the spinal cord: Below the level of the lesion: spasticity and other UMN lesion phenomena At the level of the lesion: flaccid paralysis and other LMN lesion phenomena the UMN and LMN signs are both ipsilateral
Ulnar nerve (C 8, T 1) Hemisection of spinal cord at C 8/T 1: spasticity, extensor plantar response, etc. in ipsilateral lower limb flaccid paralysis, atrophy of intrinsic mm of ipsilateral hand
Somatotopic localization of the long ascending and descending paths: Spinal cord injuries most frequently damage its central part, “sparing” the motor activity and sensations associated with the lower sacral segments. Therefore, when present “sacral sparing”, this indicates that the recovery of some spinal cord function is more likely.
Chapter 6 know the sites of origin of the corticospinal tract fibers that command the upper and lower limbs know the locations of the corticospinal tract axons as they descend through the cerebral hemispheres and the brainstem know the sites of decussation of the pyramidal tract fibers that form the lateral corticospinal tract know the site of decussation of the ventral corticospinal tract know the motor nuclei of the spinal cord that are influenced by the ventral corticospinal tract know the site of origin of the corticobulbar tract know which cranial nerve motor nuclei are influenced by bilateral corticobulbar tracts know the cranial nerve motor nucleus that is only influenced by the contralateral corticobulbar tract know the cranial nerve motor nuclei that are not under the direct control of the cerebral cortex know the sites within the CNS were the upper motor neurons in the corticospinal (pyramidal) tract are susceptible to injury know the principal signs associated with upper motor neuron syndrome know which movements recover more readily and which movements do not recover following a corticospinal tract injury and why
Chapter 6 continued know the 3 cranial nerves that are susceptible to injury along with the pyramidal tract know the LMN and UMN signs associated with the alternating hemiplegias know how the presence of sacral sparing affects a patient’s prognosis after a spinal cord injury