Cestoda Dr E B Kia School of Public

Cestoda Dr. E. B. Kia School of Public Health Tehran University of Medical Sciences
 -cestoda (tapeworms) ● Nemathelminth (round worms)")
Helminth ● Platyhelminth -trematoda (flukes) -cestoda (tapeworms) ● Nemathelminth (round worms)

Fasciola hepatica

Taenia saginata

Ascaris lumbricoides

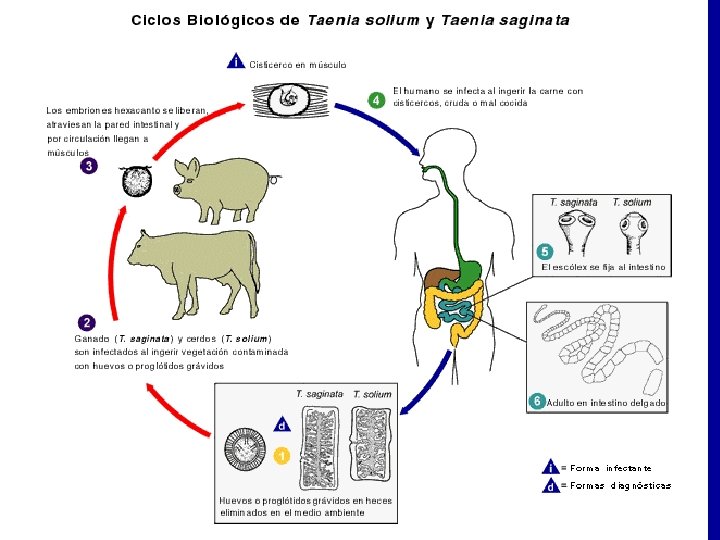
Transmission of Helminth • • • Snail Transmitted Helminthes Soil Transmitted Helminthes Meat Transmitted Helminthes Direct Transmitted Helminthes Arthropod Transmitted Helminthes

Adult cestodes in human • Taenia saginata • Taenia solium (sometimes larvae in different tissues) • Taenia asiatica • Hymenolepis nana (larvae in intestinal mucous) • Diphyllobothrium latum

Cestodes larvae in human • Hydatid cyst…. Echinococcus granulosus • Alveolar cyst…Echinococcus multilocularis • Cysticercus cellulosae…Taenia solium


Tegument- Microthrix

Onchosphere & egg embryophore
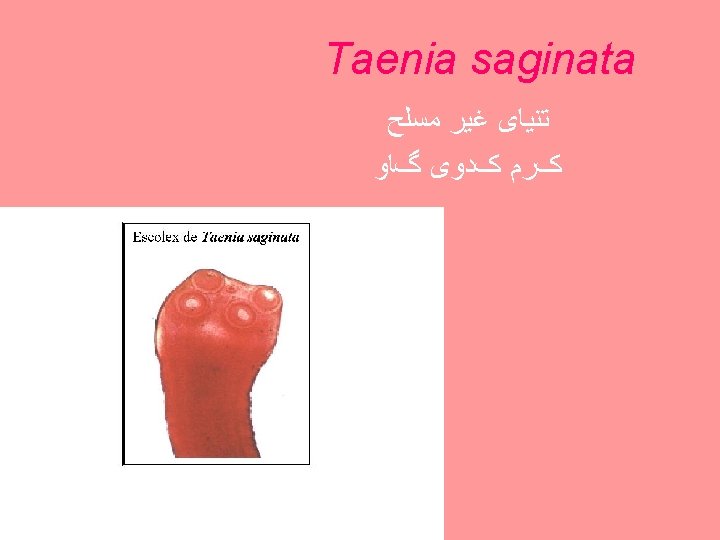

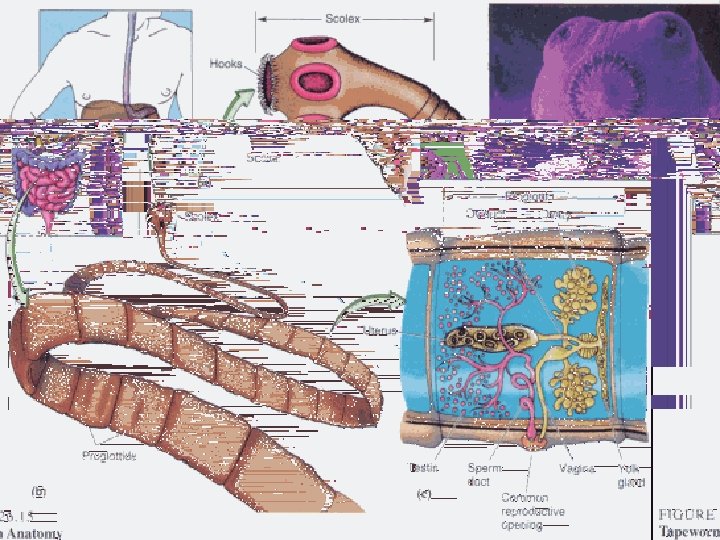
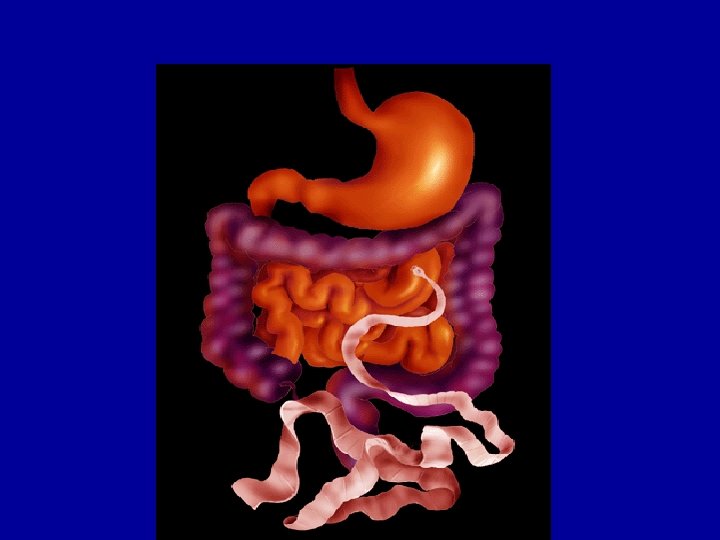
Taenia saginata • beef tape worm Location in host • The scolex of the adult tapeworm is embedded in the mucosa of the wall of the small intestine ( jejunum and ileum)

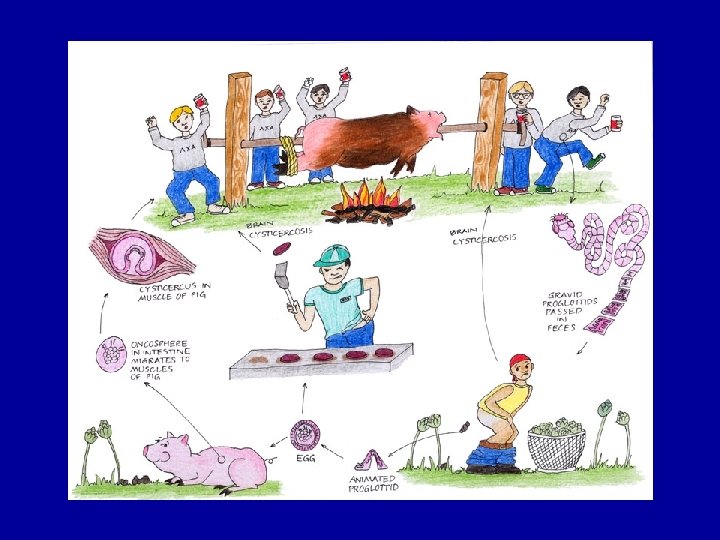
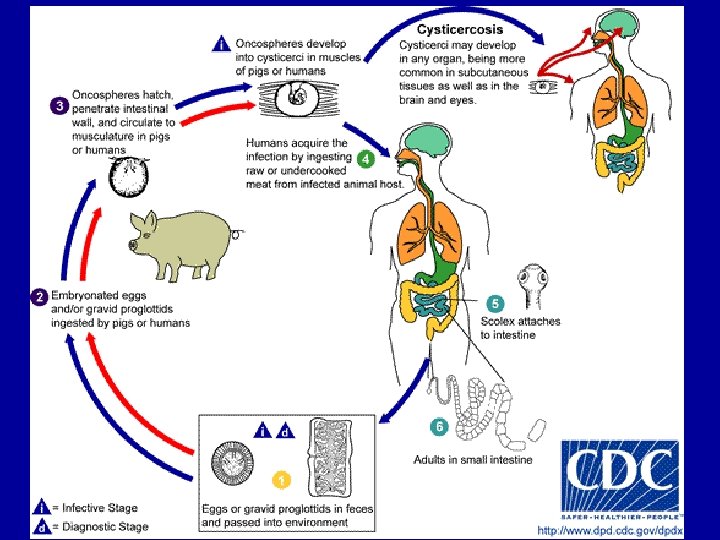
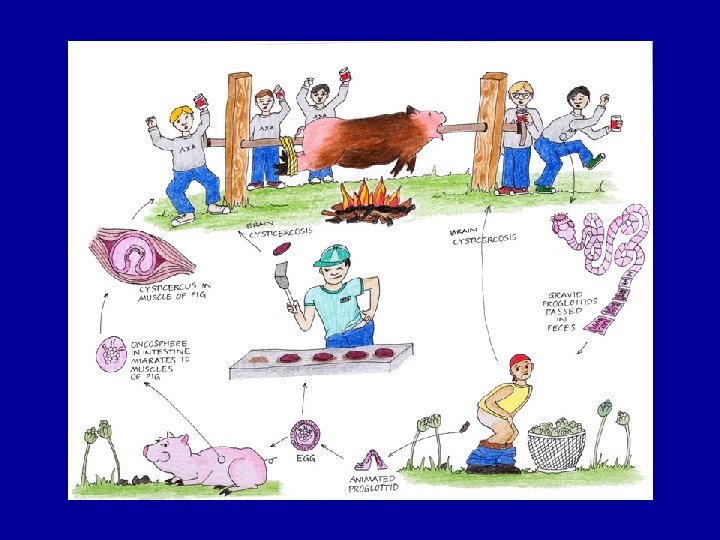
Transmission


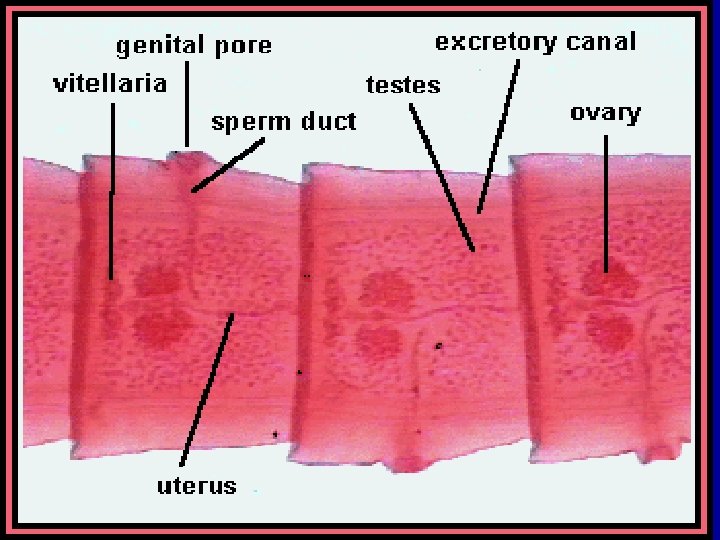
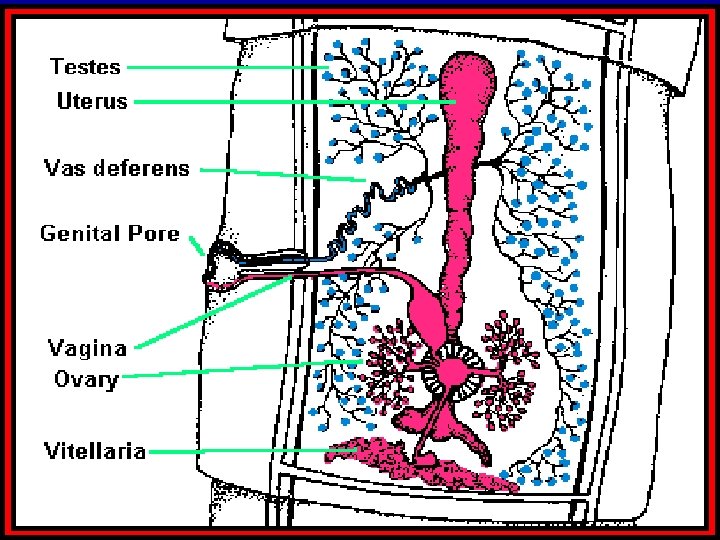
Mature proglottid
 lateral branches.")
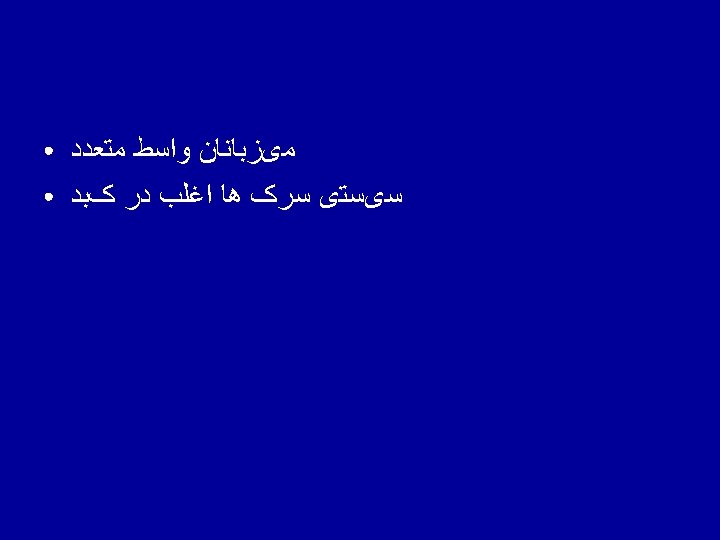
Gravid proglottides • T. saginata: 15– 32 (usually 20– 23) lateral branches.

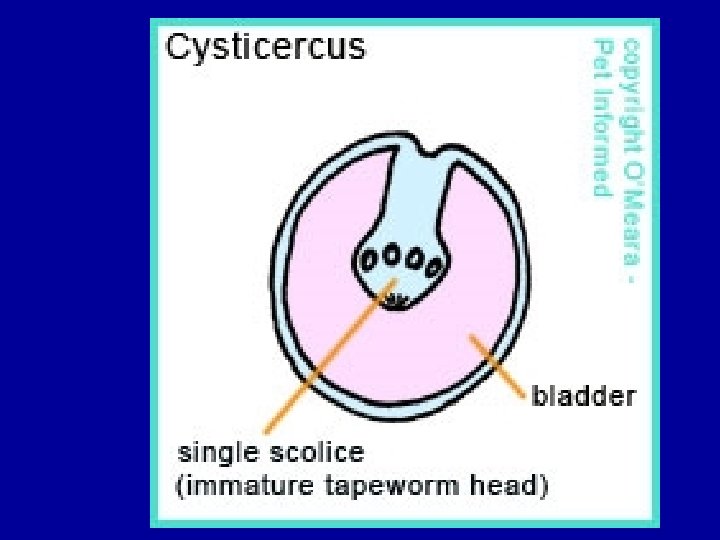
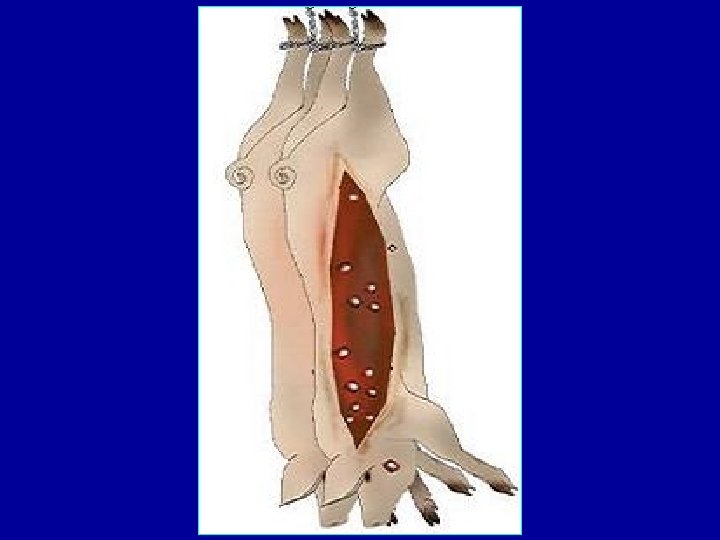
Cysticercus bovis
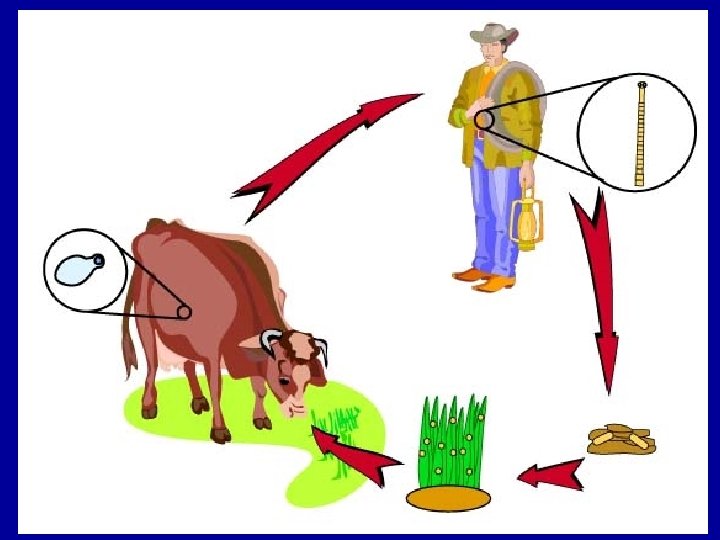

Infectivity with C. bovis




• Long life: 25 years

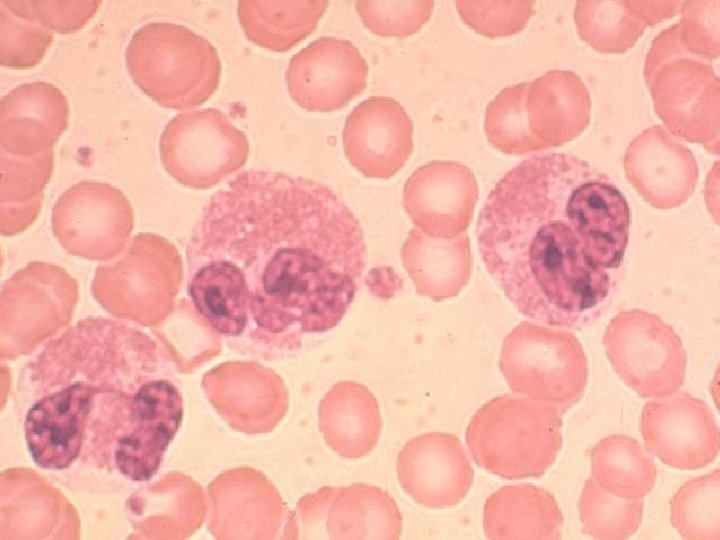
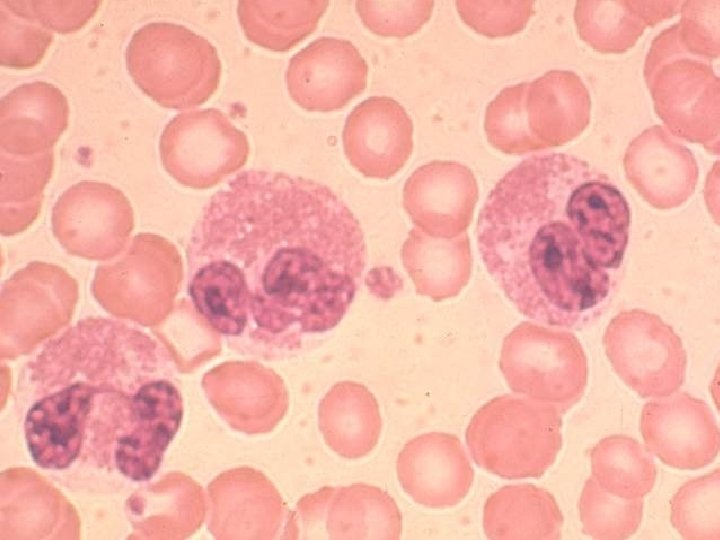
Clinical manifestations • Often only sign of infection is feeling of them ‘crawling’ out through the anus. • epigastric pain, stomach ache- nausea, weakness, loss of weight, alteration of appetite, and headache. • allergic reactions such as urticaria and pruritus • presence of a lump in the throat • intestinal obstruction and appendicitis • A moderate eosinophilia occurs in 5– 45% of patients.

Clinical manifestations constipation -diarrhea – dizziness- headache Migrating proglottids can cause: inflammation of the appendix) inflammation of the bile duct) Cholangitis/ appendicitis, obstruction -unpleasant surprise when seen in the feces.
)")
Symptoms • • Vague abdominal discomfort Hunger pangs Chronic indigestion Moderate eosinophilia- Eos. 10%)) / Ig. E

Taenia in appendix

Diagnosis • Proglottids examination • Cellophane tape swab • Stool examination is not specific method

proglottid


Taenia saginata

Onchosphere & egg embryophore
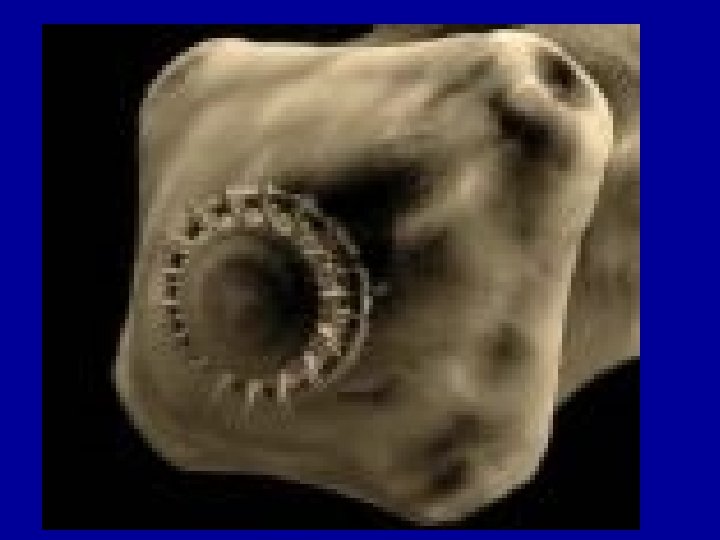
 4 x 500 mg, Side effects Scolex Praziquantel,")
Treatment • • • Niclosamide (Yomesan) 4 x 500 mg, Side effects Scolex Praziquantel, 5 -10 mg/kg, single dose Mode of action
: a single oral dose of 5– 10 mg/ kg Niclosamide (90%):")
Treatment Praziquantel (100%): a single oral dose of 5– 10 mg/ kg Niclosamide (90%): • adult: 2 g • children aged 2– 6 years: 1 g • side-effects

Prevention & Control

Health Education

Proper cooking

Freezing

Meat inspection

Taenia saginata • • • • Beef tapeworm Morphology Life cycle Adults: 4 -6 mm; scolex: 1 -2 mm; gravid s. : 16 -20 x 5 -7 mm; mature s. : 12 mm; proglottids: 1000 -2000 Long life: 25 years Cysticercous bovis: 5 -9 mm; development: 12 -15 weeks; degeneration: after one year Geographical distribution/ Iran, world No. of adults Symptomology Cholangitis/ appendicitis, obstruction Pathology Eos. / Ig. E Diagnosis Treatment

Taenia asiatica • • • Epidemiology Morphology Life cycle Symptomology Diagnosis Control & treatment

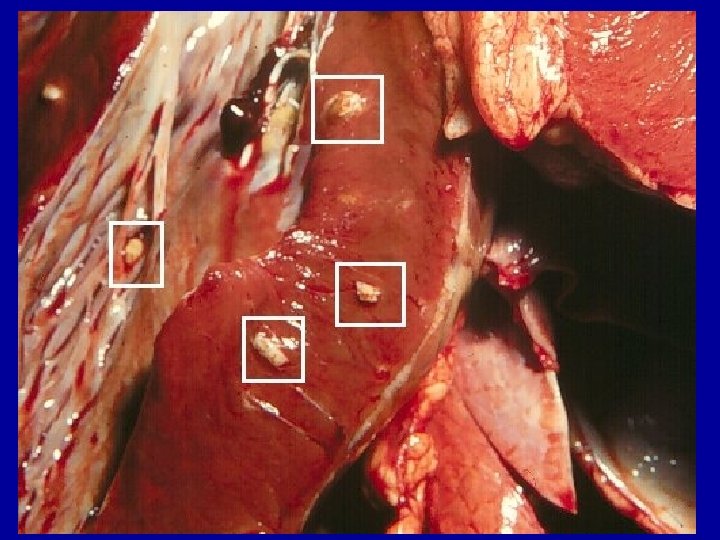
Cysts of Taenia asiatica in the liver of intermediate host

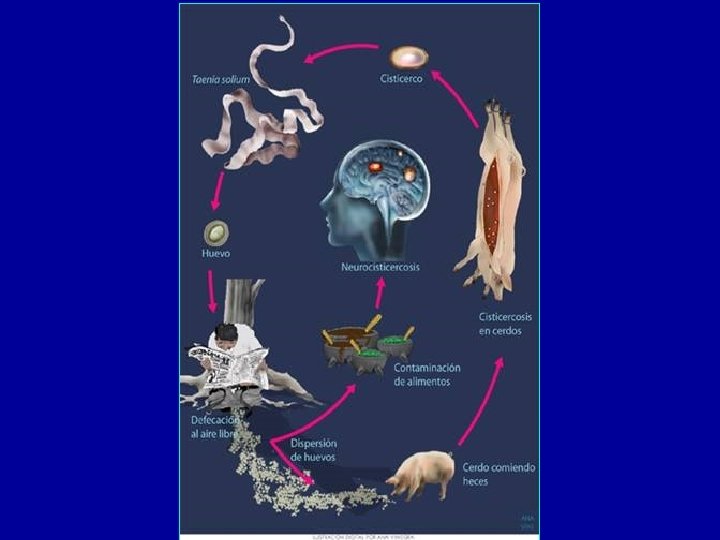
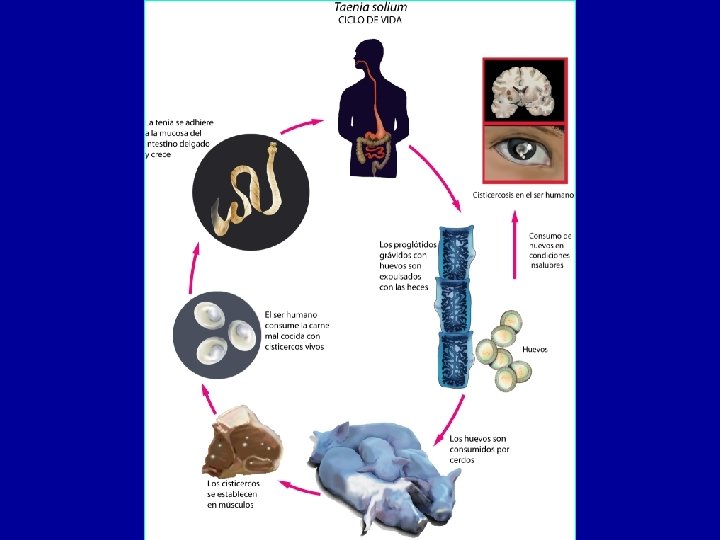
Taenia solium


Taenia saginata


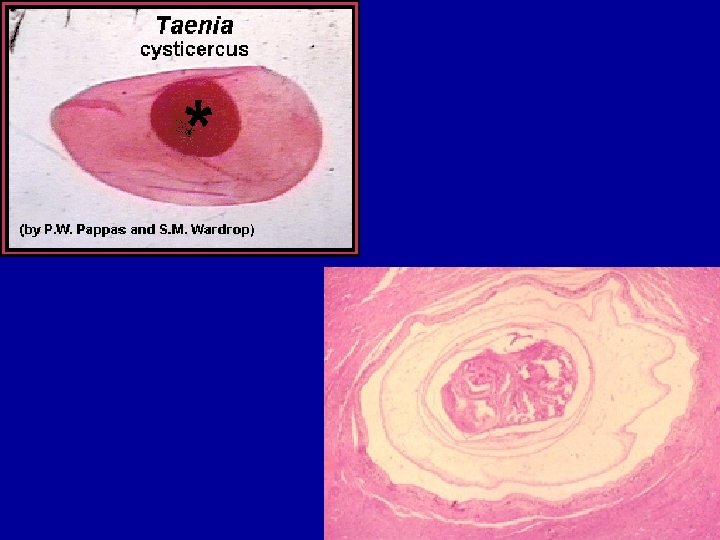
Cysticercous cellulosae

Clinical manifestations of taeniasis • Usually no distinct clinical signs. • Sometimes abdominal pain, with diarrhoea or constipation • loss of weight and weakness. • There is often an eosinophilia of 10– 13%.

Treatment of taeniasis • Give an antiemetic and follow treatment • Praziquantel at 5– 10 mg/ kg in a single oral dose is usually completely effective. • Niclosamide at an oral dose of 2 g for an adult • minor side effects

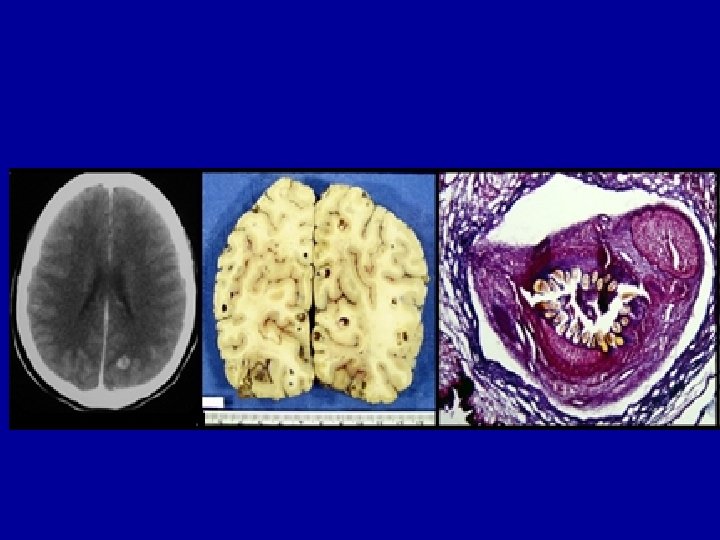
neurocysticercosis

Convultion

Racemose cysticercosis

Neurocysticercosis • • The most common parasitic D. of CNS Epileptic seizure Intracranial hypertension Headache, vomiting, vertigo, behavior disturbances, … • Cerebral edema

NEUROCYSTICERCOSIS • Cysticerci in the brain are initially viable but do not cause much inflammation in surrounding tissues; this phase of infection is usually asymptomatic. • The host develops a state of immune tolerance to the parasite, and cysticerci can remain in this stage for many years. • Clinical manifestations frequently develop when an inflammatory response develops around a degenerating cysticercus. – It is not known what triggers this degeneration, but after a variable number of years, the cyst seems to lose its ability to modulate the host immune response.

NEUROCYSTICERCOSIS • If symptoms are present, these are mainly due to mass effect, an inflammatory response, or obstruction of the foramina and ventricular system of the brain. • The symptoms of NCC depend upon the stage, site, and number of cysticerci. • The most common symptoms include seizures, focal neurological signs, and intracranial hypertension.

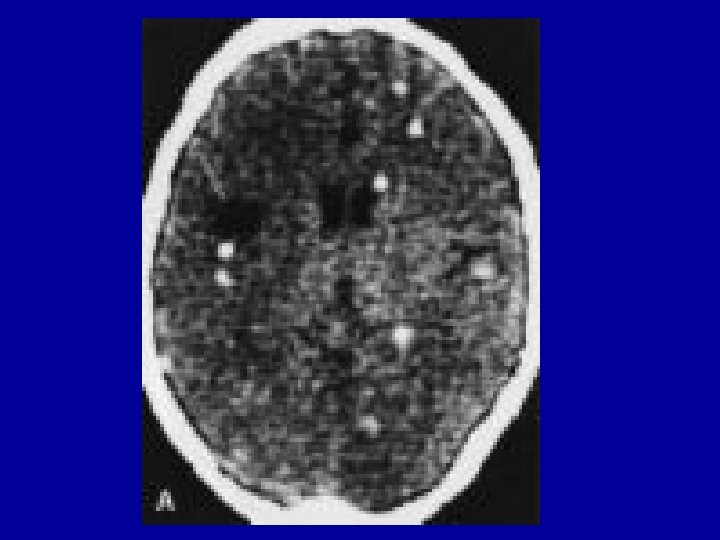
NEUROCYSTICERCOSIS • The peak of NCC has been estimated to occur three to five years after infection, but it can be delayed for >30 years. • After a variable period of degeneration, cysts can become calcified and may then become inactive. • Once they are calcified, they may cease to cause symptoms or may serve as a focus for epileptic activity. • Patients frequently have cysts in more than one location, and it is not uncommon to have active and inactive cysts present in the same patient.

Ocular cysticercosis • Ocular cysticercosis occurs in approximately one to three percent of all infections. • Patients with ocular cysticercosis may have parasites located in the subretinal space or vitreous humor. • These are often asymptomatic, but inflammation around degenerating cysticerci can threaten vision by causing chorioretinitis, retinal detachment, or vasculitis. • Parasites may also be present in the anterior chamber or may affect the conjunctiva or extraocular muscles. • Ocular cysticercosis should be excluded by a proper ophthalmologic examination in all patients with NCC prior to initiating therapy.

Ocular cysticercosis

Cysticercosis in eye

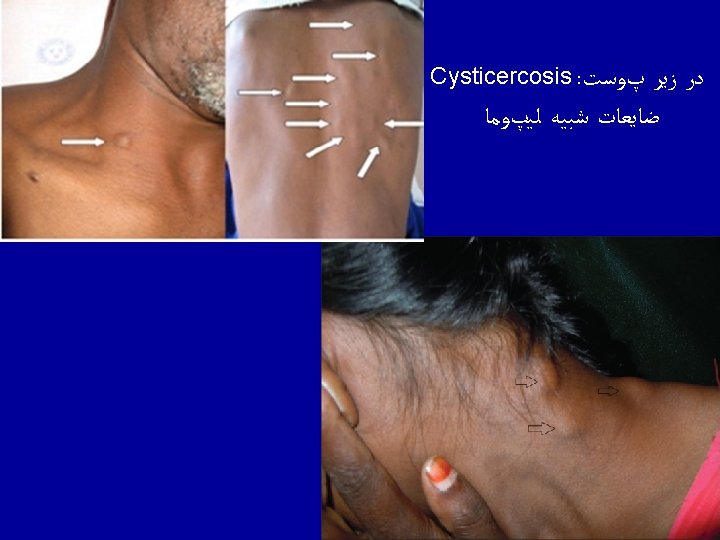
Subcutaneous and intramuscular cysticercosis • Cysticerci can develop in almost any body site, but tend to have a predilection for muscle or subcutaneous tissues. • Cysticerci at these sites are usually asymptomatic, but the patient may notice subcutaneous, pea-like or walnutsized nodules. • Subcutaneous nodules are more common in patients from Asia and Africa than from Latin America. • In cases of major muscle involvement, acute myopathy can develop. Both subcutaneous and intramuscular cysts often undergo calcification and may be detected incidentally when radiographs are performed for unrelated problems. • Cysts have also been found in the heart. Depending upon the location of the cysts, these may be asymptomatic or may result in arrhythmias and/or conduction abnormalities.


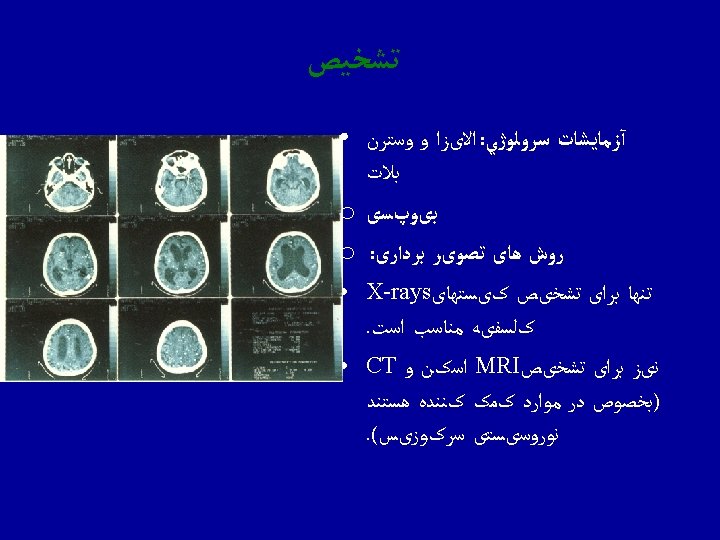
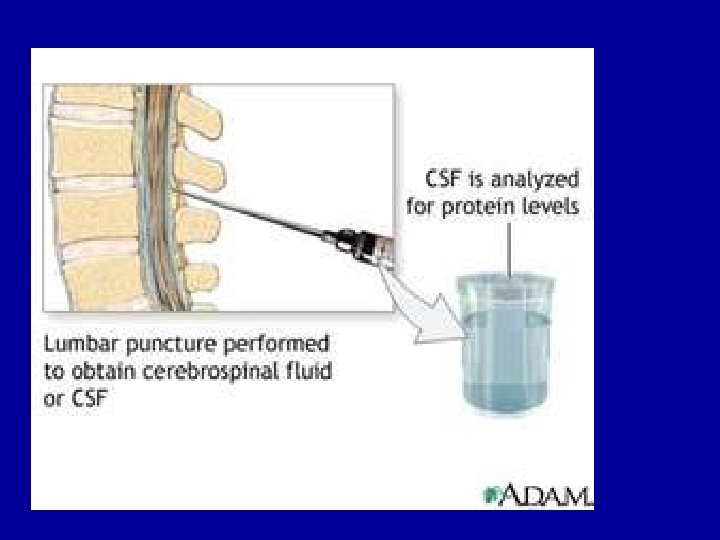
Diagnosis


Eye Examination

Management: Management Anti helminthic agents Tab. Albendazole 15 mg/kg daily x 1 month Tab. Praziquantel 50 mg/kg/day x 15 days Steroids Anti epileptic drugs Surgery

Praziquantel

Albendazole. Mode of action

Corticosteroid

Surgery

Control

Health Education

Meat inspection

Proper cooking

Freezing

- Slides: 110