CESAREAN Most common major surgical procedure in the







, blood type, antibody screen indirect coombs AB")


 (inferior epigastric arterie)")
")






 Pull Fetal pillow Round head (difficult) Encircled umbilical")
 Delivery of the placenta")


 approximated by 0 or no. 1")







- Slides: 42
CESAREAN
Most common major surgical procedure in the UNITED STATES: 1/3 of births 70% Of cesarean deliveries in the UNITED STATES are primary cesareans; three common indication are: 1. Failure to progress during labor (35%) 2. Non_reasurring fetal status (24%) 3. Fetal malpresentation(19%)
Williams: 1. Maternal Prior cesarean delivery Abnormal placentation Maternal request Prior classical hysterotomy Unknown uterine scar type Uterine incision dehisence Prior full thickness myomectomy Genital tract obstructive mass Invasive cervical cancer
Prmannet cercelage Prior pelvc reconstructive sugery Prior significan perineal trauma PELVIC DEFORMITY Hsv OR HIV infection CARDIAC OR PULMONARY DISease Cerebral aneurysm or arteriovenous mlformation perimortem cesarean delivery
Maternal Fetal Cephalopelvic Failed disproportion operative vaginal delivery Placenta previa or placental abruption
FETAL Non reasusuring fetal status Malpresentation Macrosomia Congenital anomaly Abnormal umbilical cord duppler study Thrombocytopenia Prior neonatal birth trauma
Preoperative Planned term cesarean delivery at 39 or 40 w of gestation Sedative may be given at bed time the night before surgery Solid food intake stopped at least 6 – 8 hours before surgery (uncomplicated patients moderate amount of clear liquid up to 2 hours before surgery) Admit the day of surgery Antacid is given shortly before the analgesia (Bicitra, 30 ml, orally in a single dose) Left lateral tilt Five minute tracing of fetus. Minimum fetal heart rate sound. Electrosurgical pad on the lateral thigh. Intra operative normothermia lowes wound infection rate
Preoperative Anesthesia consultation Baseline Hb (one month), blood type, antibody screen indirect coombs AB Prophylaxis: without AB 5 -20 Fold greater risk of infection compared with vaginal birth/Narrow sperctrum AB within 60 min before incision such as cefazolin or ampicillin Women<120 kg=CEFAZOLIN 2 gr (Williams 1 gr) WOMEN>=120 kg= CEFAZOLIN 3 gr Half life CEFAZOLIN>AMPICILLIN/Extra doses(excessive blood loss, duration of sugery >two half lives of thec drug CEFAZOLIN+AZITHRIMYCIN 500 mg IV=IN labor or ROM FOR AT LEAST 4 H ALLERGY: CLINDAMYCIN 900 mg+Gentamycin 5 mg/kg IV Thrombo phylaxy
Fetal presentation and placental location Bladder catheterization Hair removal Skin preparation Vaginal preparation
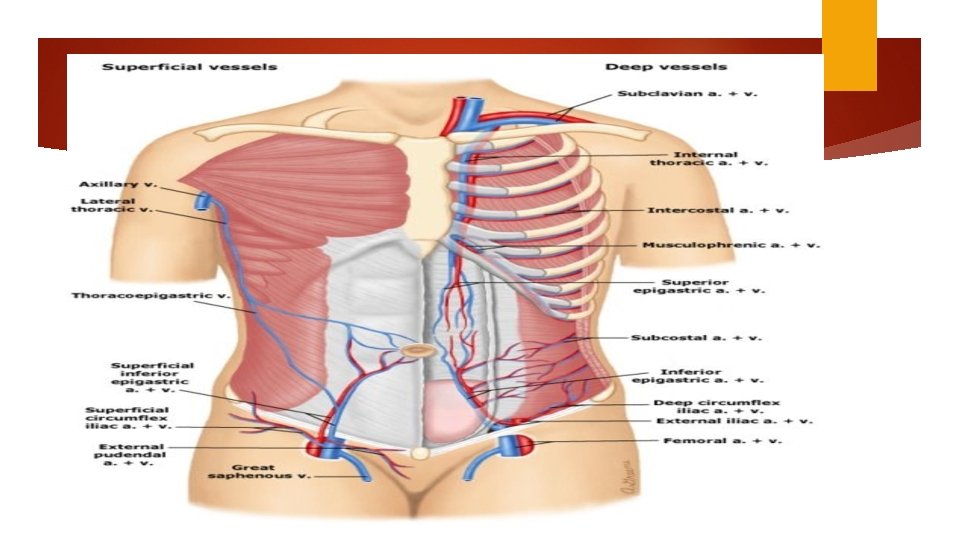
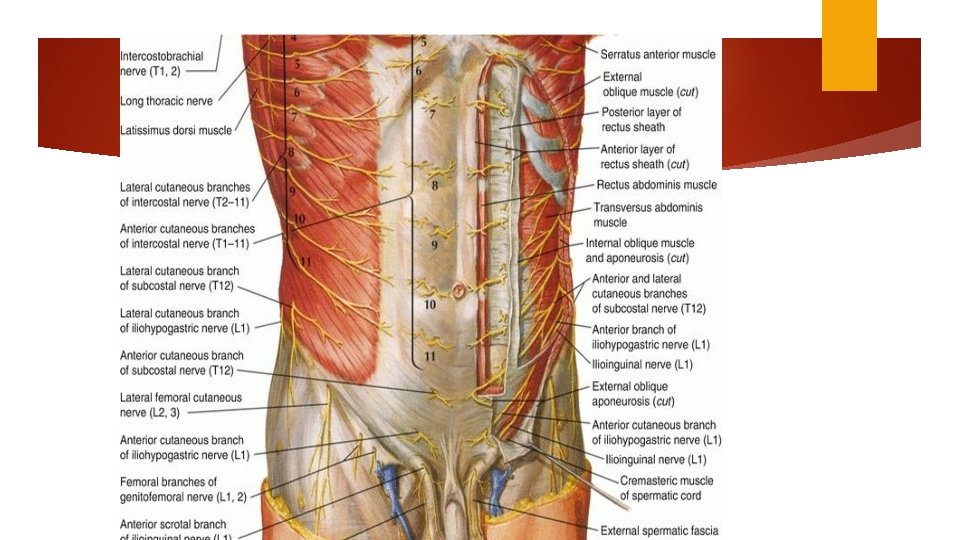
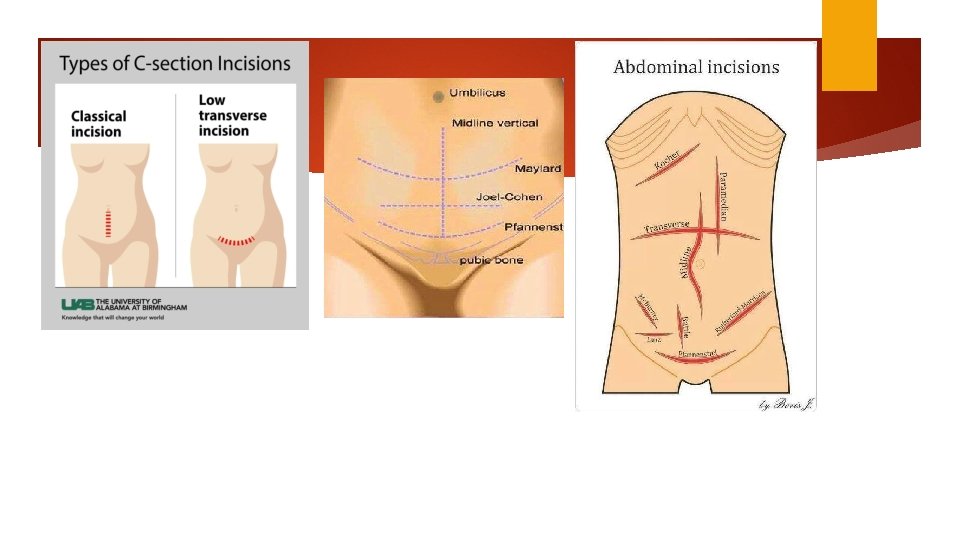
Skin incision Choice of incision — transverse skin incision: a better cosmetic appearance and possibly less postoperative pain and hernia formation. we rarely perform a vertical midline incision, we often select this approach when: The incision-to-delivery time is critical A transverse incision may not provide adequate exposure The patient has a bleeding diathesis and thus is at increased risk of subcutaneous or subfascial hematoma formation Patients with high infection risk Neurovascular structures (ilioinguinal and iliohypogastric nerves and superficial and inferior epigastric vessels) Obese patients
Transverse incision Pfannenstiel: common JOEL –Cohen Maylard incision (rectus andominies transected) (inferior epigastric arterie)
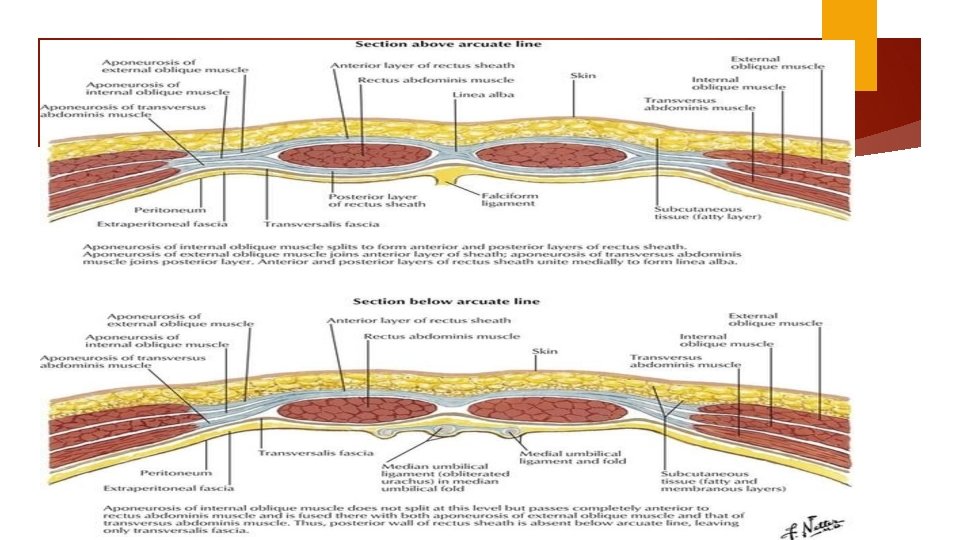
Pfannenstiel Level of pubic hair line (3 cm about superior border of symphysis pubis) 12 -15 cm Sharp dissection through the subcutaneous to the fascia (superficial epigastric vessel) Anterior abdominal fascial = aponeurosis external oblique muscle fused layer transverse abdominies + internal oblique Fascial separation cephalad 8 cm
vertical midline incision 2 to 3 cm above the superior margin of the symphysis 12 to 15 cm Sharp dissection through the subcutaneous layer Extended first superiorly then inferiorly Other stages are similar to Pfannenstiel
Subcutaneous tissue layer Fascial layer Rectus muscle layer Opening the peritoneum
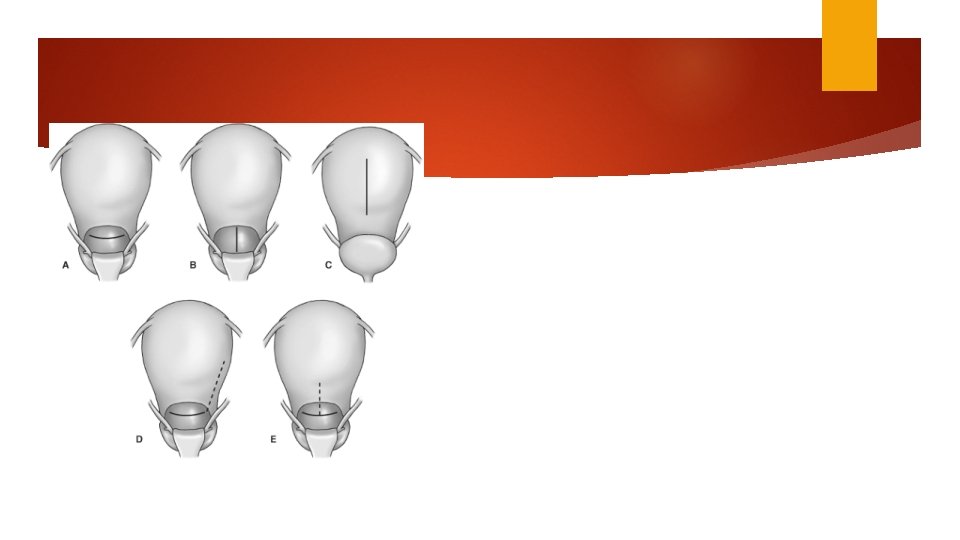
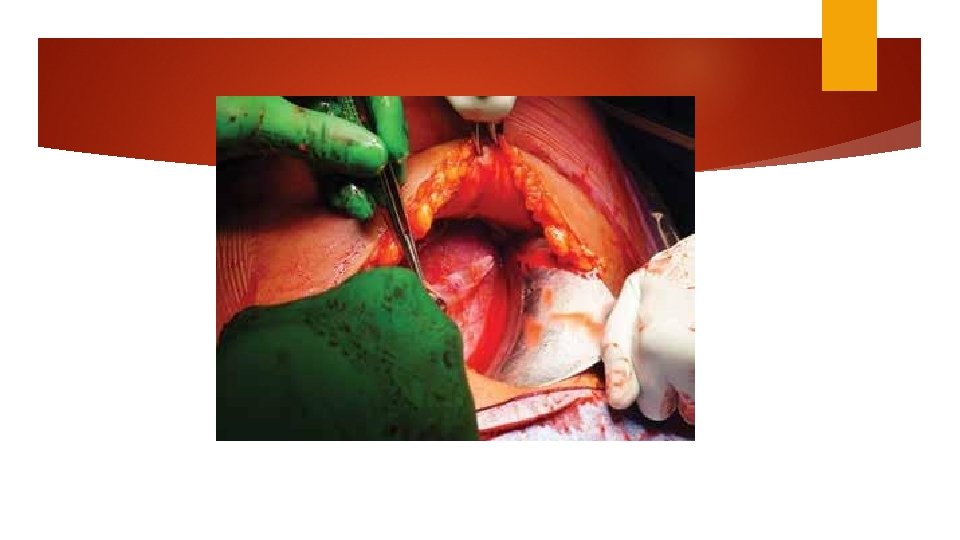
Hysterotomy Transverse incision Monro Kerr or Kerr incision Low uterine segment vertical (Kronig, De. Lee, or Cornell) classical incisions Fundal or posterior incision (placental accrete) The generally accepted indications for considering a vertical uterine incision are: ●Poorly developed lower uterine segment when more than normal intrauterine manipulation is anticipated (eg, extremely preterm breech presentation, back down transverse lie). ●Lower uterine segment pathology that precludes a transverse incision (eg, large leiomyoma, anterior placenta previa or accreta). ●Densely adherent bladder. ●Postmortem delivery. ●Delivery of a very large fetus (eg, anomalous, extreme macrosomia) when there is high risk of extension of a transverse incision into uterine vessels or a T or J extension may be required to extract the fetus.
Kerr Easier Less to repair incision-site bleeding Promote less bowel or omentum adherence to myometrial incision Less likely to rupture during subsequent pregnancy
Palpate Moist the fundus to identify uterine rotation sponge to pack protruding bowel Peritoneal Bladder edge is elevated and incised laterally flap shorter skin incision to delivery time
Uterine incision Digital palpation to find the physiological border between firmer upper segment and more flexible lower segment. Advanced 1 cervical dilation hysterotomy is higher to 2 cm Comparing blunt and sharp expansion: blunt associated with fewer unintended incision extension, shorter operative time and less blood loss.
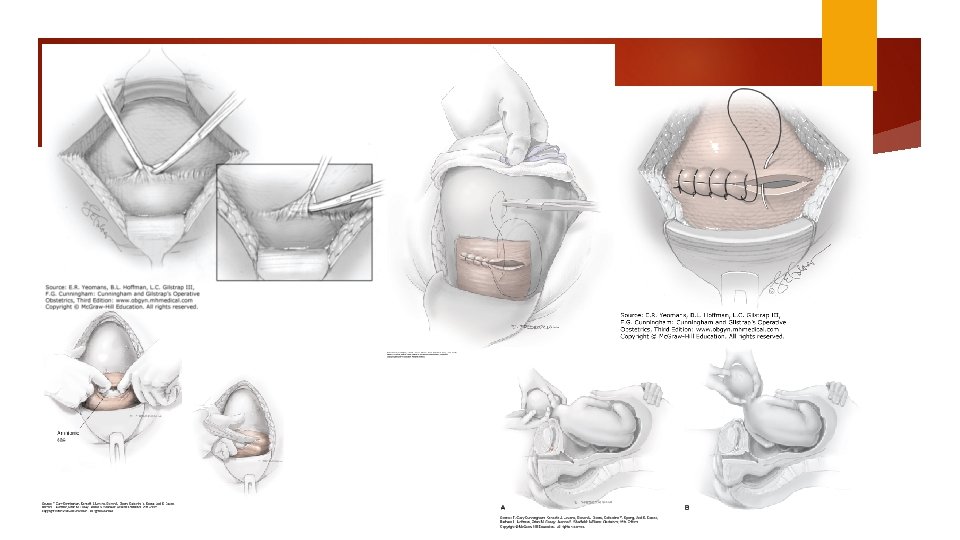
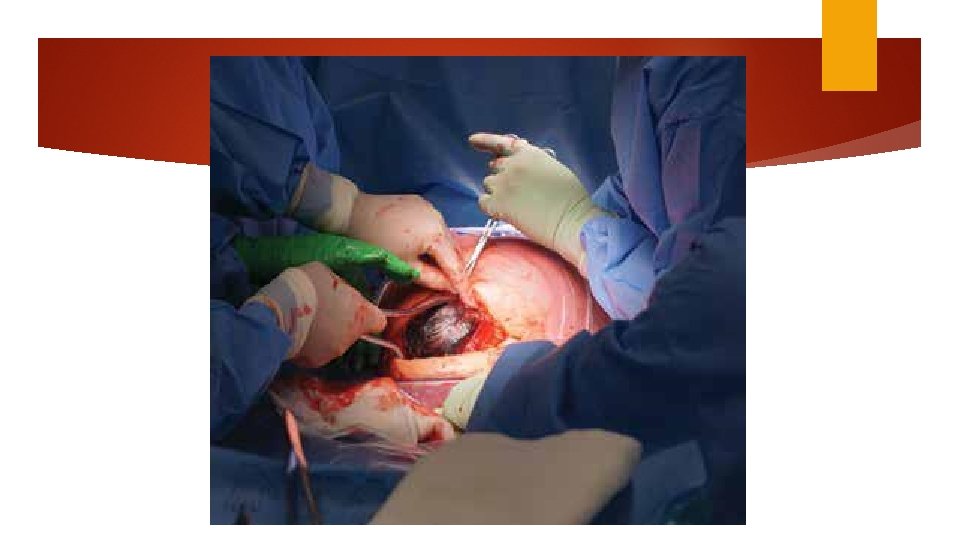
Delivery of the fetus Push (dislodge) Pull Fetal pillow Round head (difficult) Encircled umbilical cord
20 units of oxytocin per liter (10 ml/min) Delivery of the placenta
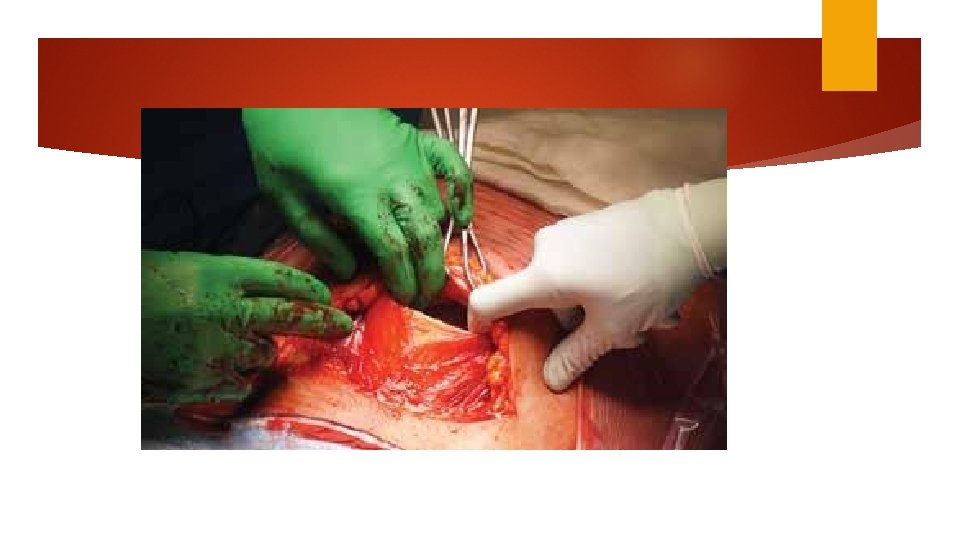
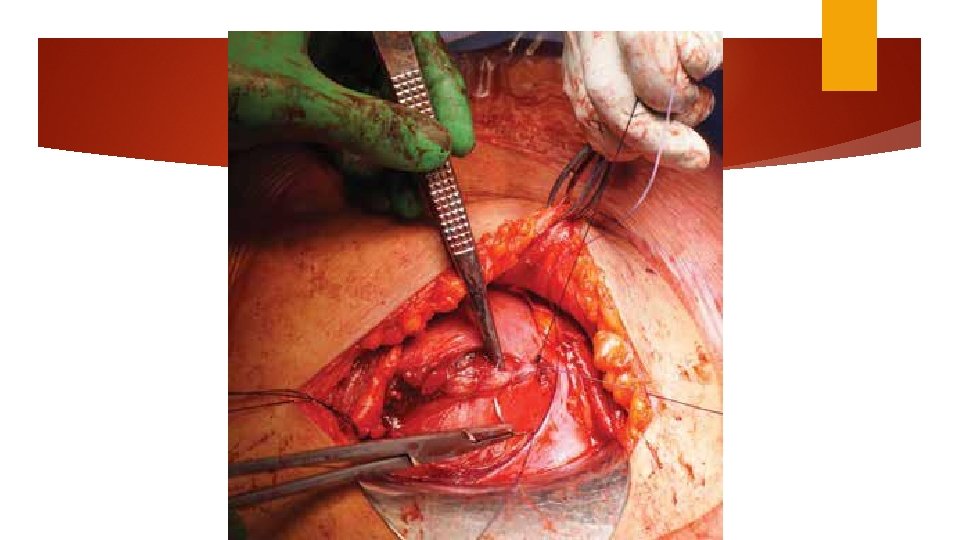
Uterine repair Uterus is lifted One or two layers of continues 0 no. 1 absorbable suture: chromic catgut / Vicryl Single layer is faster Individual bleeding site: figure of 8 or mattress
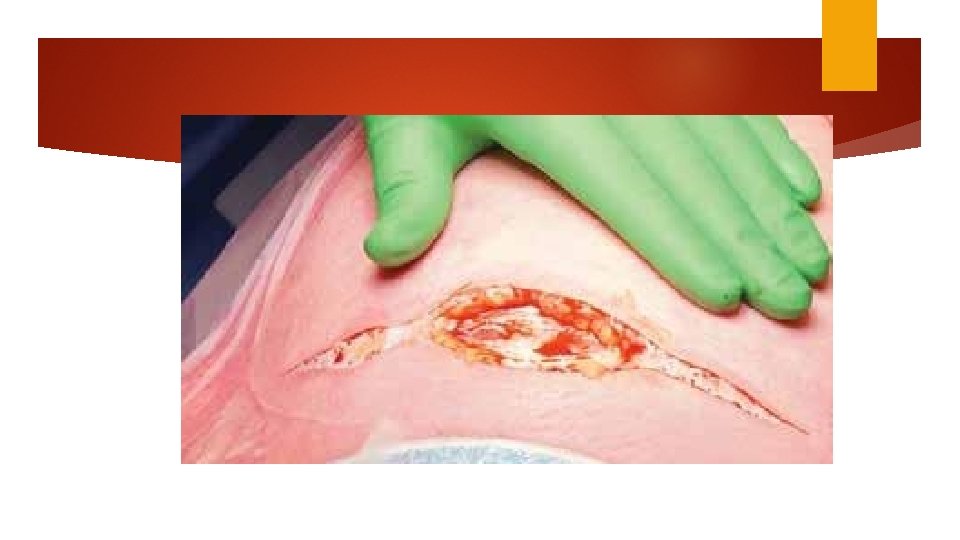
Scaring can be reduced by handling tissues delicately achieving hemostasis and minimizing tissue ischemia infection foreign body reaction No benefit to peritoneal closure No benefit of adhesion barrier
Abdominal closure Irrigation Muscle (greater intra operative nausea) approximated by 0 or no. 1 Chromic figure of 8 gut sucure. Overlying rectus fascia: continues nonlocking with delayed absorbable suture Subcutaneous Skin tissues if less than 2 cm thick need not be closed with 4 -0 delayed bsorbable
Joel-Cohen and Misgav ladach techniques Differ from Kerr by their initial incision and greater use of blunt dissection Joel-Cohen Technique: Straight 10 cm transverse skin incision 3 cm below the level of anterior superior iliac spine. Subcutaneous tissue is opened sharply. Misgav ladach technique defers in that peritoneum is interred bluntly Shorter operative time, less blood loss and post operative pain Difficult in women with adhesion or fibrosis
Uncomplicated cesarean delivery of fetus in cephalic presentation
UTERINE CLOSURE Exteriorizing the uterus