Chapter 5 Emergency Airway Management Rapid Sequence Intubation

Chapter 5 Emergency Airway Management — Rapid Sequence Intubation Loren G Yamamoto MD, MPH, MBA, FAAP, FACEP Textbook reading Ped ED group of CGMH MA陳冠甫

¡ ¡ Rapid Sequence Intubation Sedatives Sedative Selection Muscle Relaxants Muscle Relaxant Selection Defasciculation and Priming ¡ Adjunctive Agents ¡ Rapid Sequence Intubation Protocol Nasal Intubation Compared with Oral Intubation in the Trauma Patient Cervical Spine Immobilization During Endotracheal Intubation ¡ Alternative Intubation and Airway Techniques ¡ Avoiding Problems ¡ Multiple Trauma ¡ Head Trauma ¡ Burns ¡ Status Epilepticus ¡ Agitated Patients Who Require Procedures or Transport

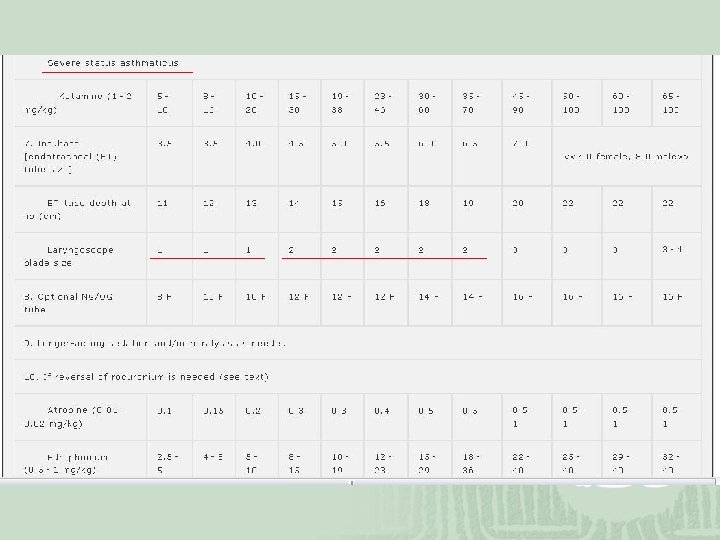
Table 5. 1. Equipment Needed for Rapid Sequence Intubation Pulse oximeter End-tidal CO 2, monitor or detector Electrocardiogram monitor Uncuffed endotracheal tubes, sizes 2. 5– 6. 0 Cuffed endotracheal tubes, sizes 6. 0– 8. 5 Endotracheal tube stylets Laryngoscopes (straight blade sizes 0– 3, curved blade sizes 2– 4) Oral airways Oxygen masks, preferably a nonrebreather Ventilation masks in all sizes for bag-valve-mask ventilation Large and small self-inflating ventilation bag with oxygen reservoir tail and positive end-expiratory pressure valve attachment Laryngeal mask airways in all sizes Oxygen source Suctioning source Large-bore stiff suction tips Flexible suction catheters Nasogastric tubes Tracheostomy surgical instrument set 12 - and 14 -Gauge needle catheters for needle cricothyrotomy Preassembled transtracheal ventilation setup

Indication 1. severe hypoxenia 2. inadequate alveolar ventilation 3. inadequate lung expansion 4. inadequate resp muscle strength 5. excessive work of breathing 6. unstable ventilatory drive 7. prophylactic mechanic ventilation, TB 8. IICP 9. flail chest, TB 10. COPD, asthma

Rapid Sequence Intubation Sedatives Table 5. 2. Significant Properties of Rapid Sequence Intubation Sedatives Cerebro Protective Effect Cardiovascular Effect Bronchial Effect Drug Onset Duration Etomidate Rapid Brief Good Neutral Thiopental Rapid Brief Good Significant depression Broncho spasm Midazolam Less Brief Modest Neutral Rapid Other Disadvantages Myoclonus, cortisol suppression Titration recommended, is not feasible in rapid sequence intubation (RSI) Ketamine Rapid Brief Adverse Stimulatory Bronchodilator Psychic reactions and excessive airway secretions Fentanyl Less Brief Modest Neutral Seizurelike activity and chest wall rigidity Brief Good Significant depression Neutral Less experience with agent in emergency department RSI rapid Propofol Rapid

Other side effect or precaution ¡ Thiopental Contra: porphyria and status asthmaticus ¡ Midazolam Contra: glaucoma Insufficient unconsciousness ¡ Ketamine Contra: ICP, IOP, HTN Lorazepam for psychi ¡ Etomidate (standard in US) Adrenal insufficiency: long term user ¡ Fentanyl Pre: MAOI ¡ All sedatives cause some degree of CV depression!!

Sedative Selection
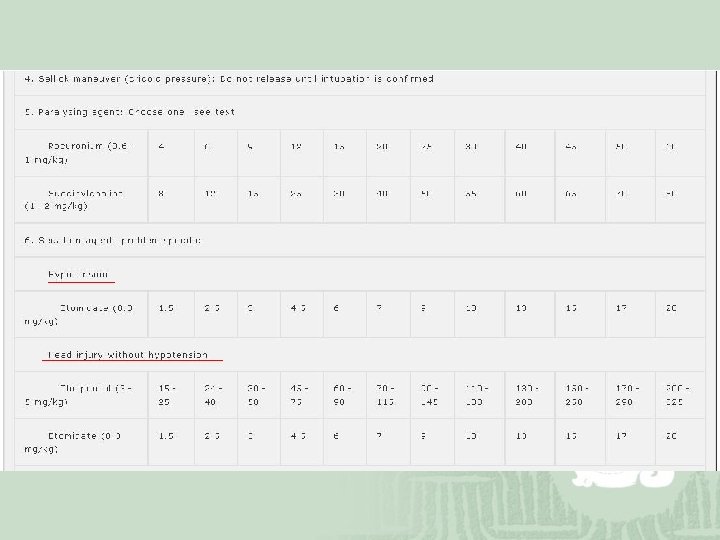

Muscle Relaxants ¡ Depolarizing muscle relaxant, Succinylcholine Onset: 30 to 60 seconds Duration: 3 to 12 minutes Disadvantages: ¡ ↑ICP, IOP, IGP ¡ Fasciculations: rhabdomyolysis, myoglobinuria Defasciculating dose of vecuronium, 10% (>5 y/o) Atropine premedication: bradycardia and bronchodilate Contraindicated: glaucoma, penetrating eye injuries, significant neuromuscular disease, history or family history of malignant hyperthermia, and pseudocholinesterase deficiency, at 3 to 60 days after trauma or burns, severe burns or large crush injuries

Muscle Relaxants ¡ nondepolarizing muscle relaxants Rocuronium vs Vecuronium ¡Onset: 30 -90 vs 90 -120 seconds ¡Duration: both 25 to 60 minutes ¡Ro: premixed Pancuronium vs Atracurium ¡Pan: slower onset and more CV side effects ¡Atra: same as Ve but more histamine and CV SE

Muscle Relaxant Selection ¡ Rocuronium and succinylcholine Safer: Rocuronium Reversible /c edrophonium: Rocuronium Onset: same Quicker: succinylcholine, good in difficult one ¡ Defasciculation and Priming Defasciculation: in Succ, 1/10 dose of Roc, 1 -3 mins prior ¡ Muscular p’t Priming: in non-dep, 1/10 dose of it, 5 mins prior ¡ Shorten onset ¡ Min effect in Roc

Adjunctive Agents ¡ Atropine Routine in kid, add /c ketamine in adult ¡ Lidocaine ↓ICP and airway reactivity Cerebroproctect not clear if /c other agent Topical: add complexity Asthma: ↓bronchospasm to PREVENT ETT! ¡ Opiate analgesics Unconsciousness: reliable in etomidate & thiopental BZD: need titrated & less reliable

Rapid Sequence Intubation Protocol ¡ Protocol 6 Ps: important to stress Sequence: relaxant to sedatives? Regularly review ¡ Nasal vs Oral Intubation in Trauma Patient N>O: Older literature O>N: ¡ more reliable, ¡ lesser neck movement, ICP, vomiting, no difference in C-spine movement ¡ Laryngoscope: no evidence, and RSI can improve ¡ C-Spine Immobilization During Endotracheal Intubation Philadelphia collars, Axial (inline) traction: no evidence Anterior portion of neck collar 2005 CPR: still moved by jaw thrust

Alternative Intubation & Airway Techniques ¡ Flexible fiberoptic scopes, lighted stylets to guide nasal tracheal intubation, retrograde intubations, and surgical airways ¡ Reserved for conventional airway techniques prove unsuccessful ¡ not recommended in ED: aided by bronchoscopy, lighted stylets, and retrograde wire technique ¡ Recommended: Recommended Combitube and LMA ¡ Surgical airway: favor needle cricothyrotomy

Avoiding Problems ¡ Possible CV adverse effect: wide open IVF ¡ Paralysis: not a substitute for sedation except… ¡ Multiple Trauma Still ABCDEs Oximetry for perfusion Sedatives in hypovolemic or hypotensive: reduced or avoided ¡ Head Trauma ICH can cause significant hypovolemia in infant ¡ Burns avoid succinylcholine ¡ Status Epilepticus initiate RSI earlier rather than later. ¡ Agitated Patients Who Require Procedures or Transport Consider RSI earlier
- Slides: 16