Changes in Heart Rate and Heart Rate Variability

Changes in Heart Rate and Heart Rate Variability Before Ambulatory Ischemic Events 2009. 3. 21 김우영

Contents • • • Background Objectives Methods Results Conclusions 2
 • Transient myocardial ischemia and sudden cardiac death – Often preceded by")
Background (1/2) • Transient myocardial ischemia and sudden cardiac death – Often preceded by periods of changes in autonomic nervous system activity consistent with vagal withdrawal – Depressed levels of HRV also predict future cardiac morbidity and mortality in patients with coronary artery disease, congestive heart failure, valvular heart disease • Possible pathophysiologic mechanisms – Vagally mediated increases in cardiac demand – Reduced coronary blood supply due to coronary constriction 3
 • Physical exercise and mental stress – Potent triggers of myocardial ischemia")
Background (2/2) • Physical exercise and mental stress – Potent triggers of myocardial ischemia – Neural mechanisms for mental stress-induced ischemia are not well understood but are likely to involve both the parasympathetic and sympathetic nervous systems – Provoke transient decreases in the HF HRV • Spectral analysis of HRV – HF : vagal tone – LF, LF/HF : sympathetic/ parasympathetic balance • Transient variations in HRV – Validated as a measure of short term changes in autonomic tone 4

Objectives • To determine the time course of autonomic nervous system activity preceding ambulatory ischemic events – Whether indicators of decreased vagal tone precede ischemic events documented by ambulatory electrocardiography – Further compared preischemic changes during episodes of high vs. low physical and mental activities during daily life 5
 • Patients – 19 men (62. 1 ± 9. 3 years) •")
Methods (1/9) • Patients – 19 men (62. 1 ± 9. 3 years) • Stable angina, coronary artery disease • Previous positive exercise test for myocardial ischemia and evidenced ischemia during 48 h ambulatory ECG monitoring – Approved by the Institutional Review Boards – Patients gave written informed consent 6
 • Ambulatory ECG monitoring – Performed while • Anti-ischemic medications (beta-adrenergic blocking")
Methods (2/9) • Ambulatory ECG monitoring – Performed while • Anti-ischemic medications (beta-adrenergic blocking agents, calcium antagonists and long-acting nitrates) were held for greater than three half lives – – 48 h Within patient reliability Cardiodata AM recorder 2 experienced readers using a Marquette 8000 Series Holter – Artifacts removed, only ECGs in sinus rhythm 7
 • ST-segment analysis of ambulatory ECG monitoring – Ischemic response • Horizontal")
Methods (3/9) • ST-segment analysis of ambulatory ECG monitoring – Ischemic response • Horizontal or downsloping ST segment depression of ≥ 1 mm below the isolectric baseline, measured 80 ms after the J point and persisting for ≥ 60 s • Upsloping ST depression ≥ 1. 5 mm not observed • 2 experienced investigators – for each episode of ST-segment depression • Time of onset, duration and magnitude were recorded – Heart Rate • Before an ischemic event at 60, 20, 10, 4, 2 min • After 2, 10, 20, 60 min – ST depression during sleep was not included – Multiple ischemic events selectively excluded 8
 • HRV analysis – Used as indicator of autonomic activity in accordance")
Methods (4/9) • HRV analysis – Used as indicator of autonomic activity in accordance with guidelines for standardization – Assessed 60, 20, 10, 4, and 2 min before and 2, 10, 20, 60 min after ischemic event • Using a Marquette series 8000 Holter system – ECG recordings into 2 min intervals – Frequency domain parameters • FFT • Power of each frequency band was logarithmically transformed, and expressed in ln(ms^2) – LF, HF, LF/HF calculated – Physiological underpinnings of the LF, HF HRV Not 9 well understood
 • Control periods matched for heart rate – Nonischemic control periods •")
Methods (5/9) • Control periods matched for heart rate – Nonischemic control periods • Preischemic changes in HRV components – Specific to ischemic events or merely reflected fluctuations in HR ? – Selected based on the ischemic heart rate profile for each patient, with readers blinded to physical and mental activity levels • HR was selected to be the same as during the patient’s ischemic event, and the heart rates at 20 min and 10 min before ischemia were required to be the same as well – Changes in HRV for control periods were analyzed at parallel time intervals as the ischemic events 10
 • Analysis of patient diaries for physical and mental activities – Validated")
Methods (6/9) • Analysis of patient diaries for physical and mental activities – Validated diary system • To evaluate patients’ physical and mental activities throughout the day – Mental and physical activity levels coinciding with the onset of ischemia were graded on a scale from 1 to 6 – Physical activity classifications are • 1) Sleep, 2) rest, reclining, 3) talking, eating, 4) driving, dressing, 5) shopping, and 6) climbing stairs, heavy physical work – Mental activity • 1) sleep, 2) rest, reading, 3) talking, clerical work, 4) waiting. Driving, 5) concentration, 6) anger or anxiety 11
 – Cut off points for activity levels • Used to compare HRV")
Methods (7/9) – Cut off points for activity levels • Used to compare HRV trajectories occurring at low (scores < 5) versus high (scores ≥ 5) activity levels • Patients also recorded episodes of chest pain and use of nitroglycerin • Activity levels were cross tabulated with the concurrent ischemic events as well as with the nonischemic control periods • Required that a valid activity entry was made that covered the 10 min period before onset of the ischemic event 12
 • Statistical analyses – Data are presented as mean ± SD –")
Methods (8/9) • Statistical analyses – Data are presented as mean ± SD – The changes in HF, LF HRV were first analyzed across all time points before the ischemic event • ANOVA • Paired t test : only if ANOVA for change over time was statistically significant • Separate repeated measures ANOVA were performed to examine recovery patterns of HRV 13
 – The effects of physical and mental activities were examined • Mixed")
Methods (9/9) – The effects of physical and mental activities were examined • Mixed model ANOVA comparing high vs. low activity levels as between subjects factor, repeated measures of HRV as within subject factor, and differences between high vs. low activity levels in preischemic HRV trajectories were evaluated by examining the interaction term • Interaction term (“high vs. low activity” X “repeated HRV assessments”) • T-test • HR and HRV changes : Product-moment correlations • To examine… HR and HRV 14

Results • HRV before ischemic events – 68 ischemic events • 3. 6± 2. 7 episodes per patient, range from 1 to 9 • Mean duration of 9. 5± 13. 3 min (range 2 to 56 min) • All were asymptomatic – Nonischemic control periods based on matched heart rates • Obtained in 13 of the 19 patients (37 episodes) – Figure 1 • Postischemic recovery pattern of HRV – Figure 1 – Sustained postischemic HRV levels were depressed only in events triggered by high levels of mental or physical activities 15

Results • Effects of mental and physical activity – Figure 2. – Mental activity – Physical activity 16

Results • Relation between heart rate and HRV – HRV in High HR and low HR – Figure 3, Table 1 17

Depressed only in events triggered by high level of mental and physical activities No changes in LF/HF 18

Reduced HF HRV during mental stress specifically before ischemic events No effects of mental stress Reduced LF HRV 2 min before but not significant • Only LF was elevated during high physical activity • no effects of physical activity on nonischemic Control 19
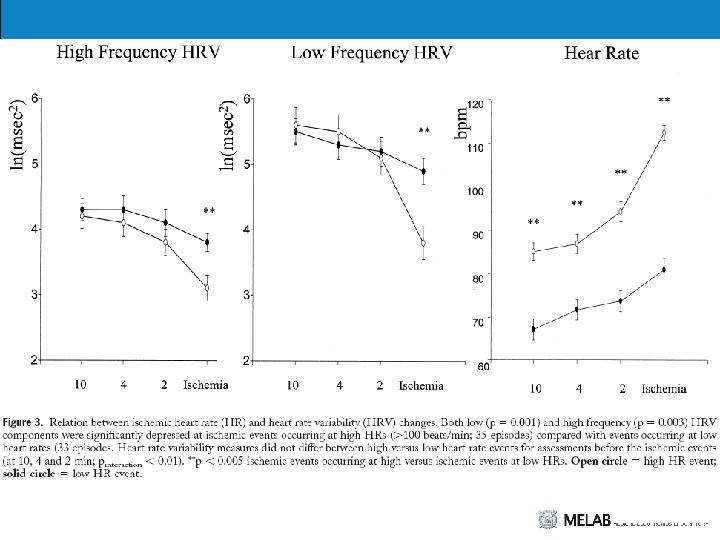

HR higher directly preceding Ischemia No significant difference in HF Only with high mental stress 21
 • Decreases in HRV precede myocardial ischemia during the activities of daily")
Discussion (1/10) • Decreases in HRV precede myocardial ischemia during the activities of daily life – Beginning at 10 min, peak at 4 min, before STsegment depression – Ischemic events occurring at high mental activities • Preceded by significantly decreased HF HRV levels – Vagal withdrawal • precedes the onset of transient myocardial ischemia • May help explain the phenomenon of mental stress induced ischemia, which typically occurs at low heart rate 22
 • Ambulatory ischemia and the time course of autonomic changes – Goseki")
Discussion (2/10) • Ambulatory ischemia and the time course of autonomic changes – Goseki et al. • Without discontinuation of beta-blocking agents – This study • Tested off anti-ischemic medications • More precisely define the trajectory of postischemic HRV changes • Assess the interrelationship between HR and HRV • Evaluate the role of physical and mental activities in HRV changes before ambulatory ischemic events – Vagal withdrawal • Found to persist until 20 min 23
 – Vagal withdrawal • Found to persist until 20 min • Sustained")
Discussion (3/10) – Vagal withdrawal • Found to persist until 20 min • Sustained HRV depression – Only observed for events occurring at high activity levels • Possible that – Transient ischemia has sustained residual effects on cardiac vagal tone, independent of activity levels – Or, ambulatory ischemia persisted for longer than detectable by ST-segment depression • Further study needed 24
 • Association of mental stress with autonomic changes and myocardial ischemia –")
Discussion (4/10) • Association of mental stress with autonomic changes and myocardial ischemia – Vagal withdrawal associated with mental activities appears to be specific to ischemic events • High mental activity levels associated with HRV decreases in ischemia, but not in nonischemic, control periods • Not confounded by potential influences of perceived pain on ANS because all ischemic events were asymptomatic – Mental stress may trigger ambulatory ischemia only if sufficient vagal withdrawal is elicited by the activity 25
 • Relations between heart rate and HRV before ambulatory ischemia – HR")
Discussion (5/10) • Relations between heart rate and HRV before ambulatory ischemia – HR and HRV are not independent factors • Mental stress induced ischemia in the laboratory and the ambulatory ischemia occur at lower HR than observed during clinical exercise testing with rapidly increasing work loads – Similar heart rates for ambulatory ischemic events triggered by mental and by exercise – Main difference between exercise and mental stress-induced ischemia may • Decreased HF HRV characterizes mental stress induced ischemia 26
 • Relations between heart rate and HRV before ambulatory ischemia – Patterns")
Discussion (6/10) • Relations between heart rate and HRV before ambulatory ischemia – Patterns of HRV preceding ischemic events did not significantly differ from HRV changes during non ischemic heart rate matched control periods • Vagal withdrawal also occurs with high HR without electrocardiographic ischemia event – The reasons of the lack of differences in HRV • ECG is not sensitive to detect ischemia at low HR • Not feasible to completely separate HR and HRV – Vagal withdrawal of cardiac vagal tone causes an increase in HR • But High mental activity was associated with a decrease in HRV variability before ischemic events but not in HR matched control independence of HRV and HR 27
 • Relations between heart rate and HRV before ambulatory ischemia – The")
Discussion (7/10) • Relations between heart rate and HRV before ambulatory ischemia – The reasons of the lack of differences in HRV • HF HRV is more accurate indicator of vagal tone compared with HR • Prospective studies have demonstrated differential predictive value of HRV over HR for adverse long term prognosis of cardiovascular disease 28
 • Study limitations – Not applicable to all coronary disease patients because")
Discussion (8/10) • Study limitations – Not applicable to all coronary disease patients because only male patients with stable disease were examined – Were not able to control for confounding effects of breathing frequency – Because this study uses ambulatory techniques to assess autonomic and behavioral precipitants of ambulatory ischemia – Based on observation, not under experimental control 29
 • Study limitations – Events rather than patients • Multiple events of")
Discussion (9/10) • Study limitations – Events rather than patients • Multiple events of one individual patient • Same number of events but in different patients – Heart rate variability is an indirect measure of cardiac autonomic tone; direct measures are not feasible during ambulatory studies – 128 SPS is not optimal for LF HRV 30
 • Clinical implications – Activity induced changes in the sympathovagal balance •")
Discussion (10/10) • Clinical implications – Activity induced changes in the sympathovagal balance • Involved in triggering myocardial ischemia • Prognostic value of decreased HRV for cardiac disease progression may be mediated, in part, by exercise and mental stress induced autonomic changes – Beta blockers may be beneficial in the treatment of myocardial ischemia – Decreased vagal activity • occurs as early as 10 min before the electrocardiographic evidence of ischemia • Vagomimetic agent such as scolpolamine will be beneficial for the treatment of refractory myocardial ischemia 31
- Slides: 31