Cervical Screening Implementation and local audit Siobhan Hicks

Cervical Screening. Implementation and local audit Siobhan Hicks October 2014.
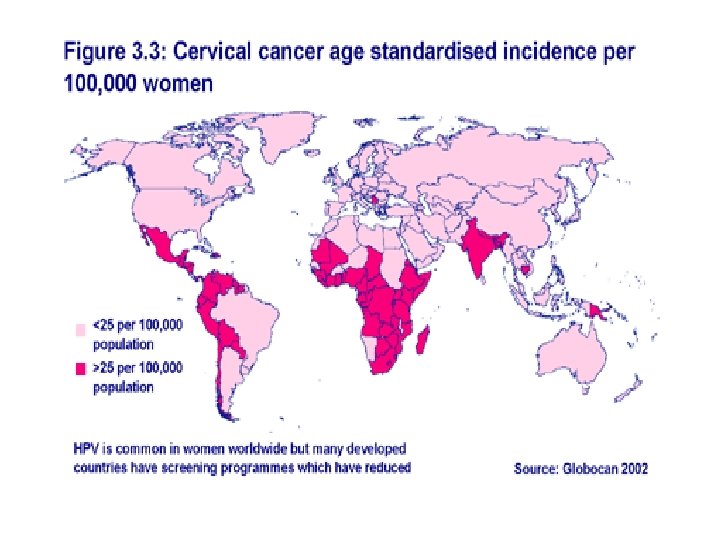

Estimated Cervical Cancer Incidence Worldwide in 2012
 of the global burden")
Incidence of cervical cancer • A large majority (around 85%) of the global burden occurs in the less developed regions, where it accounts for almost 12% of all female cancers. • High-risk regions, with estimations over 30 per 100, 000, include Eastern Africa (42. 7), Melanesia (33. 3), Southern (31. 5) and Middle (30. 6) Africa. • Rates are lowest in Australia/New Zealand (5. 5) and Western Asia (4. 4). Cervical cancer remains the most common cancer in women in Eastern and Middle Africa. http: //www. who. int/vaccine_research/en/ Accessed 10/10/12

Incidence of cervical cancer • World wide 110 female cancers diagnosed is Ca. Cx • Rate varies seven fold around the world • Highest rate is Zimbabwe, 67. 21 per 100, 000 women years • One of the Lowest rates is in China, 2 -3 per 100, 000 women years ( interpret this with caution- why? ) • *England 2010 2. 2 per 100, 000 population (The NHS Information Centre, 2011).

Implementation of the national programme nhs. cancerscreening. nhs. uk

A Brief History

• Papanicolaou's seminal publication in the 1940 s, which showed that exfoliated cervical cells could be reliably harvested and spread, fixed and stained on a glass slide, laid the foundations of cervical screening. • This technique remained virtually unchanged until the introduction of Liquid Based Cytology (LBC) and is still used all over the world in the prevention of cervical cancer.

• The gradual increase in the use of exfoliative cytology in the late 1960 s and 1970 s naturally resulted in an increase in the number of abnormal tests. This, in turn, required the means to investigate and treat cervical intraepithelial neoplasia (CIN)* without the amount of damage caused by the traditional knife cone biopsy. • *CIN = cellular changes in the cervix of the uterus preceding the invasive stages of cervical cancer.

• Colposcopy therefore, became widely adopted and treatments such as laser and large-loop excision of the transformation zone (LLETZ) have been successful. • The incidence of cervical cancer following treatment of CIN 3 is now less than 1% and the consequent death rate less than 0. 5%.

Colposcopy clinic referrals • • Persistent inadequate, Borderline changes, Mild Dyskaryosis, Moderate Dyskaryosis, Severe dyskaryosis, Potential invasive cancer, Potential Glandular Cancer……. . (Refer to NHS CSP Annual Review 2012).

The NHS Cervical Screening Programme • Until the 1980 s, cervical screening was not applied in a systematic fashion in the United Kingdom (UK). The death rate from cervical cancer was essentially unchanged until the national programme was instituted in 1988. • This programme originally involved every woman between the ages of 20 and 64 years (20– 60 years in Scotland) being called and recalled every 3– 5 years for a cervical sample test. • This managed programme introduced quality standards at every step: smear takers, cytoscreeners and colposcopy, in order to assure the quality of the process.

The NHS Cervical Screening Programme • Since 1988 – 64 million tests and >400, 000 significant abnormalities detected (NHS CSP, Annual Review 2012).
")
The NHS Cervical Screening Programme • The National Health Service Cervical Screening Programme (NHSCSP) has issued a series of guidelines governing the management of the programme. • The programme has had a dramatic effect, with a falling incidence of death from cervical cancer: the death rate is now just 50% of what it was in 1988.
 In addition to the")
The NHS Cervical Screening Programme and Public Health England (2013) In addition to the NHS Cancer Screening Programmes, other organisations including • UK National Screening Committee (NSC) • Health Protection Agency (HPA) • Joint Committee for Vaccinations and Immunisation • (JCVI) will move to PHE. The connection with vaccinations and the HPA will be particularly useful for cervical screening as it will build links with the HPV surveillance and modelling work which the HPA undertakes.
.")
EARLY DETECTION AND TREATMENT CAN PREVENT 75% OF CANCERS (NHS CERVICAL SCREENING PROGRAMME, 2009). .
 lives")
• It is estimated that 4, 500 (i. e. , in England) lives a year are saved, many in young women. The annual expenditure of £ 130 million consumed by the NHSCSP is viewed as highly cost effective.

Coverage of the Screening Programme

Coverage of the target population If overall coverage of 80% can be achieved, the evidence suggests that a reduction in death rates of around 95% is possible in the long term. (NHS Cervical Screening Programme, 2009) 2011 – *78. 6%; 2010 - 78. 9%; 2006 – 79. 5%. * % of women (aged 24 - <65 yrs) who were recorded as screened at least once in the previous five years (The NHS Information Centre, 2011).

Is the screening programme effective?
")
Effect of Cervical Screening Programme in England • 2002 – 2. 8% (927 cases) Cervical Cancer mortality rates. • 2005 – 2. 5% (841 cases) • 2010 – 2. 2. % (753 cases) (The NHS Information Centre, 2012).

Effect of Cervical Screening Programme in the UK • Efficacy of cervical screening varies with age. • Much less effective in women under 40 years. • Maximum effectiveness in post menopausal women. Sasieni et al (2003. )

Current developments HPV Vaccine

Impact of the HPV vaccine on the NHSCSP • The current vaccine are only available for high risk HPV types 16, 18. • Expected the vaccine could therefore prevent around 70% cancers • Cervarix protects against type 16 and 18 (not anal warts) • Cost of treating genital warts is £ 120 million per annum and rising • Gardasil introduced in 2012 and offered protection against warts too. • Currently no NHS vaccine offered to boys in UK – although licensed and can be accessed via private services.

HPV • HPV is a sexually transmitted disease with peak incidence in the age band 20 -24 years which gradually declines up to about the age of 40 -45 years, but then may begin to increase slowly again. • Most infections are transient, with a median duration of at most 12 months, and pose no risk of cervical neoplasia: only the 10 -20% that remain persistent are of concern. • The majority of all sexually active women will be affected by the HPV in their lifetimes • (NHS Cervical Screening Programme, 2009).

Impact of the HPV vaccine on the NHSCSP • Impact will not be seen for some years • Greater immunological response if girls are vaccinated between 10 -14. • If 10 year olds were vaccinated, it would be 10 -15 years before a decision needs to be taken whether they should be screened or not. • If older women were vaccinated, it is likely they would need to be screened for 10 -15 years as well.

Impact of the HPV vaccine on the NHSCSP • Cervarix supplied as a single dose pack. • Introduced in September 2008/9. July 2009. 12 -13 year old girls (year 8. ) 76. 4% (12 -13 yr olds) received all 3 doses. 24. 9% (17 -18 yr olds) “ “ (NHS, Cervical Screening Programme, 2009).
. Latest figures show")
Impact of the HPV vaccine on the NHSCSP • DH (2011). Latest figures show that the HPV programme is a success with >84% (13 – 14 year old girls) and 60. 4% (12 – 18 year old girls) receiving the complete course. • It has been estimated that year on year with an 80% uptake, there should be a 2/3 reduction in the incidence of cervical cancer in women aged 30 years by 2025.
, which")
HPV vaccines • There are two licensed HPV vaccines: – Gardasil. TM (quadrivalent), which protects against HPV types 16/18 and 6/11, and – Cervarix. TM (bivalent), which protects against types 16/18 only. Both vaccines are over 99% effective. The two vaccines are not routinely interchangeable

Current vaccination policy

Gardasil N. B. there was a change of from 2012 from Cervarix to Gardasil. Fifty five (55) million doses of Gardasil have Been administered world wide (DH, 2012).

HPV vaccines • Two dose schedule (for girls aged between nine years old and below 15 years of age) since March 14 • Antibody response to two doses in adolescent girls is as good as a three dose course in the age group where efficacy against persistent infection and pre-cancerous lesions has been demonstrated.

Incomplete vaccination • Previous incomplete vaccination with Cervarix® • There is no longer a NHS supply of Cervarix® available in the UK. For girls who started the schedule with Cervarix, ® but did not complete the vaccination course, the course can be completed with Gardasil®. • Green Book Chapter 18 a v 2_1

Current Screening Policy

Screening Programme Policy • • Age 25 25 -49 50 -64 65+ 1 st screening 3 yearly 5 yearly Only screen those who have not been screened since age 50, or who have recent abnormal results http: //www. cancerscreening. nhs. uk/cervical about-cervical-screening. html#invited Accessed 11/10/10

“To screen or not to screen” What about women who are not sexually active? • The NHS Cervical Screening Programme invites all women between the ages of 25 and 64 for cervical screening. But if a woman has never been sexually active, then the research evidence shows that her chance of developing cervical cancer is very low indeed. We do not say no risk, only very low risk. In these circumstances, a woman might choose to decline the invitation for cervical screening on this occasion. If a woman is not currently sexually active but has had partners in the past, then we would recommend that she continues screening http: //www. cancerscreening. nhs. uk/cervical/about-cervicalscreening. html#active [Accessed 11/10/10]

Screening programme policy Cervical Screening starts at 25 years of age recommend by: • The International Agency for Research on Cancer. • Cancer Research UK. • The Independent Advisory Committee on Cervical Screening (NHSCSP, 2009).

• Why are women under 25 not invited? Cervical screening in women aged 20 -24 is substantially less effective in preventing cancer (and in preventing advanced stage tumours) than is screening in older women (Sasieni, et al, 2009 - Effectiveness of cervical screening with age: population based case-control study of prospectively recorded data).

• HPV Testing included in the NHS CSP from April 2011.

HPV triage • Borderline and mild dyskaryosis screened for HPV • HPV found refer for colposcopy • No HPV return to normal screening

Test of cure • Reviewed in 6 m • Borderline moderate or severe dyskaryosis referred for colposcopy • No HPV return to normal screening

How can we increase uptake of cervical screening in our practice?

Think about • High risk groups • Integration with other services • ‘Hard to reach groups’

Monitor your work!

Audit • What is the uptake in your practice? • Are they any groups which are under represented? • What is your inadequate result rate? • How effective is your system to inform people of their results?

Summary. § NHS CSP effective. § Significant reduction in inadequate smear results since the introduction of LBC. § HPV and its relationship with cervical changes. § The HPV programme.
- Slides: 49