Chapter 1 Abnormal Behavior in Historical Context Outline

Chapter 1 Abnormal Behavior in Historical Context

Outline Understanding Psychopathology Historical Conceptions of Abnormal Behavior § The Supernatural Tradition § The Biological Tradition § The Psychological Tradition The Present § The Scientific Method § An Integrative Approach

Focus Questions How do psychologists define a psychological disorder? What is a scientist-practitioner? What supernatural influences were formerly believed to explain abnormal behavior? How do psychological approaches including psychoanalysis, humanism and behaviorism explain abnormal behavior?

What is a Psychological Disorder? Psychological dysfunction associated with distress and/or impairment in functioning Involves a response that is not typical or culturally expected May include cognitive, behavioral and/or emotional elements

Distress, Impairment and Cultural Context Distress is normal in some situations Dysfunctional distress occurs when person is much more distressed than others would be Impairment: Must be pervasive and/or significant § Mental disorders are often exaggerations of normal processes (e. g. , extreme shyness or sadness) Culture: Consider “normalcy” relative to behavior of others in same cultural context Rule of thumb: Mental disorder = harmful dysfunction

What is a Psychological Disorder?

An Accepted Definition Behavioral, psychological, or biological dysfunctions that are unexpected in their cultural context and associated with present distress and/or impairment in functioning, or increased risk of suffering, death, pain, or impairment

The Science of Psychopathology: Scientific study of psychological dysfunction Mental health professionals § The Ph. D. : Clinical and counseling psychologist (trained in research and delivering treatment) § The Psy. D. : Clinical and counseling “Doctor of Psychology” (trained in delivering treatment) § M. D. : Psychiatrist § Psychiatric nurses § LICSW: Licensed clinical social worker (trained in delivering treatment)
 and research mutually influence each other A scientist-practitioner: §")
The Scientist-Practitioner Practice (treatment delivery) and research mutually influence each other A scientist-practitioner: § Stays current with research in field § Evaluates own assessment and treatment § Conducts research

The Scientist-Practitioner

Clinical Description Begins with the presenting problem § Symptoms (e. g. , chronic worry, panic attacks) Description aims to: § Distinguish clinically significant dysfunction from common human experience Describe prevalence and incidence of disorders

Clinical Description

Clinical Description Describe onset of disorders § Acute vs. insidious onset Describe course of disorders § Episodic, time-limited, or chronic course Prognosis § Good vs. guarded Consider age of onset, which may shape presentation

Causation, Treatment and Outcome Etiology § What contributes to the development of psychopathology? Treatment development § How can we help alleviate psychological suffering? § Includes pharmacological, psychosocial, and/or combined treatments

Historical Conceptions of Abnormal Behavior Major psychological disorders have existed across time and cultures Perceived causes and treatment of abnormal behavior varied widely, depending on context

Historical Conceptions of Abnormal Behavior Three dominant traditions have existed in the past to explain abnormal behavior § Supernatural § Biological § Psychological

The Supernatural Tradition Deviant behavior as a battle of “Good” vs. “Evil” § Believed to be caused by demonic possession, witchcraft, sorcery § Treatments included exorcism, torture, religious services

The Supernatural Tradition § “Stress and melancholy” = anxiety and depression § Competing view that coexisted with supernatural tradition: “insanity” is caused by emotional stress, not supernatural forces § Treatments: Rest, sleep, healthy environment, baths, potions § Possession Mental illness sometimes believed to reflect possession by evil spirits Treated by shocking/scaring out spirits (e. g. , hang patient over snake pit)

The Supernatural Tradition Mass hysteria § Saint Vitus’s Dance/Tarantism Modern mass hysteria § Emotion contagion § Mob psychology The moon and the stars § Paracelsus: Swiss physician suggested that mental health problems are affected by pull of moon and stars Led to term “lunatic”
 § Father of modern Western medicine §")
The Biological Tradition Hippocrates (460 -377 BC) § Father of modern Western medicine § Etiology of mental disorders = physical disease § Hysteria “the wandering uterus” – psychological symptoms were a result of the uterus moving around in the body § Linked abnormality with brain chemical imbalances Foreshadowed modern views § Galen (129 -198 AD) extended Hippocrates’ work

Galenic-Hippocratic Tradition Humoral theory of disorders: Functioning is related to having two much or too little of four key bodily fluids (humors) § Blood, phlegm, black bile, yellow bile § Example: Depression caused by too much black bile § Treated by changing environmental conditions (e. g. , reducing heat) or bloodletting/vomiting
 and the biological link with madness §")
The 19 th Century General paresis (syphilis) and the biological link with madness § Several unusual psychological and behavioral symptoms § Pasteur discovered the cause – a bacterial microorganism § Led to penicillin as a successful treatment § Bolstered the view that mental illness = physical illness

The 19 th Century John P. Grey and the reformers § Psychiatrist who believed mental illness had physical roots § Championed biological tradition in the U. S. § Led to reforms of hospitals to give psychiatric patients better care

The Development of Biological Treatments Psychotropic medications became increasingly available in 1950 s Electric shock Crude surgery Insulin (discovered by accident to calm psychotic patients) Major tranquilizers (discovered mid-20 th C) Minor tranquilizers (e. g. , benzodiazepines) – commonly prescribed for anxiety today

Consequences of the Biological Tradition Overall, mental illness understood to have physical roots Increased hospitalization § Mental illness often seen as “untreatable” condition Improved diagnosis and classification § Emil Kraepelin was father of classification Increased role of science in psychopathology

The Psychological Tradition The rise of moral therapy § Became popular in first half of 19 th century § “Moral” = referring to psychological/emotional factors § Main idea: Treat patients as normally as possible in normal environment § More humane treatment of institutionalized patients § Encouraged and reinforced social interaction

The Psychological Tradition Proponents of moral therapy § Philippe Pinel and Jean-Baptiste Pussin – patients shouldn’t be restrained § Benjamin Rush – led reforms in U. S. § Dorothea Dix – mental hygiene movement Asylum reform > more patients getting care § Moral therapy declined because more difficult with large groups of patients Soon followed by emergence of competing alternative psychological models

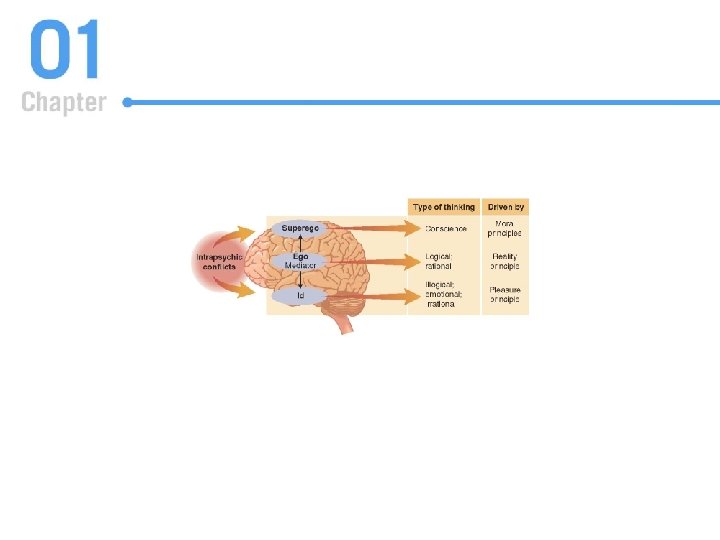
Psychoanalytic Theory Freudian theory of the structure and function of the mind § Unconscious § Catharsis § Psychoanalytic model sought to explain development and personality) Structure of the mind § Id (pleasure principle; illogical, emotional, irrational) § Superego (moral principles) § Ego (rational; mediates between supergo/id)

Psychoanalytic Theory Defense mechanisms: Ego’s attempt to manage anxiety resulting from id/superego conflict § Displacement & denial § Rationalization & reaction formation § Projection, repression, and sublimation Psychosexual stages of development § Oral, anal, phallic, latency, and genital stages § Theory: conflicts arise at each stage and must be resolved

Later Developments in Psychoanalytic Thought Anna Freud and self-psychology § Emphasized influence of the ego in defining behavior Melanie Klein, Otto Kernberg, and object relations theory § Emphasized how children incorporate (introject) objects § Objects – significant others and their images, memories, and values
 The “Neo-Freudians”: Departures from Freudian thought De-emphasized the")
Later Developments in Psychoanalytic Thought (continued) The “Neo-Freudians”: Departures from Freudian thought De-emphasized the sexual core of Freud’s theory Examples: § Carl Jung emphasized the “collective unconscious” § Alfred Adler focused on feelings of inferiority, invented “inferiority complex”

Psychoanalytic Psychotherapy: The “Talking” Cure Unearth the hidden intrapsychic conflicts § “The real problems” Therapy is often long-term Techniques § Free association § Dream analysis Examine transference and counter-transference issues Little evidence for efficacy

Psychodynamic Psychotherapy Therapy with themes of psychoanalysis, but often shorter and more goal-directed Emphasizes conflicts and unconscious, may work to uncover rauma and active defense mechanisms Focus on: Emotional expression Avoidance and other cognitive or behavioral patterns Past experience Interpersonal experience Therapeutic relationship Wishes, dreams, fantasies

Psychoanalytic Psychotherapy Major criticism: Largely unscientific and untested Contributions § Unconscious processes have been empirically demonstrated § Emotions can be driggered by triggered by cues outside of conscious awareness § “Therapeutic alliance” is important § Defense mechanisms

Humanistic Theory Theoretical constructs § Intrinsic human goodness § Striving for self-actualization Person-centered therapy § Carl Rogers (1902– 1987) Hierarchy of Needs § Abraham Maslow (1908– 1970) § Humans fulfill basic needs first (e. g. , food, safety) before moving onto higher needs like self esteem

Humanistic Theory Person-centered therapy § Therapist conveys empathy and unconditional positive regard § Minimal therapist interpretation No strong evidence that purely humanistic therapies work to treat mental disorders § More effective for people dealing with normal life stress, not suffering from psychopathology

The Behavioral Model Derived from a scientific approach to the study of psychopathology Classical conditioning (Pavlov; Watson) § Ubiquitous form of learning § People learn associations between neutral stimuli and stimuli that already have meaning (unconditioned stimuli) § Conditioning explains the acquisition of some fears

The Behavioral Model Classical conditioning – concepts § Stimulus generalization Start to respond in the same way to similar stimuli. E. g. , a child taught to fear the color red (because it is paired with a loud, scary noise) may also fear the color orange § Extinction When the conditioned stimulus is repeatedly presented without the unconditioned stimulus, the association is weakened
 § Believed that psychology should be")
The Behavioral Model John B. Watson (1878– 1958) § Believed that psychology should be as scientific and objective as possible § “Little Albert” experiment: Baby Albert was taught to fear a white rat when it was repeatedly paired with a loud noise (classsical conditioning) Mary Cover Jones § One of the first to treat phobias with exposure and extinction of learned association
 § Law of")
The Behavioral Model - Operant Conditioning E. L. Thorndike (1874– 1949) § Law of effect: Behavior will repeated more often if it is followed by good consequences and less often if it is followed by bad consequences B. F. Skinner (1904– 1990) § Behavior “operates” on environment and is managed by consequences (rewards and punishments) § Behavior “shaping”: New behavior can be learned by reinforcing successive approximations

The Beginnings of Behavior Therapy Behavior therapy: Creating new associations by practicing new behavioral habits, and/or reinforcing useful behaviors with positive consequences Behavior therapy tends to be time-limited and direct Strong evidence supporting the efficacy of behavior therapies Example: Joseph Wolpe (1915– 1997) § Systematic desensitization: Individuals gradually exposed to fears (usually through imagination) while practicing relaxation exercises

The Present: The Scientific Method an Integrative Approach Defining and studying psychopathology § Requires a broad approach § Multiple, interactive influences Biological, psychological, social factors § Scientific emphasis continues to be very important The supernatural tradition no longer has a place in a science of abnormal behavior Advances in neuroscience and cognitive and behavioral science will add to our knowledge
- Slides: 43