Cervical Dysplasia and Cancer Screening around the Globe

Cervical Dysplasia and Cancer Screening around the Globe UCSD Global Health Elective Suresh Rangarajan Lillian Lai July 2009

Case #1 Ms. Farza is a 45 y/o G 4 P 3 A 1 Iraqi refugee who presents to your clinic with her husband for her first women’s health exam. You notice that she avoids eye contact with you as her husband speaks. Her LMP was 2 weeks prior. He reports that she has not had a history of dysparunia, dysmennorhea or mennorhagia. However, he has noticed blood on his penis after intercourse during the past 3 months. She has never had a PAP smear.

Case #1 questions How would you explain the PAP smear procedure to the husband wife? 2. How could you make the procedure more comfortable for both you and them? 3. Her pap smear is highly suspicious for atypical cells concerning for malignancy. What procedure does she need? 1.

Case #2 Mapala is a 19 y/o G 0 P 0 Sudanese woman who to referred to your clinic by Survivors of Torture for a woman’s health exam. During her escape across the Chad border she was raped multiple times and often had to barter sex to support safe passage for herself, mother and younger brother. She denies vaginal discharge but report lower abdominal pain and mennorhagia. She has never had a pelvic exam. On her O 157 form she is HIV+, RPR-.

Case #2 questions Does her HIV history increase her risk for cervical dysplasia? ► Her PAP reveals ASCUS? What f/u would you recommend? ► Should you give her the HPV vaccine? ►

Case #3 Anupa is 25 y/o G 1 P 0 A 1 Bhutanese female who recently arrived in the U. S. after living in a refugee camp on the Nepali-Bhutanese border for the past 17 years. She reports treatment for Chlamydia infection in the past but no history of a PAP. She is concerned as her mother died of breast cancer and grandmother died of cervical cancer in the camp.

Case #3 questions Her PAP reveals AGUS? Would you test her for HPV? 2. What other lab work, tests or procedures does she need? 3. Should you give her the HPV vaccine? 1.

Learning Objectives ► Understand prevalence of the global HPV epidemic and cervical screening patterns worldwide ► Understand the pathogenesis and HPV infection with cervical cancer and indications for the HPV vaccine ► Learn to adjust woman’s health exam to be culturally sensitive to refugee populations ► Classify cervical dysplasia and cancer and direct appropriate treatment and follow-up
 www. cdc. gov")
Incidence rate of Cervical Cancer by State, 2005 (per 100, 000) www. cdc. gov
 International Association of Cancer Registries, 2002")
Incidence of Cervical Cancer Worldwide (per 100, 000) International Association of Cancer Registries, 2002

HPV Screening in Limited Resource Settings NEJM April, 2009: HPV Screening for Cervical Cancer in Rural India by Sankaranarayanan et al. ► Cluster-randomized control trial of ~130, 000 women between 30 and 59 yo in India. ► Randomly assigned to 4 groups: HPV testing, pap smear (cytologic testing), colposcopy (a. k. a. visual inspection of the cervix with acetic acid ~VIA), or standard care (control). ► Women with positive results on HPV underwent colposcopy and directed biopsies. Women with cervical lesions received appropriate care. ►
 Reduction in number of")
HPV Screening for Cervical Cancer in Rural India § 1) Reduction in number of advanced cancers in HPV group: 0. 47 hazard ratio (95% CI 0. 32 -0. 69) § 2) Reduction in number of deaths in HPV group: 0. 52 hazard ratio (95% CI 0. 330. 83) § 3) No significant reductions in advanced cancers or deaths in cytologic-testing or VIA groups compared with control group.

HPV Screening for Cervical Cancer in Rural India

HPV screening alone is as good as pap smear with HPV reflex testing overtime

Implications of NEJM study ► Results: In a low-resource setting, a single round of HPV testing was associated with a significant reduction in the incidence of advanced cervical cancer and cervical-cancer mortality, whereas pap smear and VIA were not. ► Implications: § Low-resource countries should implement widespread HPV testing. § Screening with pap smears or VIA have not been shown to be beneficial.

Cervical Cancer ► 2 nd most common cancer among women in developing countries. ► Linked to HPV § HPV shown to cause cervical cancer in humans through long-term cross-sectional and casecontrolled studies, as well as in vitro studies. § HPV 16 and 18 (45, 31) account for 50% and 20% of cervical cancers worldwide § HPV 6 and 11 cause >12% of LGSIL and 80% of genital warts.

Cervical Cancer ► Risk Factors; § Early onset of sexual activity § Multiple sexual partners § High-risk sexual partner § History of sexually transmitted diseases § Smoking (not adenocarcinoma) § High parity § Immunosuppression § DES in utero § Low socioeconomic status § Hx of vaginal or vulvar cancer

Epidemiology of Cervical Cancer ► About 75 -90% of infections clear within one year. ► Bimodal peak incidence in women ages 1520, and 40 -50 years old. ► Conventional model of cervical cancer prevention based on repeated cervical exams/pap smears, colposcopy (small blue arrows) and HPV screening.

HPV and Cervical Cancer

HPV Vaccine ► Adolescents and Woman under 26 years ► Reduce incidence of dysplasia and cervical cancer ► Are safe to use in immunocompromised persons
 ►No virus-associated ds. RNA to stimulate")
Weak Immune Response ►Little tissue destruction (no cytolysis) ►No virus-associated ds. RNA to stimulate immune response ►Only infects epithelial cells (antiinflammatory environment in epithelium) ►Depletion of antigen-presenting cells (APC’s) and interferon

Natural Antibodies ►L 1 major capsid protein: 4 -5 months after first infection but only in 50 -60% of women ►E 7: only with invasive cervical carcinoma ►Effect seen through CD 8 T-cell mediated toxicity

Recombinant DNA Technology ►L 1 protein expression by eukaryotic cells--> reassemble into virus-like particles (VLP) ►VLP elicits strong antibody response directed against genotype specific amino acids in L 1 peptide chain. NOT infectious. ►VLP + adjuvant--> immune response

Available HPV Vaccines

Who to Vaccinate? WHO Bulletin 2009 Ø Countries with limited/no screening and low access to treatment: can reduce cervical cancer deaths but current pricing is $100 per dose so arguably screening is still more cost-effective if available. Ø Pre-adolescent girls? Definitely. Current catch-up program will possible shorten time for impact of vaccine to be seen. Ø Older women? Most have been exposed to HPV and generate lower antibody titers to vaccine. Ø Previously infected individuals? Prophylactic HPV vaccines not shown to have therapeutic effects against pre-existing HPV infections/lesions. Could potentially E 6 and E 7, proteins that are expressed early in cells infected by HPV, to generate cellular immunity. (Expert Opinion Biolog. Therapy, 2008 Apr; 8(4): 421 -39. ) Ø Males? Cervical cancer affects women though so might be more cost-effective to just target women.

Dysplasia and HPV ► Infection ► 16, with high risk strains 18, 31, 33, 39, 45, 51 ► Spectrum of HPV; ►Condyloma Acuminata ►Cervical Dysplasia ►Cervical Cancer ACOG website
 Guidelines for Cervical Cancer Screening ► Start Pap screen at")
ACS (American Cancer Society) Guidelines for Cervical Cancer Screening ► Start Pap screen at 21 yo, or 3 years after onset of sexual intercourse. Continue with annual screening. ► Reduce screening to every 2 -3 years for women over 30 yo with 3 consecutive normal Paps. Exceptions are those with +HPV or weakened immune systems, who should be annual screened. ► Discontinue screening for women over 70 yo with 3 consecutive normal Paps and no abnormal pap smears in last 10 years. ► Discontinue screening for women s/p hysterectomy for benign disease. Those with cancer must be screened.

Culturally Sensitive Techniques for Women’s Health Exam ► Describe what you are going to do and while you are doing it ► Do not make direct eye contact with patient ► Place screen between yourself and patient ► Have husband and/or translator stand behind the screen and address them, not the patient ► Do not convey results or make comments during the exam, particularly questions regarding female genital mutilation
 ► Squamous ► Atypical Cell squamous cells (ASC) § Undetermined Significance")
Bethesda Classification (2001) ► Squamous ► Atypical Cell squamous cells (ASC) § Undetermined Significance (ASC-US) § Not exclude High Grade (ASC-H) ► Low Grade Squamous Intraepithelial lesion (LSIL) ► High Grade Squamous Intraepithelial lesion (HSIL) ► Squamous Cell Carcinoma ► Glandular Cell ► Atypical Glandular cells (AG) § Undetermined Significance (AG-US) § Favors Neoplasm ► Adenocarinoma In ► Adenocarcinoma Situ (AIS)

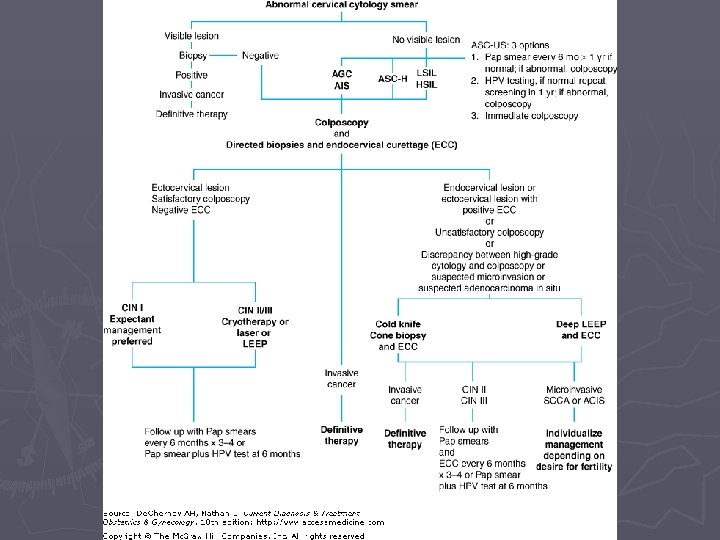
Management of Cervical Dysplasia ► Squamous Cells; § ASCUS ►HPV testing (+ refer, - repeat Pap) ►Repeat Pap in 6 months, if normal, no referral. ►If repeat Pap abnormal, Colposcopy & Cx Bx. ►If HSIL, treat with excision (LEEP) or ablation (cyrotherapy). § ASC-H ►HPV test, Colposcopy, Cx Bx & Endocervical Bx. ►If HSIL, treat with excision or ablation.

Management of Cervical Dysplasia ► Squamous § LSIL Cells ► In adolescents, just repeat Pap q 6 -12 months. ► Non-adolescent, HPV test, Colposcopy & Cx Bx. ► If LSIL, repeat Pap 6 -12 months. ► If HSIL, treat with excision (LEEP) or ablation. § HSIL ► HPV test, Colposcopy, Cx Bx, & Endocervical Bx. ► If HSIL present, excision (LEEP) or ablation (cryotherapy).
 and CIN (histology) correlates")
SIL (cytology) and CIN (histology) correlates

LSIL as seen on Colposcopy

HSIL as seen on Colposcopy High grade lesion with coarse punctation at anterior lip of the cervix

CIN 2, biopsy confirmed

Management of Cervical Dysplasia ► Glandular Cells; § AGUS ►HPV screen (give vaccine if negative), Colposcopy, & Endometrial Biopsy, and pelvic ultrasound to evaluate uterus and fallopian tubes § Adenocarcinoma in situ ►Colposcopy, Endocervical & Endometrial Biopsy ►Diagnostic Excisional Procedure (“Conization”)

Loop Excisional Biopsy Uses a thin wire on an insulated handle through which electrical current is passed. ► Multiple pass LEEP shown on right for bulky tumors. ► Local anesthesia ► Tissue specimen for histology. ► Can cause thermal damage to vaginal side wall and obscure margins ►

Cold-Knife Conization ► Removal of entire cervical transformation zone with cervical lesion by scalpel ► Operating room: requires general or regional anesthesia ► Preferred for unsatisfactory colposcopy when CIN extends deep into the endocervical canal, or older patients with high-grade lesions. ► Higher risk of hemorrhage
 §")
Immunocompromised Women ► PAP yearly regardless of age ► ASCUS/LGSIL (adolescents or adults) § Colposcopy with repeat colposcopy q 6 month x 2 and then annually if normal ► HGSIL § Excisional or ablative procedure; repeat colposcopy q 6 month x 2 and then annually if normal ► AGUS § HPV screen (give vaccine if negative), Colposcopy, & Endometrial Biopsy, repeat colposcopy q 3 -6 month for one year minimum ► Adenocarcinoma in situ § Colposcopy, Endocervical Biopsy § Diagnostic Excisional Procedure (“Conization”)

Cervical Cancer ► Signs & Symptoms; § Abnormal Vaginal Bleeding § Postcoital Bleeding § Vaginal Discharge (watery, mucoid, purulent, malodorous). ► Types of Cervical Cancer; § Squamous Cell Cancer § Adenocarcinoma (Glandular)
 ► 0 ►I ► II Carcinoma in situ. Cervix")
Staging of Cervical Cancer (FIGO) ► 0 ►I ► II Carcinoma in situ. Cervix carcinoma confined to uterus. Cervix carcinoma invades beyond uterus but not to pelvic wall or to the lower third of vagina. ► III Tumor extends to pelvic wall and/or involves the lower third of vagina, and/or causes hydronephrosis or nonfunctioning kidney. ► IV Tumor extends beyond true pelvis or has involved bladder or rectum

Invasive Cancer
 § Radical Hysterectomy plus")
Treatment of Cervical Cancer ► Early Stage (I – II) § Radical Hysterectomy plus pelvic/paraaortic lymphadenectomy with or without adjuvant chemoradiotherapy. § Radiation Therapy. **Depends on age, childbearing, disease stage, comorbidities, patient & physician preference.
 § Primary Radiation")
Treatment of Cervical Cancer ► Locally Advanced Disease (II – IV) § Primary Radiation Therapy with concomitant chemotherapy (cisplatin, 5 FU is second line).

Cervical Cancer Follow Up… ► Follow Up; § Clinical evaluation every three months for one year, every four months for one year, every six months for three years and then annually. § Annual chest x-ray. § Other radiographic images (CT, PET scan), as clinically indicated ► Clear translation and arranging transportation are essential for refugee populations

Summary ► Global disparities in cervical cancer and HPV screening and incidence are real ► HPV screening models may be more costeffective than traditional PAP smears ► HPV vaccine should be given when indicated ► Cultural sensitivity can be improved with practical steps ► Follow-up for cervical dysplasia is critical
- Slides: 47