CERVICAL LYMPHADENOPATHY Dept of Oral Medicine Radiology Yenepoya




















")



- Slides: 29
CERVICAL LYMPHADENOPATHY Dept of Oral Medicine & Radiology Yenepoya Dental College Mangalore
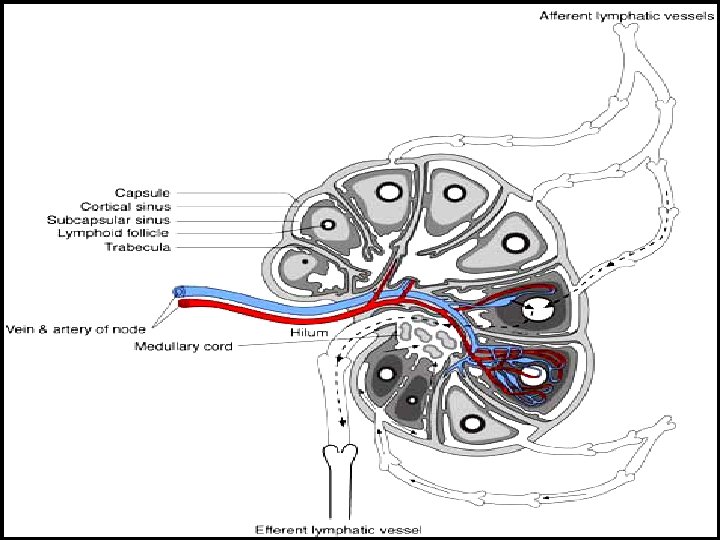
Lymphnodes are encapsulated centres of lymphocyte differetiation and proliferation
v Small, oval or reniform bodies v About 0. 1 – 2. 5 cm long v Numerous in neck, mediastinum, post abdominal wall & pelvis v about - 400 - 450 LN v Head and neck - 60 – 70 LN
FUNCTIONS v Generate mature and prime B and T cells v Add antibodies to circulation v Filter particles, microbes from lymph
1. Submental 2. Submandibular 3. Parotid 4. Upper cervical 5. Middle cervical 6. Lower cervical 7. Supraclavicular fossa 8. Posterior triangle (accessory chain)
Lymphadenitis - an inflammation or infection of lymph node and frequently occurs when an infection is present in the tissues drained by particular node pathway
CAUSES I. INFECTION BACTERIAL / VIRAL / PARASITIC II. NEOPLASIA PRIMARY SECONDARY- Ca / Malanoma III. MISCELANIOUS SARCOIDOSIS / DRUG REACTION/C T DISEASES
Infectious Causes Non-infectious causes 1. Adenovirus 1. Hodgkin's disease 2. CMV 2. Lymphomas 3. Enterovirus 3. Leukemia 4. EBV 4. Metastatic disease 5. Herpes simplex 5. Histiocytosis 6. Staphlococcus infection 6. SLE 7. Cat Scratch Diseas 7. Kawasaki Disease
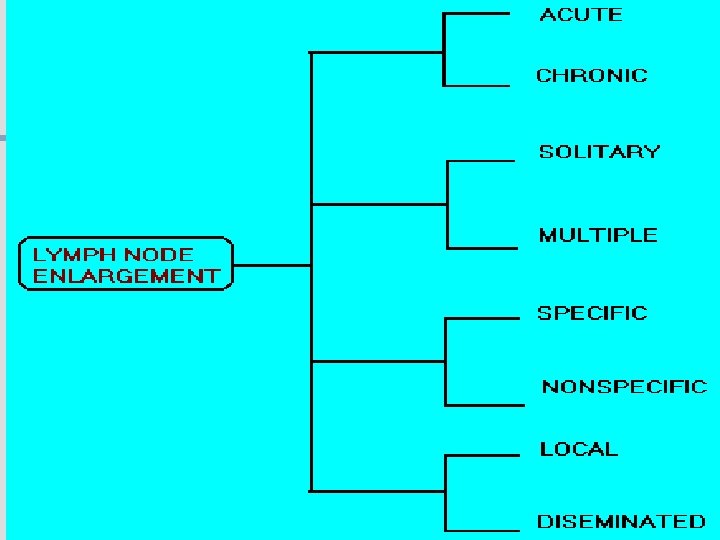
LYMPH NODES a. SITE , b. SIZE , c. NUMBER , d. TENDERNESS e. CONSISTANCY, f. . FIXITY,
INVESTIGATION n n HISTORY CLINICAL EXAMINATION n n TEMP/ DRAINAGE/ DENTAL & MUCOSAL /ENT SPECIAL INVESTIGATION n n n n BLOOD PICTURE CHEST X RAY SEROLOGY KVIEM TEST MANTOUX TEST FNAC / FNAB BIOPSY
FNAC
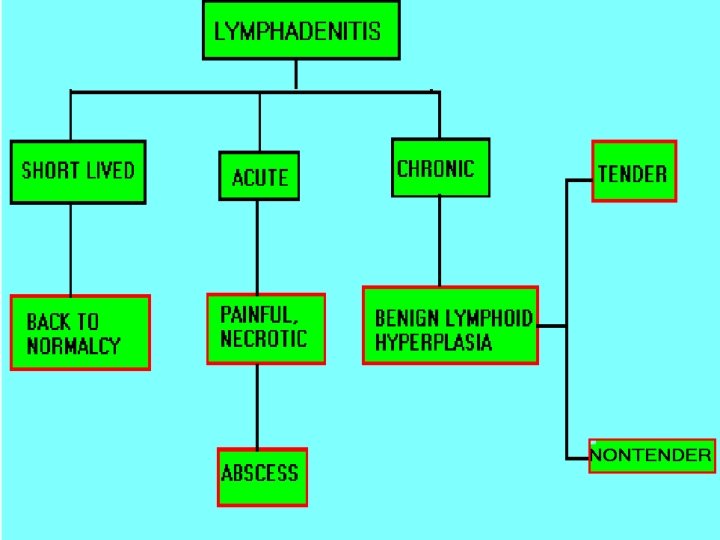
Two distinct types of benign LN enlargement v Non tender v Tender / painful
NON TENDER LYMPHOID HYPERPLASIA v Persistent chronic lymphadenitis or A permanenly enlarged LN after acute or chronic lymphadenitis v LN are solitary, discrete, asymtomatic and freely movable v Submandibular , submental and subdigastric LN
D/D Secondary carcinoma – hard & fixed Management Patient recalled after 2 week & evaluated If doubtful – removal of node & examination
ACUTE LYMPHADENITIS: v Most common pathologic cervical enlargement v Primary infection in oral cavity, nasal cavity , tonsils or Pharynx v Cause painful , swollen nodes in submental, submandibular / subdigastric v Rapid regression of inflammation - nodes Normal & non- palpable
v. SEVERAL NODES MAY BE INVOLVED v. MOVABLE OR FIXED D/D v. LUDWIG’S ANGINA v. INFECTED CYST
MANAGEMENT v When primary infection eliminated Lymphadenitis regress v Adequate doses of antibiotics
METASTATIC CARCINOMA TO CERVICAL NODES v LN are frequent sites v Result of metastatic spread from primary tumors of head & neck v Squmous cell carcinoma is most common tumor spreading to cervical LN v Adenocarcinoma of salivary glands, Scc of skin & melonoma metastasize
v. Lymphatic trunks drain upper extremities & rest of body below clavicles, so solitary metastatic nodes can be from primary tumors of breast, lungs & stomach FEATURES v Usually painless v. Detected on clinical examination v. Feel stony hard & freely movable till they penetrate node capsule & Invade surrounding tissues v. Submandibular & subdigastric nodes most frequent sites
D/D v Fibrosed nodes or nodes undergone non tender lymphoid hyperplasia v Lymphoma (rubbery) MANAGEMENT v Combination of resection, radiation & chemotherapy v Prognosis is guarded
LYMPHOMA A neoplastic proliferation within the reticuloendothelial system that occurs as primry tumor of lymph node
FEATURES v Solitary / multiple v Unilateral / bilateral v Usually rubbery v Advanced cases – patient is ill with fever, TC & DLC may be markedly changed v Other node groups axillae, groin & mediastinum involved
D/D v Multiple & disseminated nodal involvement occur in certain viral diseases & in mononucleosis v Nodes are tender & painful MANAGEMENT v Radiation & chemotoxic drugs