CHAPTER 17 Late Adulthood Physical and Cognitive Development






 • Presbycusis – Age-related hearing loss that affects about one person")
 • Bones lose more density in late adulthood, becoming more brittle")




 • Changes may be slowed or reversed through estrogenreplacement therapy.")

 • Testosterone production declines gradually from age 40 to age")

 • Couples can adapt to the physical changes of")


 • Immunological theory – Holds that the immune system is")
 • Cross-linking theory – As we age, cell proteins bind")



 • Most older adults don’t need institutional care. –")

 • Older people not adequately screened for cancer")
 • Hypertension – Affecting about 50% of Americans")

 • Osteoarthritis – – – – Painful, degenerative disease involving wear and")
 • Rheumatoid arthritis – Characterized by chronic inflammation of the membranes that")

 • Reasons for addiction or adverse reactions include – doctors prescribing")


 • Alzheimer’s disease – About one in 10 Americans")


 • AD is the fifth leading killer of older")
 • People with AD may get lost in stores,")




 • Cohn et al. (2008) believe the frontal regions—executive center of")
 conducted research on recollection of grades on")

 • People seem to recall events from the second and third")

 • Age-related decline in prospective memory – Greatest when the task")


 suggests distractibility can enable")
- Slides: 55
CHAPTER 17 Late Adulthood: Physical and Cognitive Development
Physical Development
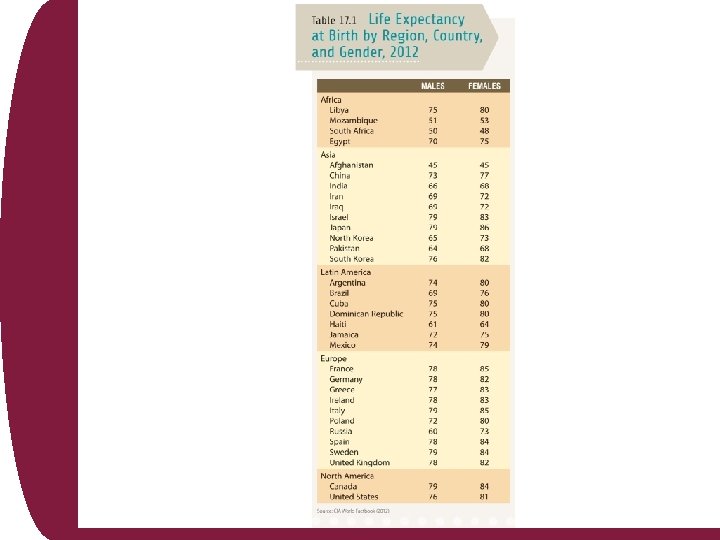
Physical Development: Longevity and Life Expectancy • Life expectancy – number of years a person in a given population can expect to live – has increased due to better medicines and vaccinations – is different for members of different cultures – Asian American women living in “America One” can expect to live to be 80 years old, whereas African American men living in “America Eight” may expect to live to be 60 years.
Gender Differences in Life Expectancy • Longevity gap between men and women is narrowing – Life expectancy among men trails that among women by about 5 years (76 years for men versus 81 years for women). • Contributing factors to difference include – heart disease occurring later in women due to drop off of estrogen – other diseases such as HIV/AIDS being more prevalent in men – men avoiding medical attention until problems are exacerbated
Fig. 17 -1, p. 351
Physical and Social Changes • Ageism – Prejudice against older people • Chemical changes of aging can lead to vision disorders such as cataracts and glaucoma. • Cataracts cloud the lenses of the eyes, reducing vision – Outpatient surgery for correcting cataracts is routine • Glaucoma – – – Buildup of fluid pressure inside the eyeball Can lead to tunnel vision or blindness Rarely occurs before age 40 Heritable Affects about one in 250 people over the age of 40 Treated with medication or surgery
Physical Changes (cont’d) • Presbycusis – Age-related hearing loss that affects about one person in three over the age of 65 – Hearing ability tends to decline more quickly in men than in women – Hearing aids magnify sound and can compensate for hearing loss. • Sense of smell decreases almost nine fold from youth to advanced late adulthood – Lose taste buds in the tongue with aging – Foods must be more strongly spiced to yield the same flavor
Physical Changes (cont’d) • Bones lose more density in late adulthood, becoming more brittle and vulnerable to fracture. – Bones in the spine, hip, thigh, and forearm lose the most density as we age. • Osteoporosis – Disorder where bones lose so much calcium that they become prone to breakage – Estimated 10 million people in the United States over the age of 50 have osteoporosis of the hip (USDHHS, 2005) – Osteoporosis results in more than 1 million bone fractures a year in the U. S. • Most serious are hip fractures • Often result in hospitalization, loss of mobility, and in people in advanced late adulthood, death from complications
Sleep • Older people need about 7 hours of sleep per night. – insomnia and sleep apnea more common in later adulthood • Sleep apnea – Person stops breathing repeatedly during the night, causing awakenings – Linked to increased risk of heart attacks and strokes • Sleep problems may involve physical changes that bring discomfort. – May symptomize psychological disorders – Other contributing factors may be men with enlarged prostate glands needing to urinate during the night, causing awakening and loneliness
Sleep • Sleep medications most common treatment for insomnia – Medicines can lead to dependence when used regularly, and to “rebound insomnia” when discontinued – Older people can benefit from developing healthier sleep habits, such as limiting daytime napping and keeping a regular sleep schedule, challenging exaggerated worries about the consequences of remaining awake, and using relaxation techniques. • Sleep apnea may be treated with surgery to widen the upper airways that block breathing or by the use of devices such as a nose mask that maintains pressure to keep airway passages open while sleeping.
Sexuality • People do not lose their sexuality as they age. • Sexual daydreaming, sex drive, and sexual activity all tend to decline with age, but sexual satisfaction may remain high. • Older people with partners usually remain sexually active. • Most older people report they like sex; a majority state orgasm is important to sexual fulfillment. • Sexual activity is influenced by psychological well-being, feelings of intimacy, and cultural expectations.
Changes in Women • Changes in older women stem from a decline in estrogen production. • Vaginal walls lose elasticity and grow paler and thinner; sexual activity may become irritating; thinning of the walls may place greater pressure against the bladder and urethra during sex leading now and then to urinary urgency and burning urination. • Vaginal changes – Labia majora lose much of their fatty deposits and become thinner – Vaginal opening constricts making penile entry difficult – Following menopause, women produce less vaginal lubrication, and lubrication may take minutes to appear; lack of adequate lubrication is main reason for painful sex.
Changes in Women (cont’d) • Changes may be slowed or reversed through estrogenreplacement therapy. – Natural lubrication may be increased through more elaborate foreplay. – Artificial lubricants can ease problems. – Older men will likely need more time to become aroused as well. • Women’s nipples still become erect as they are sexually aroused. – Spasms of orgasm become less powerful, fewer in number; orgasms may feel less intense, even though the experience of orgasm may remain just as satisfying.
Changes in Men • Age-related changes occur more gradually in men than in women. – Not clearly connected with any one biological event • After about age 50, men take longer to achieve erection. – Erections are less firm possibly due to lowered testosterone levels • Older men may require prolonged direct stimulation of the penis to obtain an erection. – Extending foreplay addresses this issue • Most men capable of erection throughout their lives – Erectile dysfunction not inevitable with aging – Men generally require more time to reach orgasm as they age.
Changes in Men (cont’d) • Testosterone production declines gradually from age 40 to age 60, then begins to level off. – Decline not inevitable and may be related to the man’s general health – Sperm production tends to decline – Viable sperm may be produced by men into their 70’s, 80’s and 90’s. – Regaining erection takes longer • Nocturnal erections diminish in intensity, duration, and frequency. – They do not normally disappear altogether • Older men produce less ejaculate; contractions of orgasm become weaker and fewer; may enjoy orgasm as thoroughly as he did at a younger age; following orgasm, erection subsides more rapidly
Patterns of Sexual Activity • Older people can lead a fulfilling sex life; years of sexual experience may compensate for any lessening of physical response. • Frequency of sexual activity tends to decline with age because of hormonal changes, physical problems, boredom, and cultural attitudes. • Sexuality among older people is variable; some engage in sexual activity as or more often as when younger; some develop an aversion to sex; others lose interest.
Patterns of Sexual Activity (cont’d) • Couples can adapt to the physical changes of aging by broadening their sexual repertoire to include more diverse forms of stimulation such as oral-genital stimulation, pornography, anal stimulation, vibrators • Sexual satisfaction may be derived from manual or oral stimulation, cuddling, caressing, and tenderness, as well as intercourse to orgasm. • Availability of a sexually interested and supportive partner may be the most important determinant of continued sexual activity.
Theories of Aging
Theories of Aging • Cellular clock theory – Focuses on the built-in limits on cell division – After dividing about 50 times, human cells cease dividing and eventually die. – Cells from longer-lived species divide more times before they die than cells from shorter-lived species. • Hormonal stress theory – Focuses on the endocrine system – Hormonal changes foster age-related changes such as puberty and menopause. – Stress hormones are left at elevated levels following illnesses, making the body more vulnerable to chronic conditions such as diabetes, osteoporosis, and heart disease.
Theories of Aging (cont’d) • Immunological theory – Holds that the immune system is preset to decline by an internal biological clock • Free-radical theory – Attributes aging to damage caused by the accumulation of unstable molecules called free radicals – Free radicals are produced during metabolism by oxidation, possibly damaging cell proteins, membranes, and DNA. – Damage may cause us to age faster and become more vulnerable to diseases associated with aging
Theories of Aging (cont’d) • Cross-linking theory – As we age, cell proteins bind to one another in a process called cross-linking, thereby toughening tissues. – Cross-linking stiffens collagen. – Collagen is the connective tissue supporting tendons, ligaments, cartilage, and bone. • Results in coarse, dry skin; believes the stiffening of body proteins accelerates and eventually breaks down bodily processes, leading to some of the effects of aging – Immune system combats cross-linking, but becomes less able to do so as we age
Health Concerns and Aging
Health Concerns and Aging • Older people typically need more healthcare than younger. – They occupy 25% of the hospital beds • Medicare – Federally controlled health insurance program for older Americans and the disabled, only partially subsidizes the health care needs of these groups • Medicaid – Another federal program – Covers a portion of the healthcare costs of people of all ages who are otherwise unable to afford coverage – Many older adults use both programs
Figure 17 -2 p 358
Health Concerns and Aging (cont’d) • Most older adults don’t need institutional care. – Two out of three older adults age 65 and older live in own homes – Less than 10% of older adults live in nursing homes or other long-term care facilities – Nursing homes are mostly made up of people age 80 and above – If older adults live long enough, half will require some form of nursing or home healthcare. • Most older Americans spend later years in retirement community – Majority of older adults remain in their own communities after retirement • Americans aged 65 and above are less likely than general population to live under the poverty level
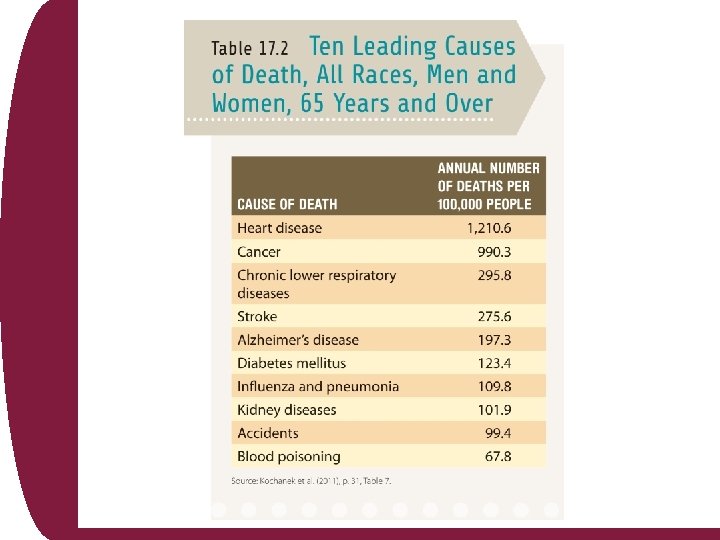
Heart Disease, Cancer, and Stroke • Three major causes of death of Americans age 65 and over are heart disease, cancer, and stroke • Heart disease – Nation’s leading cause of death among both sexes beyond the age of 80 • Cancer – Leading cause of death of women age 40 to 79, and men age 60 to 79 – Risk of cancers rises as we age due to immune system becoming less able to rid the body of precancerous and cancerous cells
Heart Disease, Cancer, and Stroke (cont’d) • Older people not adequately screened for cancer – Physicians not as aggressive in treating them – Same is true for heart disease and serious illnesses – May be due to elder bias • discrimination against the elderly on the part of some health professionals. • Dominant form of heart disease among those 65 and older is coronary artery disease resulting from atherosclerosis • Other common cardiovascular disorders in older adults – Hypertension, heart arrhythmias, and congestive heart failure
Heart Disease, Cancer, and Stroke (cont’d) • Hypertension – Affecting about 50% of Americans over the age of 65 – Major risk factor for heart attacks and strokes – Diabetes is the fifth leading cause of death – Other chronic conditions include • cataracts, chronic sinusitis, visual impairment, and varicose veins
Arthritis • Arthritis – Joint inflammation that results from conditions affecting the structures inside and surrounding the joints – Symptoms progress from redness to heat, swelling, pain, and loss of function – More common with advancing age – More common in women than men – More common in African Americans than European Americans
Arthritis (cont’d) • Osteoarthritis – – – – Painful, degenerative disease involving wear and tear on joints By age 60, half of Americans show some signs of the disease Among people over the age of 65, two of three have the disease Joints most commonly affected are in the knees, hips, fingers, neck, and lower back More common among obese people because excess weight adds to the load on the hip and knee joints Health professionals use over-the-counter anti-inflammatory drugs and prescription anti-inflammatory drugs to help relieve pain and discomfort In severe cases, joint replacement surgery may be needed Specific exercises are prescribed
Arthritis (cont’d) • Rheumatoid arthritis – Characterized by chronic inflammation of the membranes that line the joints because the body’s immune system attacks its own tissues – Affects the entire body – Can produce unrelenting pain and eventually lead to severe disability – Bones and cartilage may be affected – Disease begins between 40 and 60; anti-inflammatory drugs are used to treat it
Substance Abuse • 40% of all prescription drugs in the U. S. are taken by people age 60 and above, more than half of them take two to five medications daily. • Most commonly used drugs are – blood pressure medications, tranquilizers, sleeping pills, and antidepressants • Millions of older adults run the risk of becoming addicted to prescription drugs, especially tranquilizers. – A quarter of a million older adults are hospitalized each year because of adverse drug reactions.
Substance Abuse (cont’d) • Reasons for addiction or adverse reactions include – doctors prescribing an incorrect dosage – some people misunderstanding directions or being unable to keep track of their usage – many older people having more than one doctor, so treatment plans not being coordinated • Many older adults suffer from long-term alcoholism. – Health risks of alcohol abuse increase with age – Slowdown in the metabolic rate reduces the body’s ability to metabolize alcohol, increasing the likelihood of intoxication – Combination of alcohol and other drugs, even prescription drugs, can be dangerous, even lethal
Accidents • Older people face greater risks of unintentional injuries. • Accidents – Ninth leading cause of death among older Americans – Falls especially dangerous for older adults with osteoporosis • Accidents could be prevented by equipping the home with safety features such as railings and nonskid floors. – Wearing proper glasses and using hearing aids can reduce risk of accidents resulting from vision or hearing problems, including many motor vehicle accidents – Adherence to safe driving speeds is important because older adults have slower reaction times
Dementia and Alzheimer’s Disease • Dementia – Condition characterized by dramatic deterioration of mental abilities involving thinking, memory, judgment, and reasoning • Dementia is not a consequence of normal aging – Involves a disease process that damages brain tissue – Some causes of dementia include brain infections such as meningitis, HIV infection, and encephalitis – Chronic alcoholism, infections, strokes, and tumors – Most common cause is Alzheimer’s disease (AD) • Progressive brain disease affecting 4 -5 million Americans
Dementia and Alzheimer’s Disease (cont’d) • Alzheimer’s disease – About one in 10 Americans over the age of 65 has AD, jumping to more than one in two among those in the 75 to 84 year age range; AD is rare in people under the age of 65. – Some dementias may be reversible, such as those caused by tumors and treatable infections, or those that result from depression or substance abuse, but the dementia resulting from AD is progressive and irreversible.
Fig. 17 -3, p. 361
Figure 17 -4 p 361
Dementia and Alzheimer’s Disease (cont’d) • AD is the fifth leading killer of older Americans. • AD begins with subtle cognitive and personality changes where people with AD have trouble managing finances and recalling recent events. – Continues with people with AD finding it harder to manage daily tasks, select clothes, recall names and addresses, and drive – Progresses to having trouble using the bathroom and maintaining hygiene – People with AD no longer recognize family and friends or speak in full sentences. – They may become restless, agitated, confused, and aggressive
Dementia and Alzheimer’s Disease (cont’d) • People with AD may get lost in stores, parking lots, even in their own homes. – May experience hallucinations or paranoid delusions, believing that others are attempting to harm them – People with AD may eventually become unable to walk or communicate and become completely dependent on others. • Scientists believe that both environmental and genetic factors are involved. • Medicines can help improve memory functioning of people with AD, but effects are modest.
Cognitive Development
Memory: Remembrance of Things Past and Future • Retrospective and prospective memories – Memories of the past (“retro”) and memories of the things we plan to do in the future – Can be divided into explicit and implicit memories • Explicit memories – Specific information • Things we did or things that happened to us • General knowledge, such as the author of Hamlet • Implicit memories – More automatic – About performance of tasks • Reciting the alphabet or multiplication tables, riding a bicycle
Explicit versus Implicit Memories • Working memories of older adults hold less information simultaneously than the working memories of young adults. • Temporal memory of older adults – Recall of the order in which events have occurred may become confused • Do not fare as well as younger adults in tasks that measure explicit memory, but tend to do nearly as well in tasks that assess implicit memory
Associative Memory • Older adults have greater difficulty discriminating between new and already experienced combinations of items on an associative recognition task. • Two theories why there is a deficit in associative memory – Binding hypothesis • Older adults are impaired primarily at associating items with one another, but not at remembering individual items – Impairment in recollection theory • When the individual attempts to retrieve the information that may reflect poor binding during encoding, poor use of strategic processes during retrieval, or both
Associative Memory (cont’d) • Cohn et al. (2008) believe the frontal regions—executive center of the brain—are involved in directing one’s attention and organizing information and strategic processes. – Medial temporal lobe binds elements to form memory traces, recovers information in response to use of proper memory cues, and is a key to recollection – Neurological research indicates deterioration evident in aging in the frontal lobes and to a lesser degree in the medial temporal lobe, which impairs binding, recollection, and the use of effective strategies for the retrieval of information
Long-Term Memory • Bahrick and colleagues (2008) conducted research on recollection of grades on college graduates from early adulthood through late adulthood. – Number of correct recollections fell off with the age of the respondent, due, generally, to errors of omission • Leaving items blank rather than entering the wrong grade – Graduates who were out of school more than 40 years entered no more wrong grades, on average, than those who were out of school 8 years or so.
Fig. 17 -5, p. 324
Long-Term Memory (cont’d) • People seem to recall events from the second and third decades of life in greatest detail and with the most emotional intensity. – May be due to hormones
Prospective Memory • Prospective memory – The attempt to remember things we have planned to do in the future • despite the passage of time • despite the occurrence of interfering events – For prospective memory to succeed, we need to have foolproof strategies, such as alarms going on or off on our cell phones, or we need to focus our attention and keep it focused. – Distractibility will prevent us from reaching the goal. – Even if fluid intelligence remained intact, prospective memory might decline.
Prospective Memory (cont’d) • Age-related decline in prospective memory – Greatest when the task to be completed is not all that crucial and the cues used to jog the memory are not very prominent – When the task is important and older adults use conspicuous cues to remind them, age-related declines in prospective memory are reduced – The adults have to be cognitively intact enough to plan the strategy
Language Development • Knowledge of the meaning of words can improve into late adulthood. • Due to decline in working memory and also due to impairments in hearing, many older adults find it more difficult to understand the spoken language. – Speakers need to slow down and articulate more clearly so older people’s comprehension will increase. • Older adults may show deficiencies in language production. – Declines in associative and working memory decrease the likelihood that words will “be there” when older people try to summon up ideas. – Older people are more likely to experience “tip-of-the-tongue” phenomenon.
Problem Solving • Experiments show older adults use – fewer strategies – display slower processing speed in solving complex math problems than younger adults • Abstract problem-solving ability – As in complex math problems, is not related to older adults’ quality of life – “Real-world” or everyday problem-solving skills are crystallized; experiences with people play a helpful role • Younger versus older – – More likely to express feelings of anger or frustration Seek support from other people to solve interpersonal problems Older adults focus on remaining calm and unperturbed Difference due to older adults’ decreased tendency to express anger and increased priority on regulating emotion
Wisdom • Distractibility may contribute to wisdom – Hasher (2008) suggests distractibility can enable older adults to take a broader view of situations. • Kunzmann and Baltes (2005) – People with wisdom approach life’s problems by addressing the meaning of life by including the past, present, and future, and the contexts in which the problems arise. – People with wisdom tend to be tolerant of other people’s value systems. – Acknowledge that there are uncertainties in life and that one can only attempt to find workable solutions in an imperfect world – Ardelt (2008 a, 2008 b) suggests that wise people tend to possess an unselfish love for others and also to be less afraid of death.