Chapter 20 Schizophrenia a psychosis disorder Characteristics Delusions






















: Risk Of Agranulocytosis And Seizures; Must Be Monitored Closely")

 More Sedative Less EPS, Causes Hypotension At Higher Doses")
 • Benztropine (Cogentin) • Dyphenhydramine Hydrochloride (Benadryl)")

















- Slides: 44
Chapter 20 Schizophrenia a psychosis disorder
Characteristics • Delusions • Hallucinations • Disorganized Speech • Disorganized Or Catatonic Behavior • Psychotic Symptoms More Pronounced And Disruptive Than In Other Psychotic Disorders
• Ability to work • Interpersonal relationships • Self-care abilities • Social functioning • Quality of life
DSM IV Criteria For Schizophrenia Subtypes • Paranoid • Catatonic • Disorganized Signs and Symptoms • Positive symptoms • Negative symptoms • Cognitive symptoms • Mood symptoms
Co-morbidity • Substance Abuse – Nicotine Dependence • Depression/Anxiety • Suicide • Psychosis-induced Polydipsia
Facts About Schizophrenia • Late Teens To Early Thirties – Early 20’s For Men / Late 20’s For Women • 1 In 100 Adults • 1 In 40, 000 Children
Neuro-biological • Excessive Dopamine Activity • Neuronal Development In Utero And Young Life • Brain Structure Changes – Enlarged Ventricles, Smaller Hippocampus – Increased Number Of Dopamine Receptors In Basal Ganglia
Course Of Schizophrenia Chronic With Each Acute Exacerbation Of Psychosis Results In Residual Dysfunction
Phases In Course Of Schizophrenia 1. Acute Phase – Positive Symptoms And Negative Symptoms 2. Maintenance Phase – Acute Symptoms Are Less Severe 3. Stabilization Phase – Remission Of Symptoms
Potential Early Symptoms: Prepsychotic • Withdrawal • Depressed/Anxious • Phobias • Obsessions And Compulsions • Difficulty Concentrating • Preoccupation With Religion, Self • Dissociative Symptoms
Signs And Symptoms Of Schizophrenia
Symptoms Of Schizophrenia • Positive Symptoms • Negative Symptoms – Hallucinations – Apathy – Delusions – Flat Affect – Bizarre Behavior – Alogia; Poverty Of Speech – Paranoia – Avolition; Lack Of Motivation – Anhedonia – Poor Social Functioning
Positive Symptoms: Alteration In Thinking • Delusions: False, Fixed Beliefs That Cannot Be Corrected By Reasoning – – – – – Ideas Of Reference Persecution Grandiosity Somatic Sensations Jealousy Control Thought Broadcasting Thought Insertion Thought Withdrawal
Positive Symptoms: Alterations In Speech • Associative Looseness • Neologisms • Echolalia • Clang Association • Word Salad
Positive Symptoms: Alterations In Perception • Hallucinations: Sensory Perceptions For Which No External Stimulus Exists – Auditory – Visual – Olfactory – Tactile
Positive Symptoms: Alterations In Behavior • Extreme Motor Agitation • Stereotyped Behaviors • Waxy Flexibility • Stupor
Negative Symptoms • Affective Blunting • Anergia • Anhedonia • Avolition • Poverty Of Content Of Speech • Thought Blocking • Flat Affect/Inappropriate Affect
Cognitive Symptoms • Inattention, Easily Distracted • Impaired Memory • Poor Problem-solving Skills, executive functioning – Poor Decision-making Skills – Illogical Thinking – Impaired Judgment
Depression And Other Mood Symptoms • Dysphoria • Suicidal Ideation • Hopelessness
Assessment Of Client • Safety Of Client And Others • Medical History And Recent Medical Workup • Positive, Negative, Cognitive, And Mood Symptoms • Current Medications And Compliance To Treatment • Family Response/Support System
Treatment • Psychosocial – Clinical Support – Family Support – Rehabilitative Services – Humanitarian And / Public Services • Pharmacological – First Generation Neuroleptics – Second Generation Neuroleptics – Range Of Significant Side Effects
Atypical Antipsychotics • Chosen As First Line Treatment: Treat Both Positive And Negative Symptoms • Produce Minimal To No Extrapyramidal Side Effects (EPS) Or Tardive Dyskinesia • Decrease Suicidal Behavior
Atypical Antipsychotics • Clozapine (Clozaril): Risk Of Agranulocytosis And Seizures; Must Be Monitored Closely • Risperidone (Risperdal) • Olanzapine (Zyprexa) • Quetiapine (Seroquel) • Ziprasidone (Geodon)* • Aripiprazole (Abilify)*
Traditional Antipsychotics • Cause Extrapyramidal Side Effects – Akathisia, Dystonia, Pseudo Parkinsonism, And Tardive Dyskinesia – Also Cause Anticholinergic, Orthostasis, And Lower Seizure Threshold
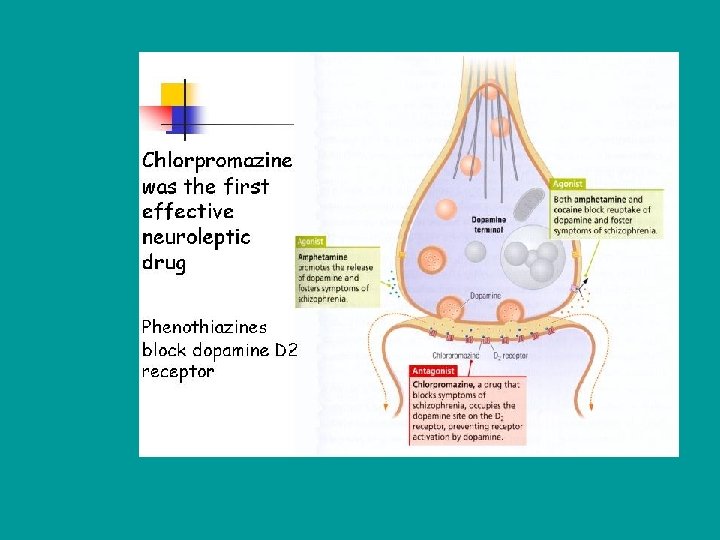
Traditional Antipsychotics • Chlorpromazine (Thorazine) More Sedative Less EPS, Causes Hypotension At Higher Doses • Haloperidol (Haldol) Least Sedating However High Incidence Of EPS ***Watch For Neuromalignant Syndrome: Decreased Level Of Consciousness, Increased Muscle Tone, tachycardia, Tachypnea, Diaphoresis, Hyperpyrexia
Treatment Of Acute EPS • Trihexyphenidyl (Artane) • Benztropine (Cogentin) • Dyphenhydramine Hydrochloride (Benadryl) • Bromocriptine Mesylate (Parlodel)
Side Effects: Anticholinergic Symptoms • Dry Mouth • Urinary Retention And Hesitancy • Constipation • Blurred Vision • Photosensitivity • Dry Eyes • Sexual Dysfunction
Side Effects: Α 2 Block: Cardiovascular Effects • Hypotension – Postural Hypotension • Tachycardia
Side Effects: Rare And Toxic Effects • Agranulocytosis • Cholestatic Jaundice • Neuroleptic Malignant Syndrome (NMS) – Severe Extrapyramidal – Hyperpyrexia – Autonomic Dysfunction
Nursing Diagnosis • Impaired Thought Process • Impaired Sensory Perceptions • Impaired Verbal Communication • Self-care Deficit • Social Isolation
Nursing Interventions • Promote Trust • Promote Positive Orientation • Promote Perceived Control • Promote Strengths • Meet Health Oriented Goals
Nursing Interventions Cont’d • Distraction From Voices: Listen To Music; Read Aloud; Count Backwards From 100 • Tell Voices To Go Away; Talk To Voices While Pretending To Use Mobile Phone • Nurses Response To Client Hearing Voices Or Having Visual Hallucinations (“I Don’t See The Devil Standing Over You, But I Do Understand How Upsetting That Must Be • Validate If Part Of A Delusion Is Real: “Yes There Was A Man At The Nurses’ Station, But I Did Not Hear Him Talk About You
Milieu Therapy • Safety – Potential For Physical Violence Due To Hallucinations Or Delusions – Priority Is Least Restrictive Safety Technique • Verbal De-escalation • Medications • Seclusion Or Restraints • Activities – Provide Support And Structure – Encourage Development Of Social Skills And Friendships
Counseling: Communication Guidelines • Hallucinations – Hearing Voices Most Common – Approach Client In Nonthreatening And Nonjudgmental Manner – Assess If Messages Are Suicidal Or Homicidal – Initiate Safety Measures If Needed – Client Anxious, Fearful, Lonely, Brain Not Processing Stimuli Accurately
Counseling: Communication Guidelines • Delusions – Be Open, Honest, Matter-of-fact, And Calm – Have Client Describe Delusion – Avoid Arguing About Content – Interject Doubt – Validate Part Of Delusion That Is Real
Counseling: Communication Guideline • Associative Looseness – Do Not Pretend That You Understand – Look For Reoccurring Topics And Themes – Emphasize What Is Going On In The Client's Environment – Involve Client In Simple, Reality-based Activities – Reinforce Clear Communication Of Needs, Feelings, And Thoughts
Client Teaching: Coping Techniques For Schizophrenia • Distraction • Interaction • Activity – Social And Physical
Client And Family Teaching For Schizophrenia • Learn All You Can About The Illness. • Develop A Relapse Prevention Plan. • Avoid Alcohol And Drugs. • Learn Ways To Address Fears And Losses. • Learn New Ways Of Coping. • Comply With Treatment. • Maintain Communication With Supportive People. • Stay Healthy By Managing Illness, Sleep, And Diet.
? • A Client Diagnosed With Schizophrenia Is Having Negative Symptoms Associated With His Illness. Which Of The Following Is Classified As A Negative Symptom? – A. Abnormal Thoughts – B. Ideas Of Reference – C. Blunted Affect – D. Hallucinations
? • Sally Believed That She Was Mary Magdalene And That Jesus Was Controlling Her Thoughts And Telling Her How To Save The World What Type Of Delusion Is This?
? • “I Was Going To Tell Him The Mannerologies Of The Hospital; I Want All The Vetchkisses To Leave The Room And Leave Me Be. ” – What Type Of Speech Is This?
? • When Mary Saw The Doctor And Nurse Talking Together, She Believed They Were Plotting Against Her. – What Type Of Delusion Is This?
Working With Clients With Schizophrenia • Peer Group Supervision • Team Approach To Decrease Staff Burnout • Periodic Re-assessments Of – Treatment Outcomes – Client's Strengths And Weaknesses