Chapter 5 Shock Objectives Identify causes and characteristics

Chapter 5 Shock

Objectives • Identify causes and characteristics of shock in the trauma patient • Describe pathophysiologic changes as a basis for assessment of the trauma patient in shock • Plan appropriate interventions for the trauma patient in shock • Evaluate the effectiveness of interventions for the trauma patient in shock

Shock Increased metabolic demand Insufficient oxygen supply Inadequate tissue perfusion Oxygen demand Cellular hypoxia Oxygen supply Triggers compensatory mechanisms

Pathophysiology Aerobic metabolism • Efficient production of ATP • ATP maintains cellular metabolic function Anaerobic metabolism • Inefficient production of ATP • Lactic acid is a byproduct of production • Leads to metabolic acidosis • Cellular dysfunction leads to cell death Normal cell Influx of fluid Cytosol and organelles swelling Rupture of membrane, leakage of proteases and lysosomes

Pathophysiology CARDIAC OUTPUT = STROKE VOLUME x HEART RATE AFTERLOAD PRELOAD CONTRACTILITY
 Shock")
Stages of Shock: Overview Stage I: Compensated Shock Stage II: Decompensated (Progressive, Hypotensive) Shock Stage III: Irreversible Shock

Stages of Shock: Compensated Shock Assessment Findings OFTEN VERY SUBTLE • Anxiety, confusion, restlessness • Narrowing pulse pressure • Rising diastolic BP • Minimal change in systolic BP • Tachycardia with bounding pulse • Decreasing urinary output

Stages of Shock: Progressive or Decompensated Shock Assessment Findings • Decreased level of consciousness • Hypotension • Narrowed pulse pressure • Tachycardia with weak pulses • Tachypnea • Cool, clammy, cyanotic skin

Stages of Shock: Irreversible Shock Assessment Findings • Obtunded or comatose • Profound hypotension • Bradycardia • Dysrhythmias • Slow, shallow respirations • Petechiae or purpura

Compensatory Response to Shock • Baroreceptors sense decreased stretch • Chemoreceptors detect increased CO 2 and decreased p. H • Sympathetic nervous system is activated • Adrenal glands release catecholamines • Epinephrine • Norepinephrine

Respiratory Response ↑ Elimination of CO 2 ↑ Respiratory rate ↑ Oxygen intake Smooth muscle relaxation allows for increased air flow ↑ Oxygen exchange

Cerebral Autoregulation Blood is preferentially shunted to the brain, which cannot store glucose Altered LOC noted when autoregulation fails (MAP less than 50 mm Hg) Cool, pale , diaphoretic skin Capillary refill > 2 seconds Blood shunted away from the skin and splanchnic circulation (GI tract, spleen, liver)

Renal Response Angiotensin II aldosterone Na and H 2 O reabsorption Angiotensin I converted to angiotensin II in the lungs Renal hypoperfusion release of renin angiotensin Angiotensin II ADH H 2 O retention Altered LOC Thirst, relentlessness Dilated pupils Vasoconstriction ↓ pulse pressure ↓urine output
 ↑ Respiratory rate • Designed to")
Immune Response • Systemic Inflammatory Response Syndrome (SIRS) ↑ Respiratory rate • Designed to limit the initial tissue injury or ↑ Heart rate blood loss • Multiple organ systems Release of are impacted • Tissue damage • Organ failure aldosterone and cortisol Cool, clammy, pale or cyanotic skin Capillary refill > 2 seconds Altered LOC Thirst, relentlessness Dilated pupils Hypotension Constriction of splanchnic vessels ↓urine output ↑specific gravity

Trauma Triad of Death Coagulopathy • Trauma-induced • Resuscitation-related Acidosis • Reduced p. H • Elevated lactate level • Excessive fluids Hypothermia • Exposure • Excessive bleeding • Worsens acidosis

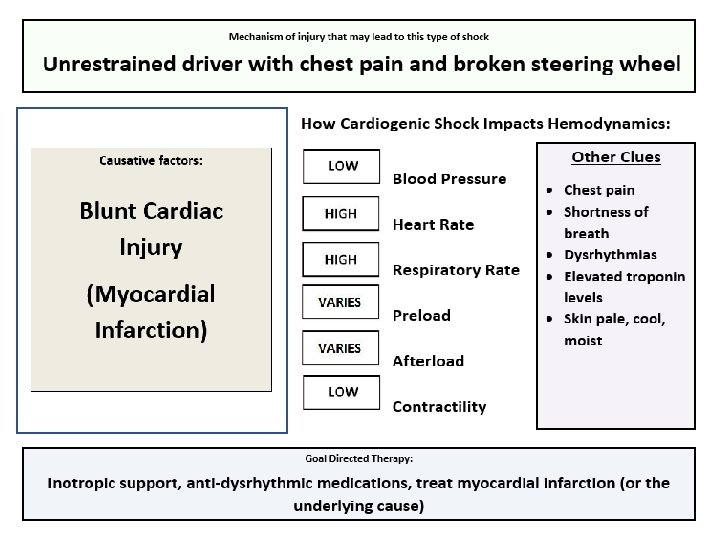
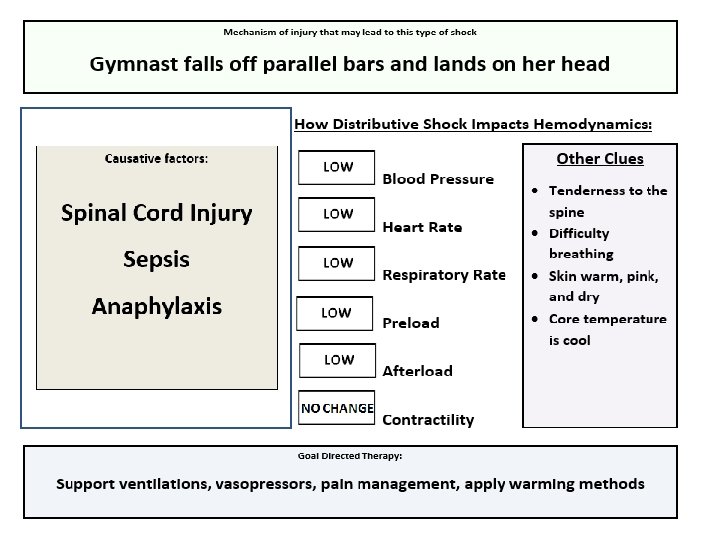
Shock: Types and Causes OBSTRUCTIVE SHOCK Compression/obstruction Cardiac tamponade Tension pneumothorax HYPOVOLEMIC SHOCK Reservoir depletion Hemorrhage Hypovolemia CARDIOGENIC SHOCK Pump failure Blunt cardiac injury Dysrhythmia Myocardial infarction DISTRIBUTIVE SHOCK Vasodilation Anaphylaxis Sepsis Spinal cord injury (neurogenic shock)

Hypovolemic Shock

Obstructive Shock

Cardiogenic Shock

Distributive Shock

Current Management Strategies • Tourniquets • Damage control resuscitation • Hypotensive resuscitation • Hemostatic resuscitation INDNAM [CC BY-SA 3. 0 (https: //creativecommons. org/licenses/by-sa/3. 0) or GFDL (http: //www. gnu. org/copyleft/fdl. html)], from Wikimedia Commons
 • Tranexamic acid (TXA) • Damage")
Current Management Strategies • Massive Transfusion Protocol (MTP) • Tranexamic acid (TXA) • Damage control surgery Mark Oniffrey [CC BY-SA 4. 0 (https: //creativecommons. org/licenses/by-sa/4. 0)], from Wikimedia Commons

Emerging Trends • TEG or ROTEM • REBOA • Whole Blood • Freeze Dried Plasma

Emerging Trends • Hemostatic dressings • Bleeding control education for the community Re. Al [CC BY-SA 4. 0 (https: //creativecommons. org/licenses/by-sa/4. 0)], from Wikimedia Commons Pfc. David Devich [Public domain], via Wikimedia Commons

Shock Activity Correlate each type of shock with its identifying characteristics Instructions Match each piece provided to the 5 spaces on your card Causative factors are placed over the shock image Think about what this looks like clinically

Obstructive Shock
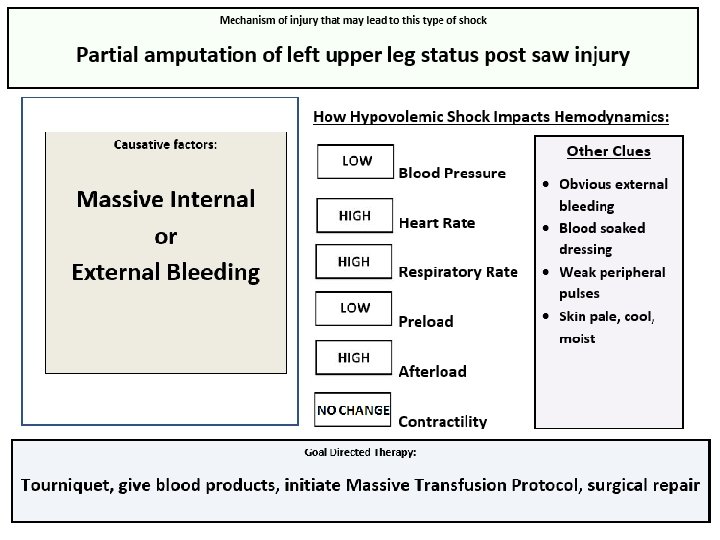

Summary • Shock is the mismatch between supply and demand of oxygen and nutrients • Hemorrhagic shock is the most common preventable cause of death in a trauma patient • Early recognition and goal-directed therapy leads to optimal outcomes

Time Left for Break 15 Minutes

Time Left for Break 14 Minutes

Time Left for Break 13 Minutes

Time Left for Break 12 Minutes

Time Left for Break 11 Minutes

Time Left for Break 10 Minutes

Time Left for Break 9 Minutes

Time Left for Break 8 Minutes

Time Left for Break 7 Minutes

Time Left for Break 6 Minutes

Time Left for Break 5 Minutes

Time Left for Break 4 Minutes

Time Left for Break 3 Minutes

Time Left for Break 2 Minutes

Time Left for Break 1 Minute

Time Left for Break 30 Seconds

Time Left for Break Time’ s Up!!
- Slides: 47